Finally got results from my CCTA. Nothing like I expected. This is basically a CAC. I asked about Cleerly and she said it was unnecessary because she could read better than the machine. Here is the entire report:
She never asked me for my history but probably it is in my medical history. Here is the last 5 years of CAC reports:
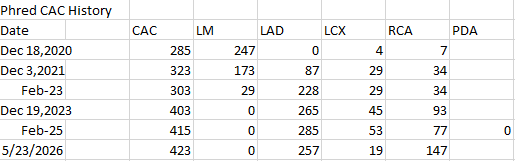
The big jump was in 2023, since then I’ve basically plateaued. The RCA could be an issue. For awhile the LAD seemed to be on fire, now going down again. Now RCA is smouldering. I wonder what put out the fire. Possibilities are:
Heavy metal treatment…Several EDTA IV treatments, learned of DMSA oral and did it for about a year, also every day Pectasol which is a binder and shown in some studies to work against heavy metals and heart disease.
Neprinol…seems unlikely but it is 30000FU nattokinase and 90000SPU of serrapeptase plus support complex and etc… I’ve been on it daily for years.
Full dose Astaxanthin
Boswellia
500mg berberine twice daily
The cardiologist offered me a coronary angiogram and said she could put in a stent if it looked like it would help. I don’t think I’ll go for that at this time because I don’t want the stent. She offered Leqvio and managed to get it for free through some program. I’m going to try that. What does anybody think?
There are 2 trials for that may shed light on all cause mortality on Leqvio…ORION-4 results in late 2026 and VICTORION-2 PREVENT in 2027.
What did this do?
DMSA is great at removing lead. It unfortunately takes copper out really well too. It’s taken orally. So I took it once a week and took copper daily. Never had a problem.
New Heart Disease Prevention Trial Makes Waves

I. Executive Summary
This analysis reviews a major primary prevention clinical trial evaluating the PCSK9 inhibitor evolocumab (Repatha) in patients at high cardiovascular risk who have no prior history of a myocardial infarction or stroke. Unlike secondary prevention models that optimize lipid management post-event, this trial assesses whether aggressive lipid-lowering can intercept and prevent initial ischemic events in subclinical populations with high risk factors, such as established arterial plaque or long-standing diabetes.
The trial enrolled over 12,000 participants in a randomized, double-blind, placebo-controlled design with a 4.6-year follow-up. Most participants were already receiving baseline lipid-lowering therapies, including statins or ezetimibe. Evolocumab administration resulted in profound lipid reductions: LDL cholesterol declined by 55%, non-HDL cholesterol by 47%, and apolipoprotein B (ApoB) by 44%.
The primary composite outcome—consisting of myocardial infarction, stroke, or cardiovascular death—demonstrated a statistically significant reduction in risk, with 336 events in the treatment group compared to 443 in the placebo arm. This equates to a roughly 25% relative risk reduction. Exploratory secondary outcomes revealed a 36% reduction in myocardial infarctions alone, a 21% reduction in overall cardiovascular mortality, and an estimated 20% drop in all-cause mortality.
Methodologically, the trial highlights the absolute risk reduction of 1.8% over 4.6 years, yielding a Number Needed to Treat (NNT) of approximately 55. However, because cardiovascular disease represents a chronic, lifetime exposure model, absolute risk reductions accumulate over time. Extrapolating the data across a lifetime exposure window suggests the NNT could drop to between 5.7 and 8.0.
While the trial confirms the therapeutic efficacy of monoclonal antibodies for primary prevention, it also highlights the concept of residual risk. The treatment did not eliminate all cardiovascular events because it addresses only one component of vascular disease: ApoB-containing lipoproteins. It does not modulate blood pressure, insulin resistance, or metabolic dysfunction.
Furthermore, because the average age of the participants was 66, the intervention represents a late-life mitigation of a lifetime of vascular damage. Genetic mendelian randomization studies show that individuals with lifelong, low-expression PCSK9 mutations experience a two- to three-fold greater reduction in cardiovascular events than those starting therapy late in life. This underscores the clinical necessity of early-life, comprehensive risk-factor modification.
