This was suggested by adssx in another thread. Simple concept. but potentially very powerful to help us reduce and optimize our drug intakes. Just comment on others drug stacks. Suggest things that can be eliminated, or weigh in on efficacies and synergies.
Please post your own stacks.
My stack as of 12/18/2024 (I am 47 male) items taken daily unless otherwise stated
The omega I currently take is Sports Research Triple Strength Omega 3 Fish Oil. Triglyceride form, 2.5/1 EPA/DHA ratio. Helped lower my blood triglyceride levels significantly. Puts me at 10 on the omega quant index.
My question would be about the statin and ezetimibe, and bempedoic acid. Do you have a documented lipid problem?
I dont eat carbs so no need for acarbose and the accompanying misery. Otherwise looks pretty comprehensive.
Right off the bench here I’d say get that heart balance test to see where to focus most — are you and overproducer or over absorber or something in the middle? Sounds like you just throw the kitchen sink at it otherwise.
Yeah I wanted to throw the kitchen sink at it! My LDL was around 150, ApoB at 145. In most people who overproduce, they still get benefit from ezetimibe. And vice versa. Thanks for commenting, hope some others post their stack
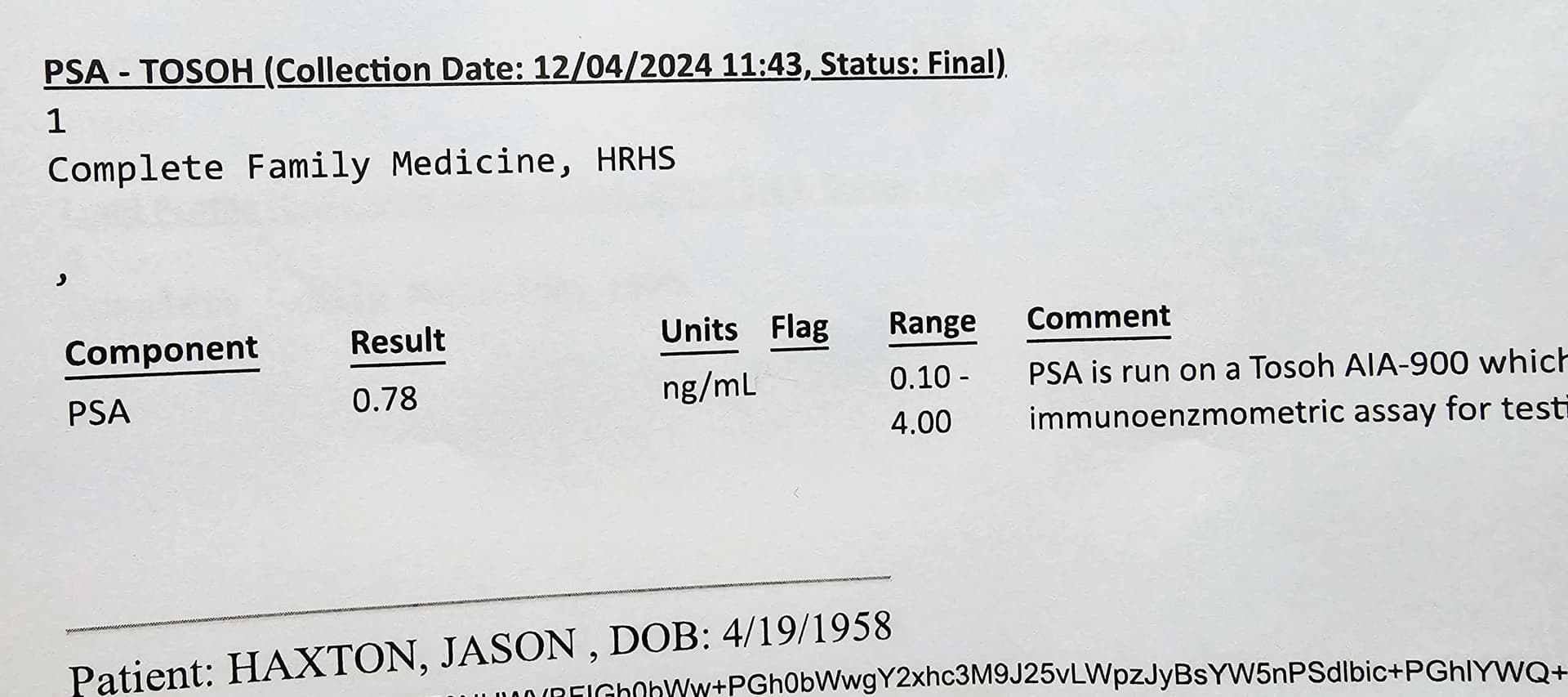
We have discussed this a little in another thread. It is one thing I am considering adding, My PSA is 0.6 which I am happy with for age 47, but I definitely want to look into trying it.
I’d say tadalafil, empagliflozin, and rapamycin are the riskiest ones in your stack in terms of rare but freaky side effects and in order of expected efficacy from lowest to highest. Priapism for tadalafil, genital infections for empagliflozin, and overall infections for rapamycin. Out of those 3 I’d guess rapamycin has the better risk vs. reward at a relatively moderate dose of 5 or 6 mg one time a week.
So far so good on tadalafil, been taking it for years, never had priapism. So far so good on no genital infections (I keep good hygiene, and more of an issue for women afaik). Yeah rapamycin no side effects so far, but only been on it a couple months.
But combination of it and rapamycin probably is not as good as one or the other for risk although hard to quantify. I think I overestimated this risk and it’s lower (for serious ones) when used on its own.
Yeah I have the same concern about ubiquinol, there are just so many conflicting studies. My rationale is that I take a moderate dose statin and do not want my coq10 depleted. I need to do more reading on the possible detrimental effects as far as statin/non-statin users.
The way I see it now is, on 20mg atorvastatin and 100mg coq10 I get no myopathy. I could eliminate the coq10 and see how the myopathy is. Not sure I want to bother with that, but will consider the experiment.
There’s not even evidence in statin users for muscle pain. You could also stop ubiquinol, lower atorvastatin to 10 mg and increase ezetimibe to the normal 10 mg.