You are likely correct. If there is a spectacular success with the pita+BA+EZE combo, I may hazard dropping BA, as long as I’m below 60mg/dL on LDL, which is my goal. But there is the wrinkle, that for whatever reason, drugs often seem to lose effectiveness for me over time. When I first took atorvastatin 10mg/day at 60 years of age after a lifetime of very high LDL, it worked spectacularly - took LDL from 170mg/dL to 70 the first year. Every subsequent year it got worse, until Oct 2024, age 66, my LDL hit 146. Pita alone at 4mg/day after 5 months lowered it slightly to 123mg/dL. Who knows, the combo may work great initially, but not longer term. Lipids tend to get worse in older age (at least into the 70’s, though usually not beyond), hence medication might become less effective.
Starting May, it’s escalating empagliflozin to 25mg/day from the current 12.5, and adding 180mg/day BE. I guess I’ll keep stuffing myself full of drugs until something gives:sweat_smile:. It’s like a contest of wills, my body wanting to go along programmed senescence and general deterioration ending in ignominious death, and my iron will to impede that process as much as I can. With every drug escalation, I’m sending my body a message: "the beatings will continue until morale improves".
But seriously, the time window for improvement of biomarkers is growing more narrow - I’ll be 67 very soon. I have to do something. And fast.
Which Came First: Inflammation or Atherosclerosis?
“The inflammatory theory of CAD posits that chronic, low-grade inflammation plays a crucial role in the initiation, progression, and destabilization of atherosclerotic plaques,” said Pablo Corral, MD, manager of the Lipids and Atherosclerosis area in the Lipid Clinic at the ICM Institute, Buenos Aires, Argentina.
“However, current evidence suggests that inflammation primarily exacerbates atherosclerosis rather than serving as the initial trigger,” he told Medscape Medical News. “The retention and modification of apoB-containing lipoproteins within the arterial wall initiates the process, and inflammation follows as a maladaptive response to this lipid accumulation.”
“Atherosclerosis is caused by vascular inflammation due to cholesterol deposition that occurs with hyperlipidemia,” said Kathryn Moore, PhD, a cardiology professor at New York University Langone Health, New York City. “The immune system recognizes the accumulated lipids as foreign, setting off an inflammatory response in the artery wall, which if not resolved, leads to the formation of plaque.”
Here is a very nice and detailed look at the Clearly overlay on a CT angiogram, the data imagery, and interpretation, by the example of Matt Kaeberlein’s scan. A good discussion around the a test that many on this list are interested in. One thing which MK pointed out and I agree with completely, is that it’s really unfortunate that you as a paying pateint will not have access to the full report and will not be able to play with the images for further insight - the full report is only available to your medical provider; this strikes me as very paternalistic and condescending as if the patient must be shielded from data they can’t handle, and need handholding from their doctor - this attitude is outdated in an era of DIY health optimizers who take a leading role in their own care.
This Simple Test Can Reveal Your Risk Of Heart Disease
According to K. White in this interview, modern CT angio is about 2-3 mSv (old ones used to be in the 20 range). As to CAC, apparently depends on the protocol, but about 0.8 - 10.5 mSv.
Coronary artery calcification screening: estimated radiation dose and cancer risk
“Radiation dose from a single CAC CT scan varied more than 10-fold (effective dose range=0.8 to 10.5 mSv) depending on the protocol.”
I replied in your other thread, but I’ll chime in here, too
I have a scary CAC score but was advised to start taking calcium a few months ago for my bones. I was told if you take K, the calcium goes to your bones and not your arteries… I share this incase it’s helpful, but also incase that thinking has changed!
@John_Hemming, does this seem like a good mix? My supplement contains
600 mcg mk7
5 mg mk4
1500mcg k1 (not that I need this but it happens to be in there)
at times I pop an additional 300 mcg mk7
@Neo
My ApoB is 43 (on repatha, BA, and EZ) … my goal is 30 but it hasn’t happened yet.
My Lp(a) is now 134, pre repatha was aprox 187
CAC almost 500 over a decade ago. Almost 400 in my early 40s. Did not win the genetic lottery!
I don’t eat dairy and could possibly be convinced to start if that would be healthier for me, but while that could get me off calcium supplements, that would also raise my sat fat intake which would hurt me in other ways… rock and hard place sort of thing…
The mk4 looks right. The mk7 is ok, it is higher than many, but I am personally experimenting with much higher amounts at the moment. The K1 probably does not matter as you say.
How much resistance training do you do? Perhaps you could cut down on at least some of the calcium and instead up the resistance training a lot?
Perhaps with extra protein for a limited time like a year or so.