II. Insight Bullets
- Primary Prevention Breakthrough: This trial provides the first large-scale clinical evidence that PCSK9 inhibitors effectively lower the incidence of initial heart attacks and strokes in high-risk patients who have never experienced an ischemic event [[01:36]].
- Aggressive Lipoprotein Clearance: Monoclonal antibody inhibition of PCSK9 via bi-weekly injection drives systemic clearance of atherogenic particles, lowering LDL-C by 55%, non-HDL-C by 47%, and ApoB by 44% [[02:29]].
- Primary Composite Risk Reduction: Over a 4.6-year tracking window, evolocumab achieved a 25% relative risk reduction in combined heart attacks, strokes, and cardiovascular deaths [[02:46], [03:02]].
- Ischemic Interception Metrics: Individual secondary outcomes demonstrated a 36% relative reduction in myocardial infarctions and a 21% reduction in total cardiovascular mortality [[03:25]].
- All-Cause Mortality Signals: The data indicated an estimated 20% reduction in all-cause mortality, reinforcing the survival benefit of intensive lipid optimization even when initiated later in life [[03:42]].
- Absolute Risk Divergence Kinetics: Kaplan-Meier curves show that the absolute clinical benefit of PCSK9 inhibition requires prolonged exposure; risk reduction is negligible at year one but widens progressively through years two, three, and four [[04:15]].
- The Time-Dependency of NNT: The absolute risk reduction over 4.6 years was 1.8%, resulting in an interim NNT of 55. This calculation is heavily time-dependent and falls over longer tracking periods [[04:03], [05:05]].
- Lifetime NNT Extrapolation: Lifetime projections for high-risk cohorts indicate that keeping ApoB particles consistently low can drop the NNT down to between 5.7 and 8.0 as lifetime absolute risk rises [[05:23], [05:41]].
- Adverse Event Parity: The overall number of adverse events did not differ significantly between the evolocumab and placebo cohorts, affirming a reassuring safety profile for primary prevention populations [[06:00]].
- Monoclonal Adverse Signals: Well-documented side effects specific to evolocumab include mild nasopharyngitis (cold-like symptoms), transient back pain, and potential increases in blood glucose in susceptible individuals [[06:17]].
- The Consistency Sourcing Method: Relying on data from a single industry-funded trial introduces risk, but confidence increases when results align across three distinct large-scale PCSK9 clinical trials [[06:30], [07:22]].
- Reverse-Engineered Human Genetics: PCSK9 inhibitors represent a successful translation of human genetics into pharmacology, modeled after rare loss-of-function mutations that naturally protect individuals from vascular disease [[07:44], [08:25]].
- The Multi-Factorial Residual Risk Trap: Despite dramatic reductions in ApoB, substantial residual cardiovascular risk remained in the treatment arm because the therapy does not address secondary risk factors like hypertension or diabetes [[09:10]].
- The Cumulative Area Under the Curve: A 5-year late-life intervention yields modest absolute changes because it truncates only a small fraction of a patient’s lifelong vascular exposure to atherogenic lipoproteins [[09:45]].
- Lifelong vs. Late-Stage Mitigation: Mendelian randomization confirms that lifelong genetic reduction of PCSK9 provides a two- to three-fold higher reduction in cardiovascular events than starting pharmacological therapy at an average age of 66 [[10:28]].
- LPA Sub-Fraction Depletion: Beyond standard ApoB-containing particles, PCSK9 inhibitors provide a unique clinical advantage over statins by concurrently lowering Lipoprotein(a) [Lp(a)] levels by 15% to 20% [[10:47]].
IV. Actionable Protocol
High Confidence Tier (Backed by Level A Evidence)
- Utilize PCSK9 Inhibitors for Primary Interception: If an individual presents with advanced subclinical cardiovascular disease (e.g., high coronary artery calcium or dense soft plaque) or long-standing Type 2 diabetes but has no history of a heart attack, consider adding a PCSK9 inhibitor to achieve target lipid ranges [[00:11], [11:43]].
