I take colchicine .6-1.2mg/day for Behçet’s and know many of you do for cardiac protection as well.
My concern is whether colchicine, a known neurotoxin, is actually a risky drug with respect to long-term effects on the brain.
As I understand, colchicine is a neurotoxin which induces Alzheimer’s in rats when injected into the brain. This is uncontested and the subject of many papers. However, we assume that it does not cross the blood-brain barrier because in overdoses from systemic exposure, death occurs from organ failure not direct CNS poisoning. However, from what I can tell, there is precious little actual evidence that colchicine definitely does not cross the BBB, OR that the limited extent it does, even if negligible in an overdose event, could cause cognitive effects over long-term usage (consider daily usage over 50-70 years) or even lead to Alzheimer’s later on.
What do we think of this: safe for daily use over years and decades, or questionable if your main priority above all else is neurological health and brainspan?
After our systematic review, we selected 125 low potency (Score 1) anticholinergic drugs (Table 1), 28 drugs with medium potency (Table 2) and 62 drugs with high anticholinergic potency (Table 3). Of these, colchicine was ruled out, as one author rated this drug with a score of 1 or 3 [46], another scale rated it as discrepant (Disc) and two scales explicitly rated it with a null anticholinergic score [42,48].
The evolutionarily conserved Hippo (Hpo) pathway has been shown to impact early development and tumorigenesis by governing cell proliferation and apoptosis. However, its post-developmental roles are relatively unexplored. Here, we demonstrate its roles in post-mitotic cells by showing that defective Hpo signaling accelerates age-associated structural and functional decline of neurons in C. elegans. Loss of wts-1/LATS resulted in premature deformation of touch neurons and impaired touch responses in a yap-1/YAP-dependent manner. Decreased movement as well as microtubule destabilization by treatment with colchicine or disruption of microtubule stabilizing genes alleviated the neuronal deformation of wts-1 mutants. Colchicine exerted neuroprotective effects even during normal aging. In addition, the deficiency of a microtubule-severing enzyme spas-1 also led to precocious structural deformation. These results consistently suggest that hyper-stabilized microtubules in both wts-1-deficient neurons and normally aged neurons are detrimental to the maintenance of neuronal structural integrity. In summary, Hpo pathway governs the structural and functional maintenance of differentiated neurons by modulating microtubule stability, raising the possibility that the microtubule stability of fully developed neurons could be a promising target to delay neuronal aging. Our study provides potential therapeutic approaches to combat age- or disease-related neurodegeneration.
Purpose: We aimed to investigate the effects of colchicine, an important anti-inflammatory agent, on cognitive functions in a geriatric population diagnosed with gout or osteoarthritis by comparing it to non-colchicine users. Methods: 138 geriatric patients (67 colchicine users and 71 non-users) were enrolled. Within comprehensive geriatric assessment (CGA), cognitive status assessment via Mini-Mental State Examination test (MMSE), Quick Mild Cognitive Impairment Screening test (Qmci), clock drowning test (CDT), and digit span tests were performed. Results: Median age was 68 (65-72), and there were 82 female (59.4%) patients. The scores of CDT, Backward Digit Span Test, MMSE-Total, MMSE-Attention, MMSE-Motor Function, Qmci-Total Score, Qmci-Clock drawing, and Qmci-Logical Memory were significantly higher in the colchicine user group (p < .005), showing better cognitive function. Adjusted model analysis showed that colchicine usage is independently correlated with higher Qmci-Total Score and Qmci-Logical Memory Score (For Qmci total score β = 7.87 95%CI = 5.48-10.27, p = <0.0001, and for Qmci Logical memory score β = 3.52, 95%CI = 2.12-4.91, p = <0.0001). Conclusion: To the best of our knowledge, this is the first study revealing that colchicine usage is associated with better cognitive performance in older adults. Further investigations with a prospective, larger-sampled and randomized design are needed to show the causal relationship between colchicine and cognition.
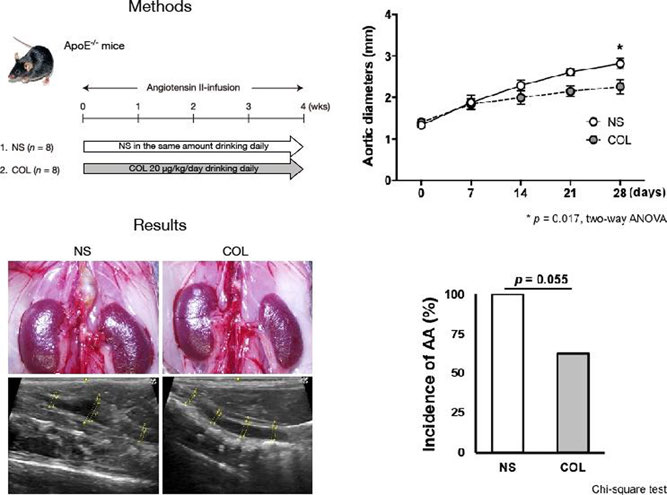
In vivo: Aortic diameter measured by echography every week was significantly suppressed in the COL group (2.25 vs 2.81 mm, p<0.05). The incidence of AA was decreased in the COL group (62.5% vs 100%). COL significantly suppressed the degeneration of aortic elastin in EVG staining (p<0.05).
@Beth NAD but my instinct is that there are a LOT of options for cardioprotection. So why choose colchicine if there are other options? There just aren’t a lot of options for Behçet’s. That said, I’m up to 3/day and perhaps going to 4 which is 1.8-2.4mg/day at 95 lbs. I think the dosing for cardioprotection is generally lower so whatever long-term effects might be of concern would be reduced. If you’re worried about it you might ask your doctor what the lowest dose is to see a benefit or ask if you can take half a pill.
