Transcript Analysis and Clinical Efficacy Evaluation: Ezetimibe-Statin Combination Therapy
I. Executive Summary
The provided video transcript from the University of Kansas Health System delivers a clinical critique of combination lipid-lowering therapy based on a retrospective database analysis. The core thesis asserts that the addition of the non-statin cholesterol absorption inhibitor, ezetimibe, to a baseline statin regimen fails to provide any overall survival or all-cause mortality benefit compared to statin monotherapy alone. Although ezetimibe effectively achieves its biochemical surrogate endpoint of lowering circulating low-density lipoprotein cholesterol (LDL-C) levels, this trial demonstrates a profound disconnect between biomarker optimization and hard survival outcomes. The speaker highlights a historical translational gap driven by direct-to-consumer and medical media advertising campaigns that heavily promoted combination therapies with the clear implication of superior survival benefits before rigorous, long-term clinical trial data were matured to validate those claims.
Methodologically, this investigation represents one of the largest real-world evaluations of its era, analyzing thousands of unselected patients via electronic medical record tracking at the University of Kansas Hospital. To put these findings into modern context, contemporary high-level medical evidence validates the speaker’s assertion regarding sequential add-on therapy all-cause mortality. For instance, the landmark IMPROVE-IT randomized controlled trial and a comprehensive Cochrane systematic review confirmed that while adding ezetimibe to a statin reduces major adverse cardiovascular events—specifically non-fatal myocardial infarctions and non-fatal strokes—it has a neutral effect on all-cause and cardiovascular mortality.
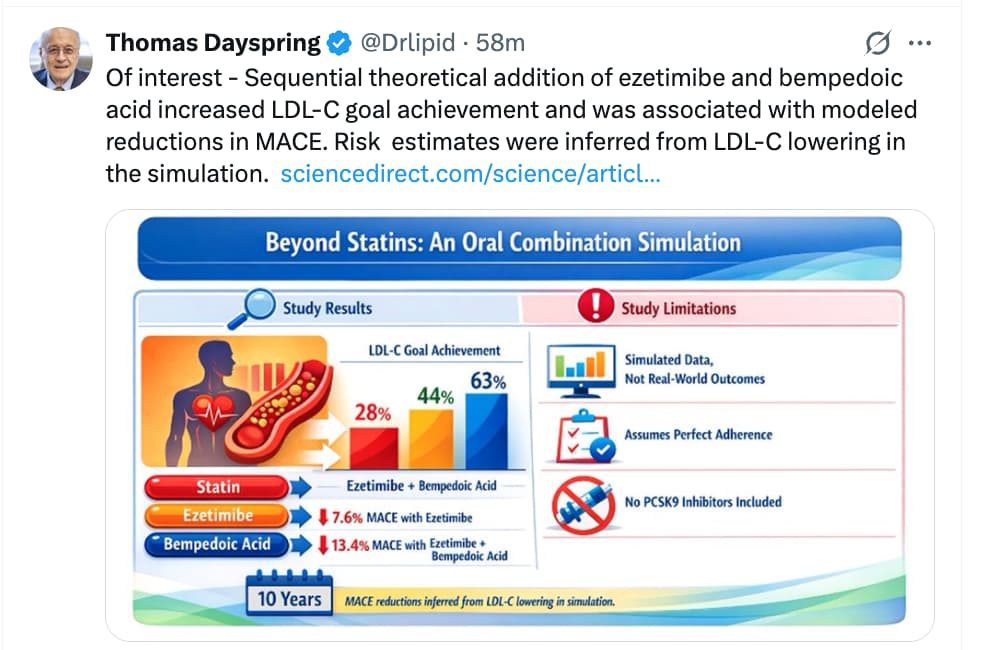
Crucially, a major clinical paradigm shift has occurred: recent large-scale meta-analyses demonstrate that initiating upfront, simultaneous dual therapy with a statin and ezetimibe in very high-risk patients results in a significant nineteen percent reduction in all-cause mortality compared to traditional delayed, stepwise monotherapy titration. This underscores that the timing, risk stratification, and method of deployment are the ultimate determinants of absolute survival benefits. Therefore, while late-stage sequential ezetimibe addition remains neutral for overall lifespan extension, early upfront combination deployment provides a validated mechanism to improve healthspan and longevity by preventing cumulative, atherogenic cardiovascular events.