- Target Comprehensive ApoB Clearance: Optimize lipid-lowering therapies to target an aggressive reduction in Apolipoprotein B particles. Pair baseline statin or ezetimibe therapies with PCSK9 monoclonal antibodies to achieve a combined reduction of ~44% in ApoB and ~55% in LDL-C [[01:53], [02:29]].
- Maintain Long-Term Therapy Adherence: Commit to long-term compliance with prescribed lipid therapies. Clinical trials demonstrate that the absolute benefit of intensive lipid-lowering is cumulative, showing expanding divergence and maximum event prevention after 2–4 years of continuous treatment [[04:15]].
Experimental Tier (Emerging Clinical Guidelines with Favorable Risk-Benefit Profiles)
- Initiate Risk Factor Suppression Early in Life: To maximize cardiovascular longevity and match the protective event-reduction rates seen in genetic cohorts, identify and manage elevated ApoB and blood pressure early in adulthood. This approach avoids the cumulative, irreversible vascular damage that occurs when treatment is delayed until later in life [[10:15], [10:28]].
- Leverage PCSK9 Inhibitors for Lp(a) Reduction: If a patient presents with elevated Lipoprotein(a)—a highly atherogenic sub-fraction that does not respond to traditional statin therapy—consider utilizing a PCSK9 inhibitor to achieve a concurrent 15% to 20% reduction in Lp(a) while optimizing general ApoB clearance [[10:47]].
Red Flag Zone (Claims Contradicted by Data or Lacking Safety Evidence)
- Do Not Expect Single-Pathway Therapy to Eliminate Risk: Avoid assuming that achieving ultra-low LDL or ApoB levels completely eliminates cardiovascular risk. Residual risk remains high if concurrent driving factors, such as blood pressure, visceral adiposity, and insulin resistance, are left unmanaged [[09:10], [09:25]].
- Monitor Metabolic Parameters on Monoclonal Antibodies: Do not overlook glycemic control while on intensive PCSK9 inhibitor therapy. Due to potential tracking signals showing elevated blood glucose in predisposed cohorts, regularly monitor fasting glucose and HbA1c during long-term treatment [[06:17]].
V. Literature Verification & Methodological Context
The clinical trial discussed by the host represents a major milestone in primary cardiovascular prevention, and its findings align with the established consensus on the relationship between apolipoprotein B and atherogenesis.
- Primary Prevention Data and the EVAPORATE/FOURIER Context: The host’s analysis focuses on a large primary prevention trial of evolocumab, which expands on findings from secondary prevention models like the FOURIER trial (Sabatine et al., 2017). It also builds on the EVAPORATE trial, which demonstrated that aggressive, long-term non-HDL-C reduction can arrest and induce the regression of low-density plaque components over a multi-year tracking window (Budoff et al., 2020).
- Lifelong vs. Late-Stage Exposure (Mendelian Randomization): The host’s emphasis on early intervention is supported by genetic epidemiology. Landmark mendelian randomization analyses published in the Journal of the American College of Cardiology confirm that lifelong exposure to lower circulating LDL-C and ApoB levels due to specific gene variants reduces cardiovascular risk by more than 50% per unit change. This reduction is substantially greater than the risk reduction achieved when comparable lipid-lowering therapies are initiated late in life (Ference et al., 2012).
- PCSK9-Mediated Lp(a) Dynamics: The mechanism by which PCSK9 inhibitors lower Lipoprotein(a) by 15% to 20% is well-documented. While statins can subtly increase circulating Lp(a) concentrations, upregulation of hepatic LDL receptors via PCSK9 clearance increases the non-specific endocytosis and destruction of Lp(a) particles, providing an added therapeutic benefit for patients with this genetic risk profile (Bittner et al., 2024).
Methodological Caveat: Although this primary prevention trial establishes clear relative risk reductions for ischemic events, the absolute risk reduction over 5 years is modest (1.8%). This underscores the importance of patient selection, confirming that these high-cost monoclonal antibody therapies should be reserved for individuals with clear, documented subclinical vascular damage or multiple compounding risk factors.
So this is more about drastically lowering ldl levels. The weapon of choice just happens to be psck9 inhibitors. I wonder if these ldl levels coincide with the ones where plaque regression occurs.
