Could you comment on this video with The Godfather of Melatonin research? He suggests that people late in life might take 50-150mg depending on their issues.
I had reliability issues with several consumer grade BP meters including ones from Balance Health and Omron. They usually err on the side of higher reading than actual, but I have seen the reverse as well when I was experimenting with various meters in the same sitting. In one occasion I took my meter with me to my doctor visit to compare with their higher grade triage BP meter. The result: some 6 or 7 higher on my device. A year ago my doctor at Kaiser sent me home with one from their medical devices stock which also uploads the data to the app/medical record. I am very satisfied with the device made by Omron (model HEM-8210T0), more expensive than the usual consumer grade BP meters. Turns out I have no high BP issues. For what it is worth, I google the model and I was able to find it for sale at around $280 from what looks like a medical devices seller. The link:
I don’t take rapa, so I’ve never considered this question.
My two cents:
Sotagliflozin and dapagliflozin were approved in Europe for Type 1 diabetes. They’re not approved anymore but “the removal of the type 1 diabetes indication is not because of any new safety concerns” (details of this complex case)
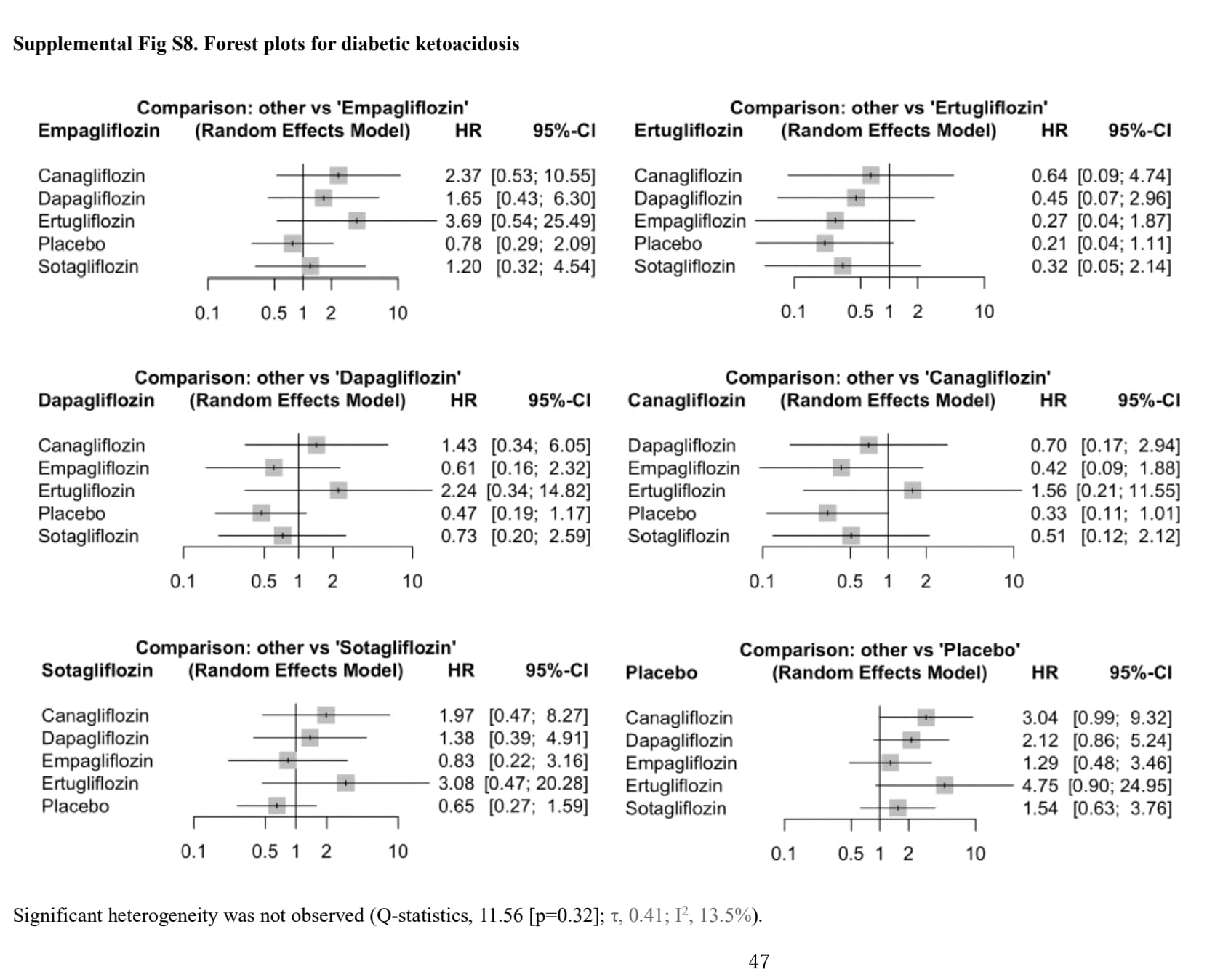
The DKA risk is dose-dependent (see Fig 2. Forest plot of comparison: SGLT2 inhibitors, outcome: incident diabetic ketoacidosis (DKA). in the above paper).
SGLTi are approved in non-diabetic people for CKD and HF.
For fasting, several papers looked at this such as Recommendations for management of diabetes during Ramadan: update 2020, applying the principles of the ADA/EASD consensus 2020: “Since the last Ramadan update in 2015, several studies have shown the safety of the SGLT2i class during Ramadan including lower risk of hypoglycemia and renal safety. However, careful pre-Ramadan assessment and education is important including advice on hydration and potential risk of volume contraction and postural hypotension, especially in warm climates with long fasting hours and risk of diabetic ketoacidosis (DKA). Testing for ketones when unwell is required for all patients who chose to fast and are using SGLT2i.”
So if SGLTi (and especially empagliflozin) are safe in nondiabetic people fasting (and also in T1D?), then I feel like we would need rapamycin to be an extremely potent inhibitor of insulin secretion to have any concern.
In doubt, check ketones + prefer empagliflozin 10 mg?
(On the other hand, we know that SGLTi increase the risk of genital infections by 4, and taking an immunosuppressant might not be great with GIs.)
I’ve been thinking of perhaps cycling between them
Rapa (and acarbose) in spring and summer, when I also focus more of resistance training than cardio and when risks of covid, colds, flu, pneumonia are generally smaller / and I’m more outside doing things
Come off of Rapa and onto SGLTi in the fall and winter, when my mTOR is less up given less resistance training and more focus on cardio and when extra good to have an optimized immune function
I’m sorry, I have to comment. I see a lack of balanced diet and Whole woods, coupled with drugs:supplements. I add this from a point of caring. Cheers to our health
SGLT2I and UTI are much more of a concern for women than men due to their physical differences. My father and I will be taking both Rapamycin and Empagliflozin (12.5 mg). We’ll let you know if there are any UTIs.