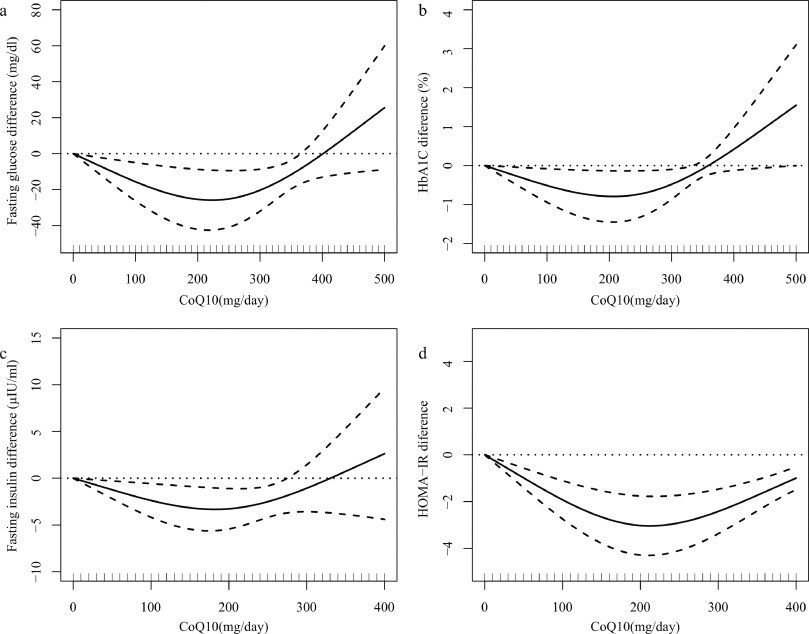
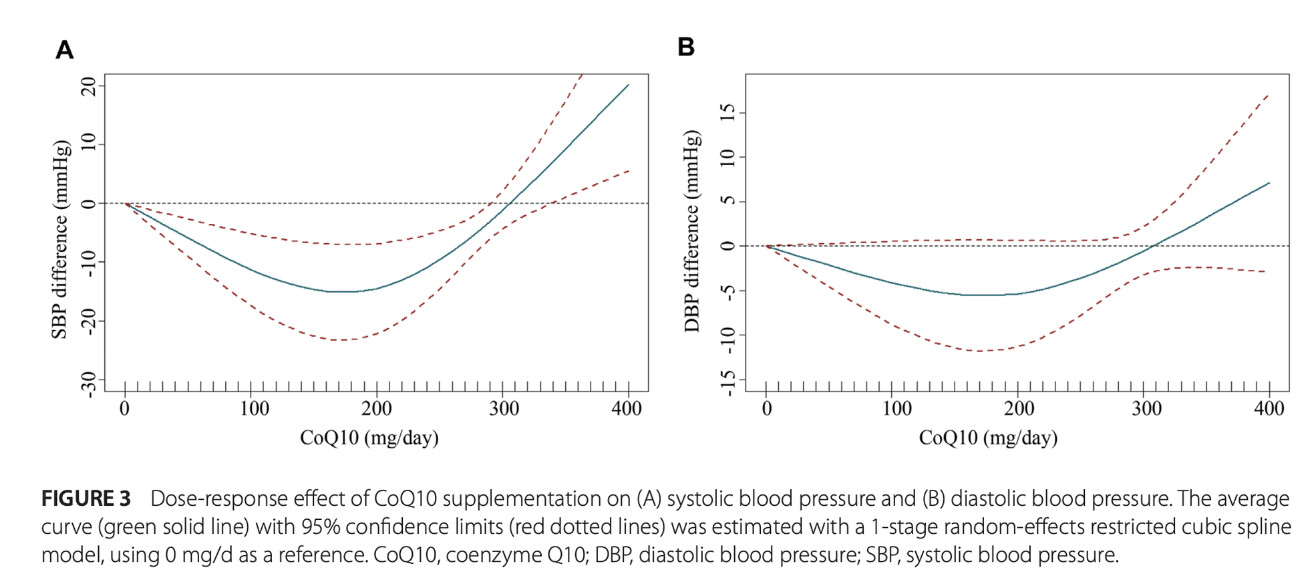
I found these meta-reviews and thought some here might be interested. Looks like for CoQ10, the dose makes the poison… The optimum seems to be around 100-200 mg/day: but is it the same for all people? Does it depend on your gender? weight? race? How do you make sure you don’t take too much?
Not sure for all impacts of Co-Q10, but for glucose and blood pressure it seems that N=1 measurements before and after each adjustment of dose of time could help dial in the dose.
Do you like Co-Q10 outside of “take with a statin” contexts? For neuroprotection?