Yes, more proof that lower is better when it comes to APO-B / LDL-C, here is the study (paywalled):
https://www.nejm.org/doi/full/10.1056/NEJMoa2514428
VESALIUS-CV enrolled thousands of patients with known atherosclerotic cardiovascular disease (ASCVD) or high-risk diabetes but whom had no history of myocardial infarction and stroke and either LDL-C of 90 mg/dL or higher, non-high-density lipoprotein cholesterol of 120 mg/dL, or apolipoprotein B of 80 mg/dL or more. Patients also were required to be currently treated with an LLT. Randomization allotted patients to receive either evolocumab or placebo in addition to optimized LLT and were followed for a median of 4.5 years.1
Primary end points of the trial were time to first occurrence of a composite of coronary heart disease (CHD) death, heart attack, or ischemic stroke, in addition to time to first occurrence of a composite of CHD death, heart attack, ischemic stroke, or any ischemia-driven arterial revascularization.1
Lower lifelong LDL cholesterol = better longevity
A 2021 paper that Mike Lustgarten just tweeted out: https://x.com/mike_lustgarten/status/2059448296855265356?s=20
Low-Density Lipoprotein Cholesterol and Lifespan: A Mendelian Randomization Study
Lifelong Cholesterol Restriction Directly Dictates Human Lifespan and Extreme Longevity
The question of how circulating low-density lipoprotein cholesterol (LDL-c) affects human life expectancy outside high-risk clinical cohorts has long remained a battleground of conflicting observational data. While randomized controlled trials definitively prove that lipid-lowering drugs protect individuals with advanced cardiovascular disease, the long-term impact of LDL-c on the lifespan of the broader, unselected population has been obscured by confounding variables, reverse causality, and brief clinical trial durations. A massive genetic study has bypassed these clinical blind spots, demonstrating that elevated LDL-c directly curtails human lifespan and slashes the odds of achieving exceptional longevity.
Using Mendelian randomization—a methodology that leverages naturally inherited genetic variants to mimic a permanent, lifelong clinical trial—researchers analyzed exposure data from 173,082 individuals and survival outcomes from a massive cohort of 1,012,240 individuals. By tracking eighty distinct single-nucleotide polymorphisms that dictate baseline LDL-c levels, the study simulated the lifelong physiological consequences of varying cholesterol profiles in individuals not pre-selected for cardiovascular risk.
The primary findings are stark. A single standard deviation increase in genetically driven lifelong LDL-c (approximately 38.7 mg/dL) translates directly to a 1.21-year reduction in overall lifespan. When evaluating extreme survival thresholds, individuals with genetically elevated LDL-c exhibited a 28 percent lower probability of reaching the 90th percentile of survival compared to the 60th percentile. For context, this 90th percentile corresponds to living past 89 years for men and 94 years for women in typical modern cohorts.
Crucially, when dissecting specific genetic drug targets, variants in the PCSK9 gene region—which mimic the therapeutic mechanism of modern PCSK9 inhibitors—demonstrated a robust, statistically significant impact on lifespan. Every standard deviation increase in LDL-c mediated through this pathway reduced lifespan by approximately one year. Conversely, genetic proxies for other common drug targets, such as HMGCR (targeted by statins) and NPC1L1 (targeted by ezetimibe), trended toward a similar lifespan reduction but lacked sufficient statistical power to clear the threshold of significance.
Significantly, the study uncovered that less than half of the story is explained by conventional heart attacks. Exactly 42 percent of LDL-c’s detrimental impact on lifespan operates via biological mechanisms fully independent of traditional coronary artery disease and ischemic stroke. This indicates that high circulating LDL-c drives mortality through broader, systemic vascular deterioration, peripheral vascular disease, or abdominal aortic aneurysms. Ultimately, these genetic insights prove that maintaining low LDL-c throughout adulthood yields a major systemic net lifespan benefit.
Actionable Insights
For longevity optimization, the primary take-home message is that cumulative, lifelong exposure to low LDL-c is fundamentally superior to late-stage crisis management. Because 42 percent of the lifespan hazard from LDL-c is independent of traditional heart attacks and strokes, keeping apoB-containing lipoproteins low prevents broad systemic vascular degradation across multiple organ systems.