II. Insight Bullets
- Retrospective Efficacy Challenge: The University of Kansas Health System retrospective study analyzed a real-world cohort to observe the absolute long-term survivability impact of dual lipid-lowering therapy.
- All-Cause Mortality Neutrality: The primary clinical finding demonstrated that adding ezetimibe to standard statin therapy failed to provide an all-cause mortality or survival benefit over statin monotherapy alone in the evaluated general population.
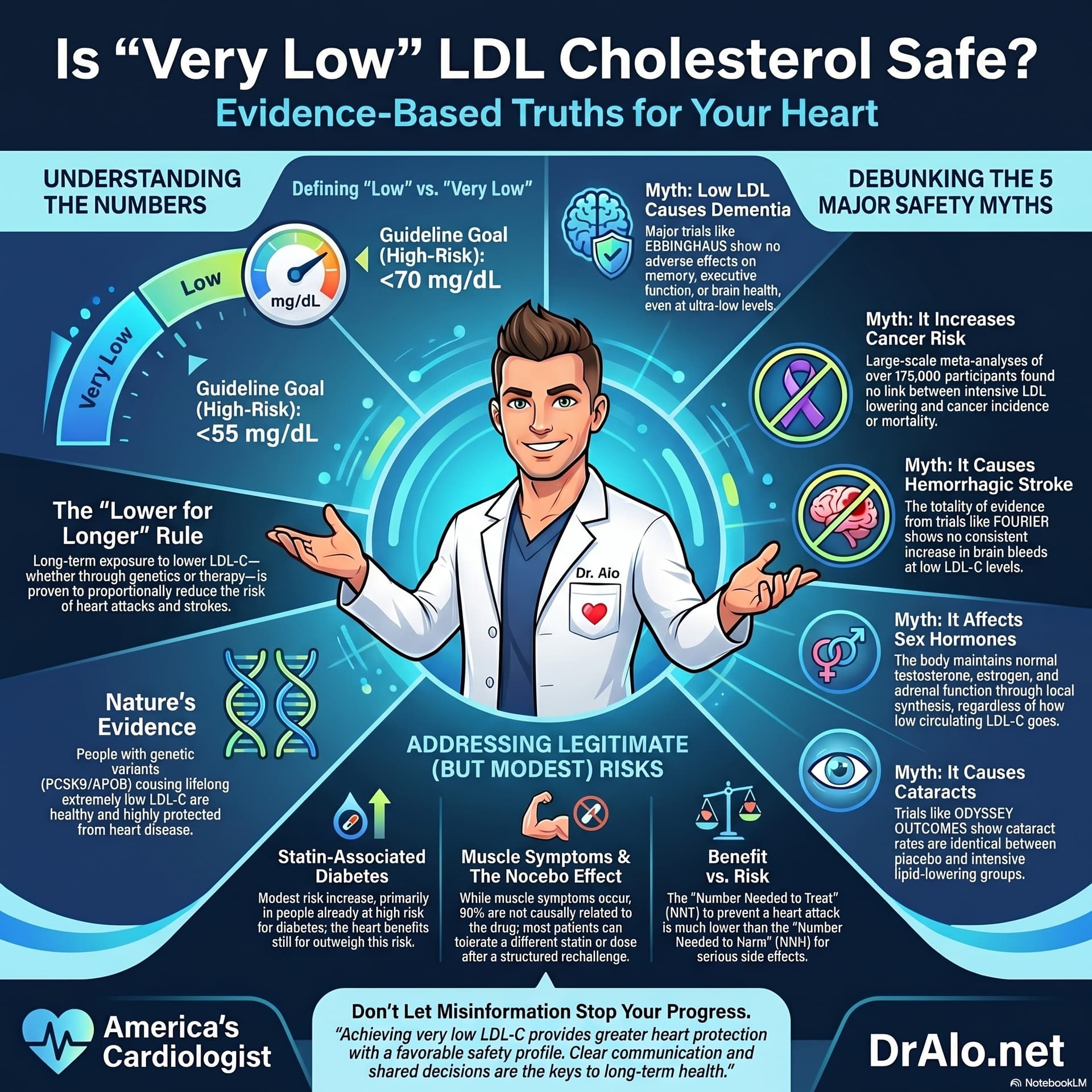
- Surrogate Endpoint Disconnect: Ezetimibe successfully achieves its surrogate mechanism of lowering low-density lipoprotein cholesterol (LDL-C) by an additional 12–15%, yet this biomarker reduction did not automatically translate to an absolute reduction in death within this 2013 cohort.