So, I wondered whether low-dose Q10 could be better for neuroprotection. And these U-shape curves signal it could be the case. 100 mg/d is probably the safest bet. At worst useless, at best maximizing the positive effects on BP and glucose
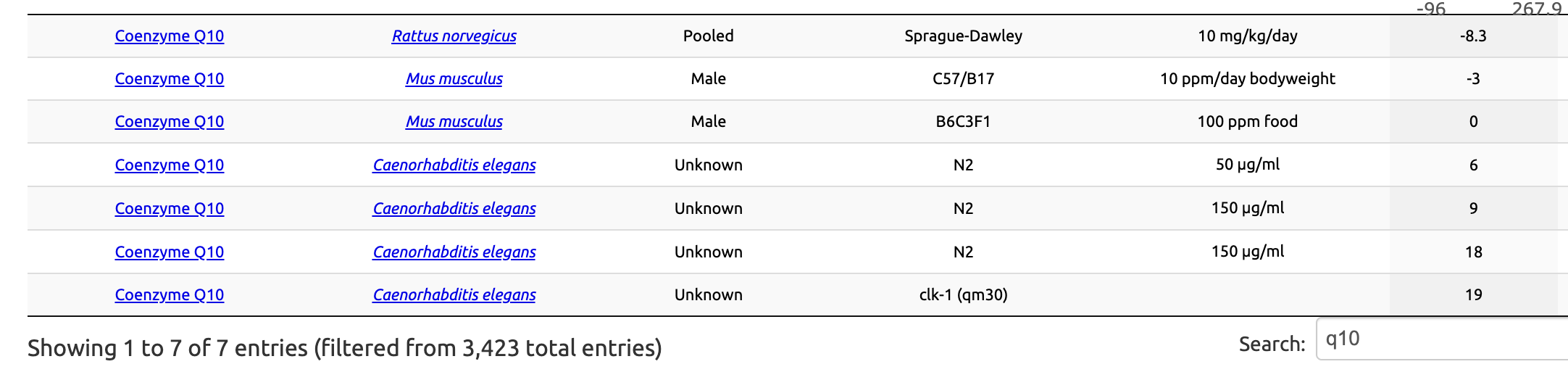
Removing Q10 from worms also makes them live longer: x.com
After all this time we would know if Q10 was that good. The U curves for BP, glucose, lipids, and inflammation markers also make it hard to choose a dose.
I don’t know. I have it on my list of things that may have an effect on the ETC. I am certain that menaquinone-7 does the job because it disrupts sleep.
I take it when I am taking all the AMPK activators etc. Whether it helps, hinders or does nothing much I don’t know.
Do you think 300mg every other day is safe because the costco 300mg softgels are cheaper than 100 or 200mg? It looks like half life is 33+ hours so thats pretty good…
Agreed. At best, CoQ10 has a role to play in mitigating statin side effects but you don’t need big doses for it as the human body produces less than 1mg of it per day naturally.
I am not persuaded that CoQ10 is a magical molecule, but would be interested in seeing the basis of the calculations. I think the calculations on melatonin are some distance out. Working out the dosage to move the needle on endogenous metabolites is complicated.
The HED calculations? They’re just using the FDA conversion factors. It’s a good rule of thumb that gives the order of magnitude but there are then many details for each compound based on their bioavailability and specific pharmacokinetics. Still, we know that at high doses, Q10 can be deleterious in animal models. So finding the right dose in humans isn’t easy.
It would be nice to have some links, but either way I don’t think it is a magic solution. I do take CoQ10 when I take my ATP boosting combination, but generally that does not seem to have as much of an effect as other things,
One simple difficulty is that an improvement in cellular function takes a while (days and weeks normally) to be visible in the phenotype.
I’m going to play a bit of devils advocate here and stick up for CoQ10. First, see my links above on CoQ10 + Selenium in combination
We know CoQ10 declines in heart failure
Here is a 2021 Cochrane review of it being helpful in heart failure. It’s not slam dunk evidence, but I think there is enough here that anyone with heart failure should be taking a decent amount of it
Here is AI’s interpretation
“Research indicates that CoQ10 supplementation may lead to reduced all-cause mortality and heart failure-related hospitalizations. Specifically, a meta-analysis reported an absolute risk reduction of 7.5% for mortality and 10.5% for hospitalization in patients receiving CoQ10 . The most notable evidence comes from a double-blind randomized controlled trial involving 420 patients, which found that those taking CoQ10 had a significantly lower risk of major adverse cardiovascular events compared to a placebo group.”
I don’t know if people with healthy hearts really need it. For people with compromised hearts, however, I think they should be taking it.
They looked at “elderly Swedish population low in selenium” and gave them selenium + CoQ10 and concluded it was good. Are you old? Low in selenium? Do we know if the positive outcome was due to selenium, CoQ10, or the combination? Would you get the same outcome with selenium + Nutella?