Clinically, this validates the proactive, early deployment of lipid-lowering strategies in individuals who do not fit classical high-risk cardiovascular profiles. The genetic data uniquely highlights the robust lifespan protection offered by the PCSK9 pathway, positioning PCSK9 inhibitors or long-acting small interfering RNA therapies (such as inclisiran) as premier therapeutic choices for structural longevity management. Because conventional daily oral pills face high rates of long-term patient non-adherence and side effects, moving toward long-acting therapeutics or profound early dietary shifts—such as the restriction of saturated fat to lower the population distribution of LDL-c—can securely maximize survival advantages. Longevity seekers should prioritize driving LDL-c down early in adulthood to compound survival advantages over decades, rather than delaying treatment until arterial plaque has already accumulated.
Context & Impact Evaluation
- Institutions: Harvard Medical School (United States), Imperial College London (United Kingdom), St George’s University of London (United Kingdom), Novo Nordisk Research Centre Oxford (United Kingdom).
- Countries: United States and United Kingdom.
- Journal Name: British Journal of Clinical Pharmacology.
- Impact Score Context: The impact score of this journal is 3.0, evaluated against a typical high-end range of 0–60+ for top general science, therefore this is a Medium impact journal.
Good. I had also emailed the Editor to express concern and got the impression that they were looking into it - especially after the authors were talking so much BS on social media.
Big YES to the siRNA PCSK9i. I recall (sorry if I’m incorrect) that you don’t like statins, but from your results it looks that lowering your ApoB/LDL-C is the biggest bang for buck now. It will make a bigger difference than all the other stuff on your list combined.
The positive CAC unfortunately means you have relatively advanced atherosclerosis, which shows that whatever LDL-C level you have had previous was sufficient to build long-lasting plaque which has gone through the entire cycle of inflammation and repair. So whatever level you had, it ideally needs to be lowered. I think a sensible way to look at this is prioritisation. Even if statins or PCSK9i etc have potentially detrimental effects, they also have proven benefits for the very thing which is affecting you now. So IMO, you should go for aggressive lowering of atherogenic particles.
On top of that, lowering inflammation is super important, as I’m sure you know. Good luck with it all!
Anti-inflammatory effects of oral NLRP3 inhibition with ruvonoflast among individuals at elevated cardiovascular risk
Oral NLRP3 inhibition with ruvonoflast significantly reduced hsCRP with concurrent reductions in inflammatory biomarkers in participants with elevated inflammatory risk. Ongoing Phase 2 trials of larger size and longer duration will further characterize the therapeutic potential of ruvonoflast.
Following up on my previous post, relaxedmeatball, as I promised I went ahead and carefully read all the studies you posted, including re-reading the ones I was already familiar with. Initially I was going to comment on each study separately, but quickly ran into severe length issues - it would require blog length multiple posts which is not practical. So I scrapped that approach (hours of writing wasted, lol!) and focused on my original design of looking at ACM. I will of course refer to some of the studies posted, but without detailed analysis. As an example, the first study you posted (“Emerging views of statin pleiotropy and cholesterol lowering” PMCID: PMC8803071) you write the authors took a “sceptical tone” - I would characterize it as perhaps more of a review listing counterarguments to statin pleiotropy without ultimate commitment to one side of the argument - for instance in the PCSK9i and ezetimibe trials as evidence, they do observe that these were done on top of statin use, so it ultimately doesn’t allow for a clear conclusion; the use of Betteridge Law type headings further place it in the “more research needed” category and “here is how we think research could decide the issue” proposals. But these are nuances, and the general directionality of your remarks is fair, IMO.