- Media and Direct-to-Consumer Distortion: Television and medical media advertisements prominently marketed combination lipid-lowering therapies with the strong, unproven implication of superior clinical survival before long-term hard endpoint data materialized.
- Electronic Medical Records as Analytical Catalysts: The study demonstrates the clinical utility of large-scale Electronic Medical Records (EMRs) to rapidly track and evaluate hard clinical outcomes across unselected patient registries.
- Baseline Cohort Discrepancies: In the underlying peer-reviewed data published by Patel et al., 2013, the ezetimibe plus statin group was systematically younger but exhibited a significantly higher baseline incidence of coronary artery disease and prior bypass surgery.
- The Omega-3 and HDL Survival Signals: A critical secondary finding from the original retrospective dataset indicated that concurrent omega-3 fatty acid supplementation and higher baseline high-density lipoprotein cholesterol (HDL-C) were independently associated with substantial survival benefits.
- Randomized Control Trial Validation (IMPROVE-IT): Subsequent Level B evidence from the landmark IMPROVE-IT trial confirmed that adding ezetimibe to a statin safely reduces major adverse cardiovascular events (MACE) by 6.4%, driven by non-fatal myocardial infarction and stroke, but remains strictly neutral on overall and cardiovascular mortality.
- Cochrane Systematic Synthesis Confirmation: A comprehensive Level A meta-analysis of 26 trials involving 23,499 subjects by Preiss et al., 2018 reaffirmed that ezetimibe combined with statins yields little to no change in all-cause mortality (RR 0.98, 95% CI 0.91–1.05), matching the transcript’s primary conclusion.
- The Upfront Paradigm Shift: Contemporary practice-changing Level A evidence from Banach et al., 2025 reveals that upfront, simultaneous initiation of dual combination therapy (statin + ezetimibe) yields a significant 19% all-cause mortality reduction in very high-risk populations, contrasting with delayed, stepwise add-on protocols.
