I replied in your other thread, but I’ll chime in here, too
I have a scary CAC score but was advised to start taking calcium a few months ago for my bones. I was told if you take K, the calcium goes to your bones and not your arteries… I share this incase it’s helpful, but also incase that thinking has changed!
@John_Hemming, does this seem like a good mix? My supplement contains
600 mcg mk7
5 mg mk4
1500mcg k1 (not that I need this but it happens to be in there)
at times I pop an additional 300 mcg mk7
@Neo
My ApoB is 43 (on repatha, BA, and EZ) … my goal is 30 but it hasn’t happened yet.
My Lp(a) is now 134, pre repatha was aprox 187
CAC almost 500 over a decade ago. Almost 400 in my early 40s. Did not win the genetic lottery!
I don’t eat dairy and could possibly be convinced to start if that would be healthier for me, but while that could get me off calcium supplements, that would also raise my sat fat intake which would hurt me in other ways… rock and hard place sort of thing…
The mk4 looks right. The mk7 is ok, it is higher than many, but I am personally experimenting with much higher amounts at the moment. The K1 probably does not matter as you say.
How much resistance training do you do? Perhaps you could cut down on at least some of the calcium and instead up the resistance training a lot?
Perhaps with extra protein for a limited time like a year or so.
Then when we have Lp(a) lowering meds out in year or something and if they look successful, you could perhaps begin with one of them and then re-up the calcium a bit.
Thx. I have been focusing on resistance training for the last year. I dropped two of my three pilates sessions for resistance workouts. I should really add one more.
And sigh, I’m so focused on getting enough protein each day that I am miserable :), but yet I persevere!!! (I’m WFPB so it’s work!! So. Sick. Of. Protein. Shakes!!!)
A few weeks ago, someone on the forum shared that someone on LDN and rapa had phenomenal bone growth!! I’m hoping lightening strikes twice. My dexa was in aprox Oct, and I started LDN in Jan, so I imagine this summer would be a good time for an update and then create a new action plan. We will see if Ldn, calcium, and/or workouts have worked. Our much loved doc wants me on calcium, so I will continue unless we or he learns more. It doesn’t mean I am not nervous about it!
Sorry to hear K2s are impacting your sleep! I just googled and saw that it a thing for some. On my 1 minute deep dive on Reddit, someone suggested extra magnesium… ?
It is a bit surprising, since calcified plaque is usually more stable and less likely to rupture. And also, though Brad went for a very misleading, clickbaity title, the apparent nuance is that dietary calcium is absolutely fine whereas supplementing it is not.
Still, I’m pretty sceptical of those results. Even the claim itself just sounds incredibly implausible at face value; a 30-90% increase is massive. That’s the same magnitude of risk increase you see with something like obesity or smoking.
This I think is the K2s with more than 6 isoprene residues. I think it arises when the level of k2 >6 is going up which with a 75 hour half life means for potentially the first 5 doses of n.
My experience is that with it static things are generally ok and levels going down can be quite good for sleep.
My takeaway was don’t take calcium supplements without vit D (I can’t imagine that many people do), but I was not clear if he feels that solves the problem or it’s just better than nothing. I was surprised he didn’t mention K.