Nonetheless, touching upon the cancer vs statin issue, I wanted to at least introduce some newer fascinating research, so it doesn’t simply become cherry picking of studies for and against. I think there is a very cool mechanism illustrated here which might explain why there are such conflicting results wrt. statins and cancer - it is possible that in a broad category of cancers there is a timing and adaptation element (as so often with cancer). So while some statins might intitially be effective against it, cancer adapts and they no longer work the same. This is of course not the case for all cancer, but I thought super interesting nonetheless. It appears mediated at least partially by cholesterol avialability. Additionally relevant to rapa fans, it touches upon mTOR1. Here’s the study and a popsci article:
Noncanonical PI(4,5)P2 coordinates lysosome positioning through cholesterol trafficking
https://www.science.org/doi/10.1126/sciadv.aeb8658
“Apart from the role of PI5P4Ks in coordinating lysosomal cholesterol trafficking, this study highlights the critical nature of these enzymes in TNBC tumor maintenance. Using an inducible knockdown model, we have shown that depletion of these enzymes in established tumors leads to decreased activation of mTORC1 signaling, apoptotic cell death, and an accumulation of intratumoral cholesterol. An intriguing question that remains is to what extent the deficiency of p53 affects endogenously synthesized cholesterol turnover, low-density lipoprotein (LDL) derived cholesterol import, or the balance between these two systems. This question will have great importance for the future of therapeutics, where cholesterol trafficking is targeted in breast cancer and beyond.”
And the popsci article:
Cholesterol-craving cancers need lipid enzymes to use metabolites for growth, study shows
https://medicalxpress.com/news/2026-05-cholesterol-craving-cancers-lipid-enzymes.html
"“The mTOR activation pathway is really what drives tumorigenesis, and so mTOR is an important target for cancer drug development,” said Emerling. “If we can target mTOR activity in aggressive cancers by blocking the sensing of cholesterol, that would be a promising treatment strategy.”
Previous research has looked at the use of statins as cancer drugs due to their ubiquity and safety as treatments for patients with high cholesterol. While more research is needed, studies so far suggest that tumors eventually acquire resistance to statins. “It is important for us to find other ways to more comprehensively cut cancer cells off from cholesterol to impede their growth,” said Loughran.
“We’ll continue to explore blocking PI5P4Ks as a more targeted approach tailored to how tumors operate,” said Emerling."
I think there’s still a place for statins here, if one can find a way to prevent the cancer adaptation. This could synergize well with mTOR drugs, so I think those of us taking both rapamycin and statins might actually be addressing cancer metabolism in some way - of course, we need data showing cancer rates, perhaps in transplant patients taking both vs those who are taking only rapa.
I myself attempted to take advantage of such possible synergy when it came to my beloved cat (RIP) who was suffering from a bad case of squamous cell carcinoma that started on his lower eyelid. Rapamycin by itself was pretty effective in reversing the spread of the cancer to the rest of his skin elsewhere (head, neck and shoulders), but despite escalating the dose, it failed to arrest the original site. Hunting around, I found indications that pitavastatin (which I conveniently had a lot of on hand) might be useful:
Pitavastatin Induces Apoptosis of Cutaneous Squamous Cell Carcinoma Cells through Geranylgeranyl Pyrophosphate-Dependent c-Jun N-Terminal Kinase Activation
“In addition to the effects of regulating blood lipids, many studies have shown that pitavastatin has anticancer effects. For example, pitavastatin acts on lung cancer cells and human lung tumor-associated endothelial cells by suppressing prenylation-dependent Ras/Raf/MEK and PI3K/Akt/mTOR signaling10. In another example, pitavastatin induces apoptosis in oral SCC through activation of FOXO3a11. Although anticancer effects have been recognized in other systems, the effects and action mechanism of pitavastatin on cutaneous SCC cells have not been investigated.”
One of the complications when looking at the effect of statins on cancer is that these are broad categories, and there are differential effects of specific statins on specific cancers. Pitavastatin is one such example. In any case, the fact is that the paper here on pita and SCC is not in vivo in cats, so my looking at this was a case of pure desperation trying anything on earth to save my cat. I understood the odds were super remote, but nonetheless having nothing to lose, all the vets having completely given up, I tried pitavastatin 0.25mg/day + rapamycin 6mg/1-week. In the end, I don’t think this did much of anything, but by that point where I was trying everything and anything the cancer was already in a pretty advanced state.
