True… and I’m not familiar with any natural ways to maintain it or prevent a decline at any given age.
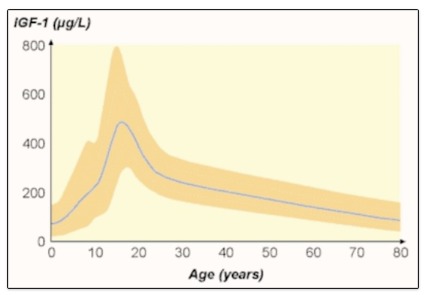
Source: Growth Hormone in Aging
True… and I’m not familiar with any natural ways to maintain it or prevent a decline at any given age.
Source: Growth Hormone in Aging
@DeStrider An important question. I would point to declining adaptive homeostasis as a clue. My hypothesis is training my body to restore its ability to react and adapt to changes in my environment and activity level and diet will make my body operate as if I was younger. Maybe that’s not as good as being younger (many other processes to address) but it’s a good start.
Here is a paper on the subject
I will be publishing an interview with Mike T Nelson PhD on this exact topic soon. Dr Mike is the creator of the Metabolic flexibility and Physiologic flexibility programs which operate along these lines.
I agree with your hypothesis. I believe that we can chose to “compete” directly with our younger self as we age. That competition is unique to the individual but adaptive to a range of physical and mental activities. Any human activity (dancing, card games, running, birding, musical instrument, strength training, clipping toe nails, etc etc etc) can be adapted to within the aging process and probably key to healthy aging. The older one is, the more important this adaptation is to remaining robust.
As it applies to hormonal health, it probably means one continues activities that exposes us to sunlight, and circadian rhythm. As one becomes less adaptive people very slowly but profoundly see themselves as fragile and taking less risk and exposure to the natural environment.
Additionally, even though the range of medicines available to extending one’s life have been important to mitigating modern lifestyle morbidities (diabetes, heart disease), those same medicines are notably responsible for declines in hormones (testosterone) and mitochondrial dysfunction (metformin).
I still drive my motorbike (at age 70) to give one example. Generally, every spring, I note the news reports of motorcycle accidents. Often times it is a guy at upper middle-age who is found in a field after taking a curve on the highway. I always wonder what happened. Did they forget how to ride over the winter? Or did they reach an age where they just don’t have the skills to lean the bike over and judge the physical dynamics required to take that curve? Anyways, I am always considering my own judgement and capabilities when taking a curve with my motorbike. At my age the consequences of a crash are much more dire to recovery, but so is giving up a skill I have had throughout my life. (I do a lot of different and evolving things now to mitigate risk as I age, that accompany my activities.)
“As it applies to hormonal health, it probably means one continues activities that exposes us to sunlight, and circadian rhythm”
Yes. Agreed. The amplitude of our circadian rhythm declines as we age. As a kid I would play hard and sleep hard. When I woke up naturally I felt reborn…renewed. If I stayed up late I would crash and burn. Now, after years of learning how to be productive all the time and get by on little sleep, I’m stuck in that self-made rut. I’m rarely naturally tired and almost never at full power. And probably losing out on important hormone production.
Sleep is the tough one to solve but light, food, temperature, and mental (“thethethe” mantra) discipline plus breathing skills help. Earning my sleep (using my body hard) and not using stimulants during the day is key for me.
This needs to go on the rapamycin.news best quotes of all time list.
“yet”
I recently switched to dutasteride after being on finasteride for about 2.5 years. I’ve noticed no difference, no side effects. I’d just recommend most people hop straight on dutasteride at this point, the side effect profile is essentially the same as finasteride.
Glad to hear you’ve had no issues. I just switched in the past week after a little over two years on fin. Planning to take them concurrently for a week or two and then I will taper down the fin dose until I’m just on dutasteride.
Many people on Reddit report having no sides from dut whereas they had sides from fin, which I find pretty interesting and suggestive that androgen antagonism is not the issue for everyone. Finasteride inhibits an enzyme that converts norepinephrine to epinephrine, for example.
Dutasteride is a more selective molecule (w.r.t to 5ARi vs off-target) due to its increased potency, so at least for androgen-independent sides it would be superior.
Interesting, I didn’t know that about epinephrine. Need to read more about it. Yeah, i have nothing but positives to report. I switched cold turkey, too.