No, no, no. NOT AT ALL. They conclude:
In 2013, the American College of Cardiology Foundation and the American Heart Association recommended against the use of nutritional supplements (including coenzyme Q10) for the treatment of heart failure.5 The 2017 update to this practice guideline did not address coenzyme Q10. The approximate cost of a one-month supply of the 200-mg dose of coenzyme Q10 is $10.6 At this time, there is insufficient evidence to support, or refute, the use of coenzyme Q10 in patients with heart failure.
The included studies provide moderate‐quality evidence that coenzyme Q10 probably reduces all‐cause mortality and hospitalisation for heart failure. There is low‐quality evidence of inconclusive results as to whether coenzyme Q10 has an effect on the risk of myocardial infarction, or stroke. Because of very low‐quality evidence, it is very uncertain whether coenzyme Q10 has an effect on either left ventricular ejection fraction or exercise capacity. There is low‐quality evidence that coenzyme Q10 may increase the risk of adverse effects, or have little to no difference. There is currently no convincing evidence to support or refute the use of coenzyme Q10 for heart failure. Future trials are needed to confirm our findings.
Coenzyme Q10 (CoQ10) naturally occurs in small amounts in organ meats and oily fish and is a cofactor in many biological pathways including oxidative phosphorylation. Because HF results in an ATP-depleted state, exogenous administration of CoQ10 has been hypothesized to result in metabolic benefit. Researchers found modest benefit with CoQ10 supplementation by improving LV ejection fraction and quality of life in small-scale studies. In the largest randomized trial of CoQ10 in 420 patients with HF, Q-SYMBIO (Coenzyme Q10 as Adjunctive Treatment of Chronic Heart Failure With Focus on Symptoms, Biomarker Status [Brain-Natriuretic Peptide], and Long-Term Outcome [Hospitalizations/Mortality]), CoQ10 treatment was not associated with any significant changes in 6-minute walk distance, or N-terminal pro-B type natriuretic peptide levels compared with placebo, but was associated with a significant improvement of New York Heart Association functional class and reduction in major adverse cardiovascular events at 2 years (hazard ratio [HR], 0.50 [95% CI, 0.32–0.80]; P=0.003). Furthermore, in a more recent literature analysis, CoQ10 treatment was associated with a reduction in all-cause mortality. However, larger-scale randomized-controlled trials are needed before any definitive conclusion can be reached. Therefore, CoQ10 supplementation remains of uncertain value in HF at this time.
Many trials were reported poorly and were rated as having a high or unclear risk of bias in at least one domain. Meta-analysis suggested a possible benefit of coenzyme Q10 on all-cause mortality (seven trials, 1371 participants; relative risk 0.68, 95% confidence interval 0.45 to 1.03).
Available evidence suggested that, if prescribed, coenzyme Q10 has the potential to be clinically effective and cost-effective for heart failure with a reduced ejection fraction. However, given important concerns about risk of bias, plausibility of effect sizes and applicability of the evidence base, establishing whether or not coenzyme Q10 is genuinely effective in a typical UK population is important, particularly as coenzyme Q10 has not been subject to the scrutiny of drug-licensing processes. Stronger evidence is needed before considering its prescription in the NHS.
Conclusions:
CoQ10 lowers lifespan in mice and rats at human equivalent doses >60 mg/day. (This does NOT mean that at these doses in humans CoQ10 would also lower lifespan: we don’t know.)
CoQ10 is not proven to improve outcomes in humans with heart failure.
There might still be a case for CoQ10, but the above two points are undeniable facts (that could still change, for instance, if a future RCT finds benefits from CoQ10 in heart failure or another condition).
I have looked into CoQ10 many times over the years, including because I take statins. However I could never find a solid case for it. I’m glad for the people who find it helpful, but personally I can’t fit it into my stack.
Back on the CR list many years ago, there was a discussion of it that reached the conclusion that it has more harmful potential than helpful, but I don’t remember the details, unfortunately. If I find that thread I’ll post it here.
One rule of thumb I go by is that if there are many conflicting studies, and the supp doesn’t move the needle significantly either way, it’s not worth bothering about. Think of smoking - there are not many conflicting studies, they all pretty much go in one direction (PD excepted). And it’s not a small effect. OK, no smoking for me. But if it’s some supplement that’s been around for decades, and there’s still no clear effect either way, just endless waffling in multiple studies, I figure I’m not missing something vital here.
Meanwhile we have a situation here where the margins between possibly harmful doses and doses that might be speculatively beneficial are too narrow. I don’t like the risk/benefit ratio here. There are no compelling benefits shown which would justify the risk of wrong dose.
So, for me it’s a pass, but of course if it works for someone that’s fantastic. YMMV.