Nonetheless, I think combining statins with mTOR modifiers and other agents in the pathway might be effective in cancer treatment and/or prevention.
But back to statins and cancer. Since cancers are a pretty heterogenous bunch, I would not expect statins or any drug to necessarily affect all of them. Much more targeting is needed seems to me, starting with specific statins or statin classes, perhaps in specific cohorts:
Lipophilic Statins and Risk for Hepatocellular Carcinoma and Death in Patients With Chronic Viral Hepatitis: Results From a Nationwide Swedish Population
Parochially, as a male, I have an interest in prostate cancer (according to my genetic profile I’m at a 40% increased risk), so if some med can pleiotropically give me some benefit off target, well, I’ll take it. In that spirit, while not a slam dunk, I think statins are a reasonable roll of the dice. As someone of Scandinavian extraction, this caught my eye - even if just an association:
Postdiagnosis Statin Use and Mortality in Danish Patients With Prostate Cancer
Earlier and more generally, seems statin use prior to diagnosis might be better:
Use of statins and the risk of death in patients with prostate cancer
Rather than look at individual or small studies, I think it might make sense to subsume RA into all inflammatory conditions to get more subjects based on purported anti-inflammatory effects of statins. A 2020 meta:
Effect of statin use on cardiovascular events and all-cause mortality in immune-mediated inflammatory diseases: A systematic review and meta-analysis involving 148,722 participants
"Our meta-analysis included 12 studies that comprised 148,722 patients with IMIDs (57,670 statin users, 91,052 statin non-users) contributing more than 840,113 patient-years. In pooled analysis, statin initiation was associated with 28 % decreased risk of all-cause mortality (random-effects: meta-HR 0.72, 95 % CI 0.65-0.80), 23 % decreased risk of major adverse cardiovascular events (fixed-effects: meta-HR 0.72, 95 % CI 0.62-0.83). Subgroup analysis of patients with rheumatoid arthritis showed similar results (fixed-effects: meta-HR 0.77, 95 % CI 0.67-0.89 for all-cause mortality; meta-HR 0.75, 95 % CI 0.63-0.88 for major adverse cardiovascular events). Furthermore, the protective role of statin in decreasing mortality was stronger in patients receiving statin for primary prevention of cardiovascular diseases than that for secondary prevention (fixed-effects: meta-HR 0.64, 95 % CI 0.59-0.70; meta-HR 0.84, 95 % CI 0.80-0.89, respectively), although both were statistically significant. Additional analysis yielded similar benefit from statin usage between females and males regarding mortality.
Conclusion: Statin use was associated with lower risks of mortality and cardiovascular events, with greater benefits for primary prevention in those IMIDs patients without prior cardiovascular disease."
Of course, again, this is association, but fairly suggestive. Of note, ACM is computed, not just CV events.
Ancient history might have given a preview of the beneficial effects of the anti-inflammatory effect:
Influenza and COPD mortality protection as pleiotropic, dose-dependent effects of statins
“This study found a dramatically reduced risk of COPD death and a significantly reduced risks of influenza death among moderate-dose statin users.”
Ultimately, for me, it comes down to ACM, as I wrote in my previous post, where I gave extensive grounds for this preference. The problem here is disentangeling the CV mortality from other causes and the fact that there are no large cohorts of patients who take statins with no CVD or CVD risk factors. Ideally, we’d like long term adequately powered RCTs of statin users who took them without any CV indication (vs placebo). Perhaps understandably there are no such trials, but it would be the cleanest way to answer the question of whether there are any pleiotropic effects (off target CVD) of statins that affect ACM.
I looked at a whole bunch of studies going all the way back to the early 2000’s to gather enough trials with enough power to at least attempt to disentangle some of these confounders**(1)**. To begin I
So we have to make do with what we have, trying to glean ACM numbers apart from CV related mortality, often with other morbidity confounders, such as T2DM:
Effects of statins on all-cause mortality at different low-density-lipoprotein cholesterol levels in Asian patients with type 2 diabetes
“In addition to reducing LDL-C levels, statin therapy reduced all-cause mortality risk in Taiwanese patients with T2DM. Statins further reduced the mortality risk at most LDL levels. However, at low LDL-C levels, the positive effects of statins may have been nullified.”