Then when we have Lp(a) lowering meds out in year or something and if they look successful, you could perhaps begin with one of them and then re-up the calcium a bit.
Thx. I have been focusing on resistance training for the last year. I dropped two of my three pilates sessions for resistance workouts. I should really add one more.
And sigh, I’m so focused on getting enough protein each day that I am miserable :), but yet I persevere!!! (I’m WFPB so it’s work!! So. Sick. Of. Protein. Shakes!!!)
A few weeks ago, someone on the forum shared that someone on LDN and rapa had phenomenal bone growth!! I’m hoping lightening strikes twice. My dexa was in aprox Oct, and I started LDN in Jan, so I imagine this summer would be a good time for an update and then create a new action plan. We will see if Ldn, calcium, and/or workouts have worked. Our much loved doc wants me on calcium, so I will continue unless we or he learns more. It doesn’t mean I am not nervous about it!
Sorry to hear K2s are impacting your sleep! I just googled and saw that it a thing for some. On my 1 minute deep dive on Reddit, someone suggested extra magnesium… ?
It is a bit surprising, since calcified plaque is usually more stable and less likely to rupture. And also, though Brad went for a very misleading, clickbaity title, the apparent nuance is that dietary calcium is absolutely fine whereas supplementing it is not.
Still, I’m pretty sceptical of those results. Even the claim itself just sounds incredibly implausible at face value; a 30-90% increase is massive. That’s the same magnitude of risk increase you see with something like obesity or smoking.
This I think is the K2s with more than 6 isoprene residues. I think it arises when the level of k2 >6 is going up which with a 75 hour half life means for potentially the first 5 doses of n.
My experience is that with it static things are generally ok and levels going down can be quite good for sleep.
My takeaway was don’t take calcium supplements without vit D (I can’t imagine that many people do), but I was not clear if he feels that solves the problem or it’s just better than nothing. I was surprised he didn’t mention K.
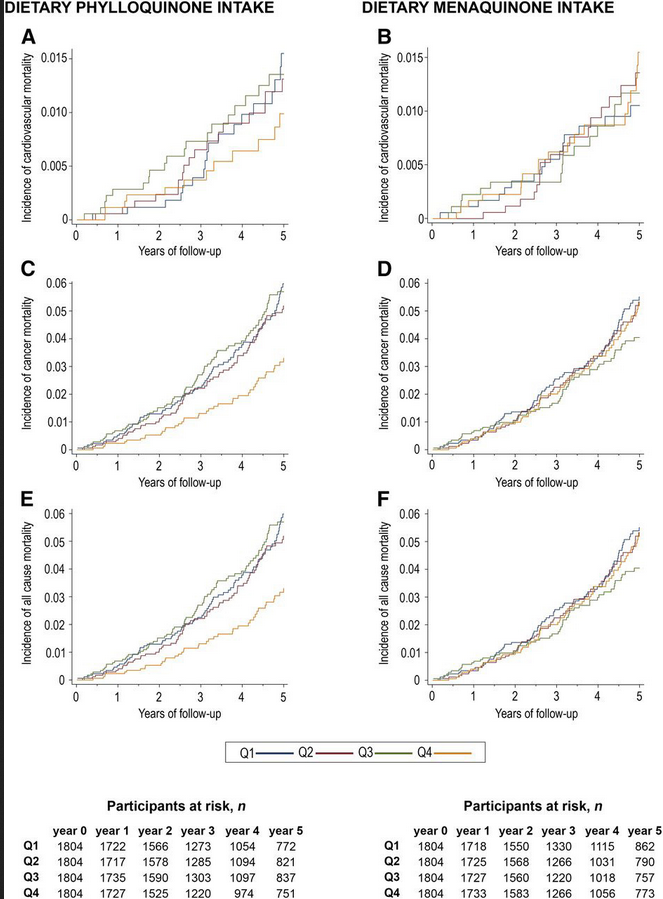
People on a med. diet followed till death and this is the pertinent graph:
Lustgarten spends a bunch of time on this in his amazing book on microbial burden and longevity. K1 helps get rid of the LPS to detoxify, makes more of the proteins that seal the gut barrier, and increases the IAP (intestinal alkaline Phosphatase). The study also talks about osteocalcin activity and all the wonderful things that does for you and how K1 increases it.
Green leafys or take the pill. You need 1400 or more K1 daily.
@Bicep thank you, that is great info! And I guess it explains why my supplement has so much k1.
I do try to eat a lot of greens, and Google just told me too much K1 can help blood clot. It makes me wonder if clotting is less than ideal for someone with heart disease… so much to learn!
I guess it’s time for a deep dive to learn more about this topic and to find out how much is too much k1.