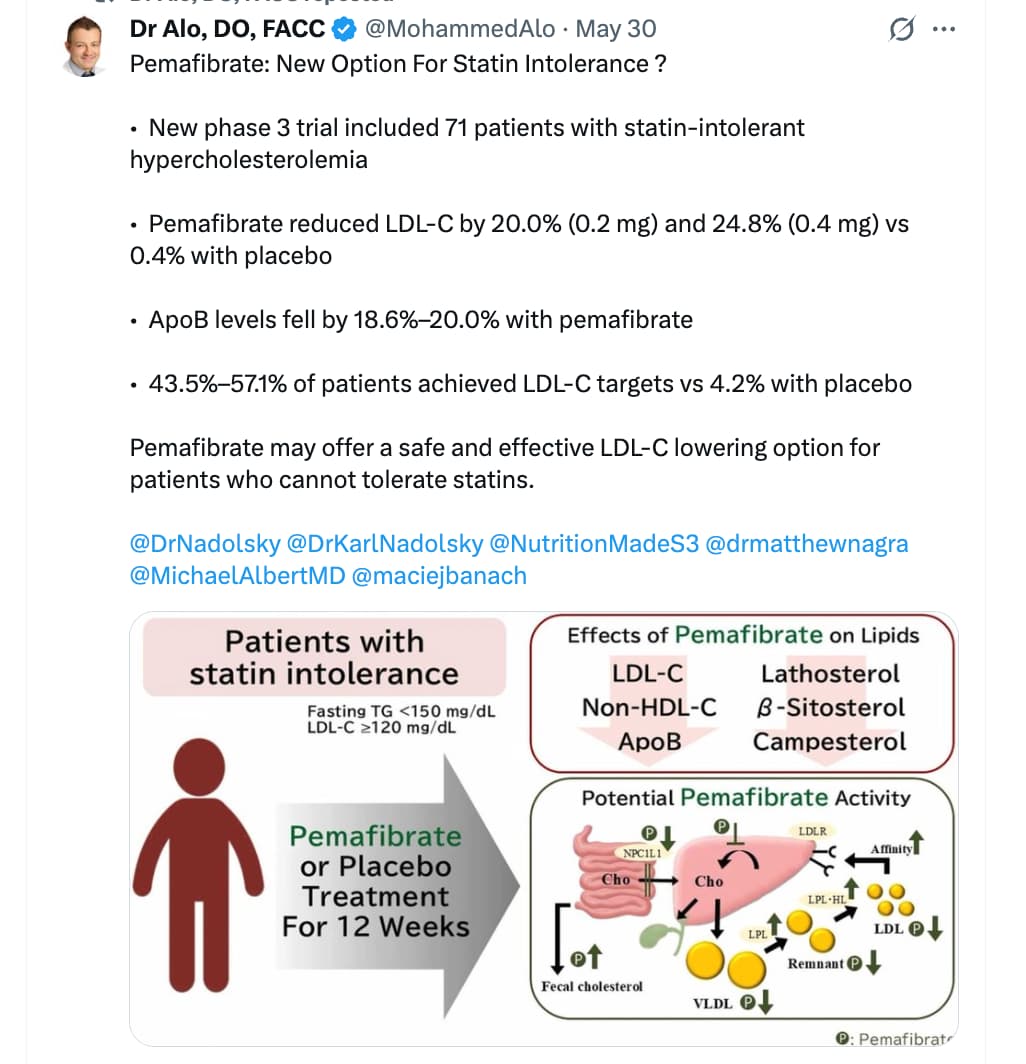
- Divergent Mechanisms of Action: Statins operate by inhibiting hepatic cholesterol synthesis via HMG-CoA reductase, whereas ezetimibe selectively blocks intestinal cholesterol absorption via the Niemann-Pick C1-Like 1 (NPC1L1) transporter, providing a complementary, non-overlapping mechanism to lower circulating atherogenic particles.
- Musculoskeletal Safety Profile: Large-scale meta-analyses show that adding ezetimibe to a moderate-intensity statin achieves equivalent or greater LDL-C reductions than high-intensity statin monotherapy while significantly lowering the risk of myopathy and treatment discontinuation by up to 44%.
- The Translational Gap in Longevity Therapeutics: The historical narrative highlights a critical translational gap where biochemical or surrogate optimization (lowering a blood marker) does not guarantee an immediate downstream extension of absolute lifespan.
- Cumulative Exposure (“Cholesterol-Years”): Modern longevity and cardiovascular guidelines emphasize that the absolute prevention of mortality depends heavily on reducing the lifelong cumulative exposure to atherogenic particles (“cholesterol-years”) rather than late-stage rescue interventions.