FYI: Finasteride and dutasteride users interested in neuroprotection might prefer to abandon these drugs: Terazosin / doxazosin / alfuzosin may protect against dementia with Lewy bodies
When things aren’t optimal and you have no levers to pull to fix it, then supplement to normalize whatever is abnormal and measure it periodically.
Dutasteride inhibits more 5ar enzymes than finasteride though.
By blocking these enzymes, 5AR inhibitors decrease the serum concentration of dihydrotestosterone, inhibiting prostatic growth3 and decreasing disease progression.2 Two 5AR inhibitors are available: finasteride and dutasteride. Finasteride is a selective inhibitor of the type 2 isoenzyme, whereas dutasteride inhibits both type 1 and type 2.4 This difference in mechanism results in a significantly greater and more consistent reduction in dihydrotestosterone with dutasteride than with finasteride4,5
The anecdotes on reddit can easily be explained by a) more people being on finasteride than on dutasteride and b) finasteride being fearmongered to death by the litigious PFS organization (that has failed repeatedly in court with the FDA even explicitly saying that there is no evidence of persistent side effects after cessation) which causes the anxiety-ridden redditors to nocebo themselves into experiecing all sorts of side effects. The same effect can be observed on the supplements subreddit.
Finasteride inhibits an enzyme that converts norepinephrine to epinephrine, for example.
This is based on ex-vivo and animal studies using high doses of finasteride and dutasteride would certainly also cause that effect due to also inhibiting 5ar2 and 5ar3.
As usually, associations do not equal causations. And to date, there is no strong signal either way of 5ar inhibitors increasing the risk of alzheimers or other neurodegenerative diseases. And is there a reason why terazosin couldn’t be used in addition to 5ar inhibitors?
The case for terazosin is strong. But yes, it doesn’t mean that 5-ARIs are neurotoxic. And yes, they can be combined.
Yes, and it does so more potently, so the expectation is greater selectivity than finasteride for non-5AR targets.
which causes the anxiety-ridden redditors to nocebo themselves into experiecing all sorts of side effects.
This sounds very biased. Nocebo may be true in some cases, but it’s a stretch to assume that everyone getting sides from finasteride has an anxiety disorder. Also, someone who nocebo’d themselves with finasteride wouldn’t be expected to improve with a stronger 5ARi if they believed that androgen antagonism was causing the sides, which is what most people believe.
This is based on ex-vivo and animal studies using high doses of finasteride and dutasteride would certainly also cause that effect due to also inhibiting 5ar2 and 5ar3.
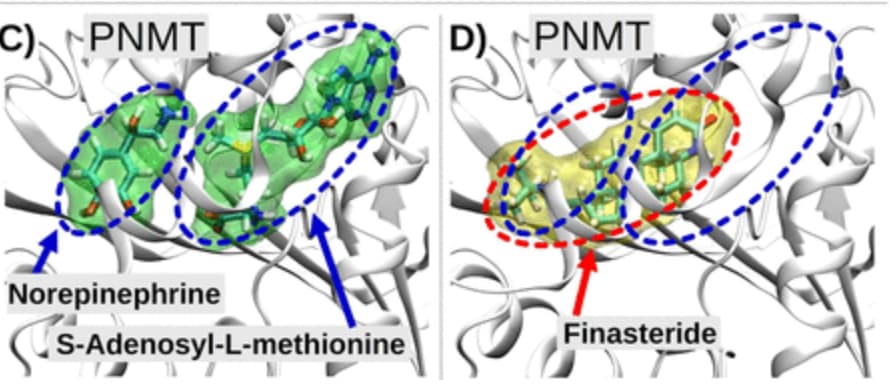
Finasteride was shown to inhibit hPNMT, and this is a 5AR-independent mechanism. Although the in vitro potency was very low (which doesn’t discount this mechanism contributing to sides, although it does make it less likely), there’s no evidence that dutasteride also inhibits PNMT.
This sounds very biased.
If you have been around on reddit for long enough, you know the type of people that hang out there. Just check out the profiles of various people.
Nocebo may be true in some cases, but it’s a stretch to assume that everyone getting sides from finasteride has an anxiety disorder.
The true incidence of side effects is 2-3%. above placebo. That equals roughly 1 in 50 people. And if you count both placebo incuded and finasteride induced side effects, the incidence is as high as 1 in 25 or even higher.