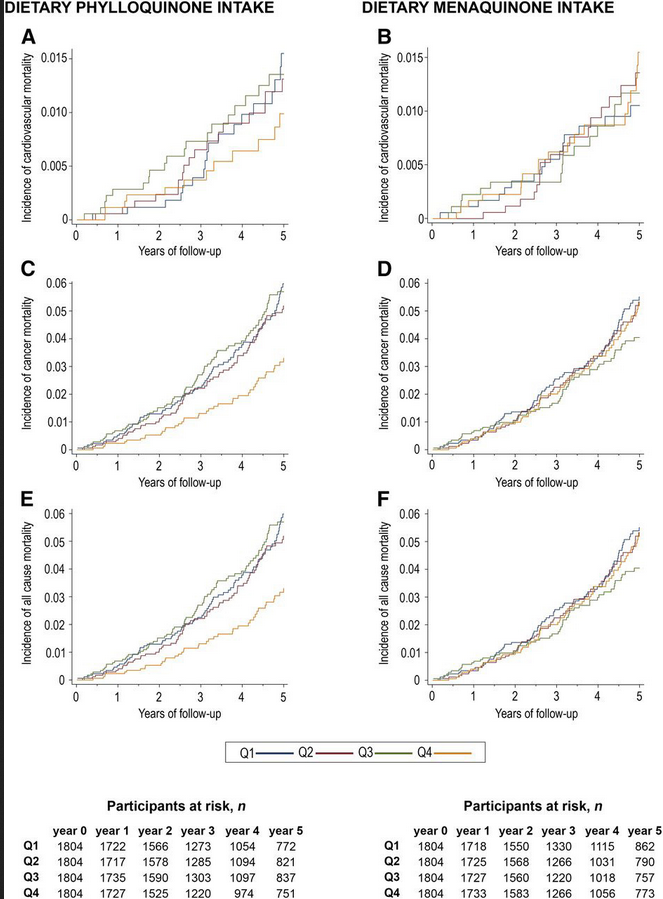
People on a med. diet followed till death and this is the pertinent graph:
Lustgarten spends a bunch of time on this in his amazing book on microbial burden and longevity. K1 helps get rid of the LPS to detoxify, makes more of the proteins that seal the gut barrier, and increases the IAP (intestinal alkaline Phosphatase). The study also talks about osteocalcin activity and all the wonderful things that does for you and how K1 increases it.
Green leafys or take the pill. You need 1400 or more K1 daily.
@Bicep thank you, that is great info! And I guess it explains why my supplement has so much k1.
I do try to eat a lot of greens, and Google just told me too much K1 can help blood clot. It makes me wonder if clotting is less than ideal for someone with heart disease… so much to learn!
I guess it’s time for a deep dive to learn more about this topic and to find out how much is too much k1.
@Paul This is the first I’m hearing of this, so thanks for sharing. I just did a quick google and it appears it might help a lot!!! And because there is no free lunch, it appears too much could cause heart attacks :). I’ll ask my docs about this asap!
Participants in the upper quartile of energy-adjusted dietary phylloquinone intake consumed nearly twice as many vegetables (especially leafy green vegetables and fruits) as those in the lower quartile. Increased menaquinone intake was associated with higher consumption of dairy products and meat (Supplemental Table 1).
The decision to discontinue the Repatha® Pushtronex® system was made to uphold the high standards Amgen holds for patient experience , focusing on delivering optimal care for patients with cardiovascular disease and hyperlipidemia (high bad cholesterol).
Dr Attia takes PCSK9 Inhibitors:, are probably needed to get lower. Very expensive 43 is excellent. Crestor 5 mg gives you appx. 85% of benefit. 10 mg 100% You can buy a combo pill of Crestor/Ezetimibe 10/10 for 1/2 cost. Good Luck on Lp(a) EZ is good, but BA?
Pharmacodynamic effect of bempedoic acid and statin combinations: predictions from a dose–response model
"Dose–response models predicted that combining bempedoic acid with the lowest statin dose of commonly used statins would achieve a similar degree of LDL-C lowering as quadrupling that statin dose; for example, the predicted LDL-C lowering was 54% with atorvastatin 80 mg compared with 54% with atorvastatin 20 mg + bempedoic acid 180 mg, and 42% with simvastatin 40 mg compared with 46% with simvastatin 10 mg + bempedoic acid 180 mg.
Conclusion
These findings suggest bempedoic acid combined with lower statin doses offers similar LDL-C lowering compared with statin monotherapy at higher doses, potentially sparing patients requiring additional lipid-lowering therapies from the adverse events associated with higher statin doses."