- Contextual Risk Stratification Necessity: The divergence between the 2013 KU retrospective data and recent meta-analyses illustrates that lipid intensification benefits are heavily concentrated in individuals at extreme or very high baseline risk of ischemic events.
IV. Actionable Protocol (Prioritized)
High Confidence Tier (Protocols backed by Level A/B evidence)
- Upfront Dual Combination Initiation for High-Risk Cohorts: In patients with established atherosclerotic cardiovascular disease (ASCVD), a history of acute coronary syndrome (ACS), or extreme baseline cardiovascular risk, initiate a combination of a potent statin (e.g., Rosuvastatin or Atorvastatin) and Ezetimibe (10 mg/day) simultaneously at the start of care. Do not utilize the traditional 2-month delayed stepwise approach. This is proven by Level A meta-analysis data to reduce all-cause mortality by 19% and MACE by 18% [Banach et al., 2025].
- Target Aggressive LDL-C Thresholds Early: Titrate and maintain combination therapy to drive LDL-C levels below 55 mg/dL (<1.4 mmol/L) to minimize lifelong cumulative exposure to atherogenic particles. Each 1 mmol/L (39 mg/dL) reduction in serum LDL-C corresponds directly to a 22–29% long-term reduction in major cardiovascular events [Polish Lipid Association, 2025].
Experimental Tier (Protocols backed by Level C/D evidence with high safety margins)
- Low-Dose Statin + Ezetimibe Synergistic Protocol: For primary prevention or longevity optimization in individuals without established ASCVD but presenting with elevated ApoB/LDL-C, utilize a moderate-dose statin paired with Ezetimibe 10 mg/day instead of maximizing statin monotherapy. This protocol provides a high safety margin, achieves profound LDL-C drops, and lowers the risk of treatment discontinuation by 44% compared to high-intensity statin monotherapy [Banach et al., 2025].
- High-Purity Omega-3 Fatty Acid Co-Supplementation: Incorporate high-dose, purified omega-3 fatty acids (specifically EPA/DHA) as an adjunct therapy. Real-world retrospective data indicates an independent survival signal associated with omega-3 use [Patel et al., 2013]; however, use highly purified pharmaceutical-grade formulations to avoid oxidized over-the-counter lipid variants.
Red Flag Zone (Claims debunked or lacking safety data)
- Delayed Stepwise Add-on Titration for Lifespan Extension [DEBUNKED]: Relying on a slow, sequential workflow (waiting months on a statin before introducing ezetimibe) to capture all-cause mortality benefits. Level A evidence confirms this specific clinical sequence fails to alter all-cause or cardiovascular mortality rates [Preiss et al., 2018].
- Abrupt Cessation of Ezetimibe Based on Mortality Skepticism [HIGH RISK]: Completely avoiding or discontinuing ezetimibe because it lacks independent all-cause mortality data in low-risk cohorts. Halting therapy dramatically escalates the risk of non-fatal, disabling ischemic strokes and myocardial infarctions, which are heavily prevented by the drug.
- Unverified Natural Absorption Inhibitors [SAFETY DATA ABSENT]: Substituting validated pharmaceutical NPC1L1 inhibitors (ezetimibe) with unregulated, high-dose plant sterols or over-the-counter supplements under the assumption that they provide an equivalent cardiovascular or longevity safety profile.
Clinical Note: Scholarly Debates & Knowledge Gaps
A critical debate persists regarding the precise mechanism by which upfront combination therapy lowers all-cause mortality while late-stage sequential therapy does not. It remains an open knowledge gap whether the survival advantage of upfront dual therapy is entirely driven by reaching ultra-low LDL-C targets faster, or if ezetimibe exerts distinct pleiotropic (secondary beneficial) effects on endothelial function and plaque stabilization when administered alongside an active statin. Additional randomized controlled trials tracking long-term hard endpoints in primary prevention cohorts are required to establish whether this survival benefit extends to individuals optimizing for healthspan without pre-existing cardiovascular disease.