Also, someone who nocebo’d themselves with finasteride wouldn’t be expected to improve with a stronger 5ARi if they believed that androgen antagonism was causing the sides, which is what most people believe.
The amount of anecdotes from people who don’t experience side effects from dutasteride but do from finasteride is pretty low on reddit. There are more anecdotes of dutasteride absolutely destroying their hair which studies also do not support at all.
Finasteride was shown to inhibit hPNMT, and this is a 5AR-independent mechanism.
I am reading through the study in question right now. First they used a novel computer simulation model to figure out possible binding interactions of finasteride. This is fairly abstract and not necessarily real.
Although the in vitro potency was very low
According to my GPT, the serum concentrations of 1mg finasteride in adult humans is 0.025µM compared to 50µM used in the in vitro study. So that is still a rather high finasteride concentration and the PNMT inhibition was still only half of that of a selective PNMT inhibitior (30%).
The same applies to the Sprague-Dawley rat model, which were fed 1mg/rat/day. And it is questionable whether the effect would translate to an actual human being. For example, finasteride in humans is not selective to 5ar1 while it is in mice.
Overall too much mechanistic speculation without much data in humans. We know that dutasteride has about the same if not slightly lower side effect profile as finasteride, but if this PNMT inhibitory effect was significant enough in humans, it would translate to a much different side effect profile, unless dutasteride’s off-target effect or selective 5ar1 compensated for that.
Also, the lack of studies on dutasteride and PNMT inhibition does not necessarily imply that it does not do so.
To add to that, there is no evidence that finasteride nor dutasteride have an effect on the progression of AD or other neurodegenerative diseases in high risk groups who could be impacted by PNMT inhibition.
This study feels like it is grasping at straws to prove any kind of mechanistic connection between finasteride and side effects.
I experience side effects from finasteride. If I take 5 mg daily, it causes depression for me. I can take it twice a week without any (noticeable) side effects though. I am switching to dutasteride this summer to avoid any problems with finasteride.
I am reading through the study in question right now. First they used a novel computer simulation model to figure out possible binding interactions of finasteride. This is fairly abstract and not necessarily real.
Although the in vitro potency was very low
According to my GPT, the serum concentrations of 1mg finasteride in adult humans is 0.025µM compared to 50µM used in the in vitro study. So that is still a rather high finasteride concentration and the PNMT inhibition was still only half of that of a selective PNMT inhibitior (30%).
The same applies to the Sprague-Dawley rat model, which were fed 1mg/rat/day.
The computational approach provides evidence that the inhibition is competitive (i.e not allosteric). This is actually important information because they used a supraphysiological concentration of norepinephrine/substrate for their assay (probably to increase the sensitivity), which will make the inhibition from a competitive inhibitor look weaker than it actually is.
The physiological concentration of norepi is 0.5uM-5uM, whereas they used a concentration of 125uM, meaning that their substrate concentration was potentially ~250x the physiological one. If you play with the Michaelis-Menten equation, you’ll see that increasing the substrate concentration by 250x will also increase the IC50 by ~250x.
I fitted their approximate data points to a logistic curve which gave an IC50 of 100uM, which corresponds to an ‘in vivo IC50’ of 0.4uM (100/250), which isn’t far off from the serum concentrations. This approximation assumes that finasteride only competes with the binding of norepi, whereas from the figures it competes with both substrates. That situation still leads to a significantly larger IC50 than the ‘in vivo IC50’, but the exact fold difference is more complicated to determine. Just playing around with the numbers is fun sometimes, don’t take it too seriously.
Also, the lack of studies on dutasteride and PNMT inhibition does not necessarily imply that it does not do so.
Sure, but due to the bulkier substituent on dutasteride’s amide nitrogen steric hindrance might be an issue with fitting into the binding site.
And I had all sorts of side effects on dutasteride while having none on finasteride. The studies show a similar side effect profile though.
And then there is a question of how much of the free, unbound serum finasteride (~10% of serum finasteride) crosses the BBB and concentrates in the cerebrospinal fluid. Imo to actually potentially have a significant impact one would have to take much higher doses than the standard 1mg one.
I posted my stack there. Feedback welcome (here or there):
I wish you a lot of strength!