That is really helpful and it never occurred to me to potentially have a half dose. I’ll check in with my cardiologist about that. Especially considering I’m taking 6mg and the dosage for cvd prevention is 5mg (6mg is super cheap)
The dosage is 0.5 mg/day, which is so low that very little colchicine would cross the blood-brain barrier. Are you also taking a P-gp inhibitor like telmisartan or verapamil?
Backgound: Colchicine is widely used for treating gout and familial Mediterranean fever. However, studies in animal models have reported ill effects of colchicine on the central nervous system, including cognitive function.
Objectives: To evaluate the cognitive status of elderly FMF patients on long-term colchicine treatment.
Methods: The study group consisted of 55 FMF patients aged 74 ± 5, attending an FMF outpatient clinic and receiving colchicine treatment for 25.1 ± 8.9 years. The Mini-Mental State Examination was used for cognitive evaluation. Patients’ scores were compared with accepted age- and education-adjusted cutoff scores, population-based norms, and scores of a matched control group of 56 subjects.
Results: Individually, all colchicine-treated FMF patients scored well above the age- and education-corrected cutoff scores. Overall, there was a large difference, 5.0 ± 1.6, from the expected cutoff points, in favor of the study group scores (P < 0.001). The individual scores of the control group were also above the cutoff points, however with a lower but still statistically significant difference (3.71 ± 1.15 points, P < 0.001). Compared to population-based norms adjusted by age and education, the study group had significantly higher mean MMSE scores (27.2 ± 2.2 vs. 25.5 ± 2.4, P < 0.001). The control group’s scores were also somewhat higher than expected, but not significantly so.
Conclusions: Our results do not support the view that prolonged colchicine treatment may be associated with cognitive impairment. On the contrary, it is possible that long-term colchicine treatment may even confer protection against cognitive decline in patients with FMF.
@Cohen thanks for that, and for the last paper you linked too! I tend to read the research as well but never saw this one on FMF patients and it’s super reassuring because they are quite similar to us. I would think those improvements are probably related to controlling the disease course and inflammation.
In this study, we aimed to determine new target proteins that contribute to the superior clinical efficacy of clozapine over olanzapine by identifying and comparing proteins that bind to clozapine and olanzapine. We identified α and β tubulin heterodimers as novel clozapine‐binding proteins. In addition, we observed that clozapine inhibits tubulin polymerization and affects the microtubule network in HeLa cells.
Ten isoforms for the α subunit and nine for the β subunit of tubulin are expressed in human neural tissues 13 . They undergo various post‐translational modifications 14 and are regulated by various microtubule‐binding proteins represented by traditional microtubule‐associated proteins (MAPs) 15 to form microtubules. As a main component of the cytoskeleton, microtubules play a central role in various cell functions 16 . In the nerve tissue, they are involved in the morphogenesis and maintenance of neurons and axonal transport 17 . Recently, it has been reported that microtubules may be involved in psychiatric disorders, including schizophrenia 18 . Gene set enrichment analysis using the term “microtubule regulation and disease” in the MetaCore database (Thomson Reuters) showed high enrichment for schizophrenia and schizophrenia spectrum disorders, and genes with altered mRNA expression in these disorders included α and β tubulin isoforms (eg, TUBA1A, TUBA8, and TUBB2B), MAPs (eg, MAP1A, MAP1B, MAP2, MAP6, FEZ1, DPYSL2, PCM1, and APC), and microtubule‐based motor proteins (eg, KIF2A, KIF21A, NDE1, and NDEL1) 19 . A detailed review found that the mRNA and protein expression levels of tubulin isoforms and their post‐translational modifications differ between disease and control groups for both humans and animal models of schizophrenia18 . In addition, the qualitative and quantitative changes of microtubule‐binding proteins, such as MAP2, DPYSL2 (also called CRMP2), and DISC1, in schizophrenia and related psychiatric diseases have been described 18 . A comparison of microtubules in neuronal cells in patients with schizophrenia and control subjects was performed using olfactory neuronal precursors, and alterations in microtubules were observed 20 . Neuronal precursors derived from patients with schizophrenia not treated with antipsychotics have a higher ratio of polymerized tubulin than controls. In contrast, the cells from patients treated with antipsychotics have a ratio of polymerized tubulin similar to that of the controls 20 . This finding is supported by another study in which the microtubule network in cultured olfactory epithelial‐derived cells was more stable in the presence of the microtubule‐destabilizing agent nocodazole in patients with schizophrenia than in healthy controls 21 . However, in the above study, all patients with schizophrenia received antipsychotics 21 . From these findings, it is assumed that microtubules are over‐stabilized in the neuronal cells of patients with schizophrenia and that antipsychotic drugs partially re‐establish these over‐stabilized microtubules. Microtubules are highly dynamic structures, particularly in neuronal growth cones 22 and dendritic spines 23 . Therefore, the dynamic properties (ie, “dynamic instability”) of microtubules are considered important for neural plasticity. We propose that clozapine acts on over‐stabilized microtubules in the brains of patients with schizophrenia to recover the “dynamic instability” of microtubules. If this is the case, it may be possible to improve the therapeutic effects of pharmacological treatment of schizophrenia using microtubule‐destabilizing agents in addition to antipsychotics. Currently, davunetide, a microtubule stabilizer, is in clinical trials for the treatment of schizophrenia 19 ; however, no microtubule destabilizer has been investigated to date. Microtubule destabilizers, such as colchicine and nocodazole, are commonly used in the treatment of cancer and gout and expertise on their safe usage has accumulated; thus, they can now be repositioned for the treatment of schizophrenia.