What is interesting here is that the ACM advantage is retained at various LDL levels (apart from the lowest), which seems fairly significant in implying more general pleiotropic impact of statins on ACM.
Mortality increases with age. Therefore, it would be of particular interest to look at ACM precisely in the elderly:
Statin Use Over 65 Years of Age and All-Cause Mortality: A 10-Year Follow-Up of 19 518 People
“Adherence to statins may be associated with reduced mortality and cardiovascular morbidity among older adults, regardless of age and sex.”
(1)[Sorry, this is again turning into blog length, so I may come back to this later].
Happy to read your reply, and again I will come back with something more detailed when I have time ![]()
I’m sorry to hear about your cat. It’s horrible when pets get sick. Advanced cancer is something where we still don’t have really good options for most of them (yet).
Again, for the record, I am not taking any sort of anti-statin position. I take them, and I encourage most others to take them. The Swedish/HCC paper I actually was aware of, since somebody close to me was unfortunately recently diagnosed with this and their doctor actually suggested a statin based on this study. However, the evidence, while suggestive, is still fairly weak since there are plenty of confounders (interaction with medical system, medication compliance etc etc). But still - the thinking is that very few people don’t benefit from a low-dose statin, and HCC is a very serious diagnosis, so there’s really no downside to trying.
My gut feeling would be that disentangling all of the various effects is probably close to impossible. I also reckon there’s no such thing as a free lunch, and it wouldn’t surprise me (pure speculation here) if hitting lipid metabolism is detrimental to some cancers but beneficial to others. (That’s certainly been the case for other interventions). And even for cancer mortality, as you said, unless somebody launches a massive study, we’ll be left with these observational studies, biomarker studies etc. Since statins are incredibly widespread nowadays, we should be seeing clear reductions in some diseases, and to my reading anything outside of CVD is murky at best. Though I agree that there are interesting suggestions that other things are at play - I just don’t think they’re strong effects.
Short-Term Trials, Lifetime Gains: Mathematical Modeling Reveals Statins Extend Life by Years, Not Days
A controversial meta-analysis previously sparked debate by claiming that statin therapy yields a surprisingly minor survival benefit—averaging just a few weeks of prolonged life. However, this bleak conclusion contains a fundamental methodological flaw: it looks only at survival within the artificially restricted timeframe of randomized controlled trials (RCTs), which typically last only five to six years. Because patients continue living—and benefiting—long after a clinical trial concludes, analyzing raw trial runtimes fundamentally misrepresents the true cumulative impact of lipid-lowering therapies on human longevity.
To expose this limitation, researchers deployed Gompertz mathematical modeling to project human survival curves across an entire remaining lifespan. The Gompertz distribution is highly accurate for mapping human mortality, particularly in older and post-operative populations. By digitizing the historical survival curves of two landmark statin studies—the 4S trial and the LIPID trial—the authors extrapolated the short-term dataset out to the patients’ predicted biological lifetimes.
The results completely shift the narrative around cardiovascular prevention. While the absolute survival extension achieved during the actual active trial periods was indeed minor—amounting to a meager 22 days in the LIPID trial and 26 days in the 4S trial—the projected lifelong survival gains were massive. Over a complete lifetime horizon, statin therapy extended mean survival by 2.8 years for the LIPID cohort and a remarkable 9.9 years for the 4S cohort.
Crucially, the researchers validated their mathematical projections using real-world extended follow-up data collected after the formal trials ended. The extrapolated Gompertz curves tightly matched the actual observed long-term survival of the patients, solidifying the predictive power of the model. Ultimately, the study demonstrates that short-term clinical metrics drastically obscure the compound interest of early, sustained preventative health interventions.
Actionable Insights
For longevity optimization, this study offers critical takeaways regarding cardiovascular health management:
-
Shift to Lifetime Horizons: Evaluate preventative therapeutics through a lifelong lense rather than short-term windows, as true longevity benefits compound exponentially over decades.
-
Target Aggressive LDL Reduction: Lifespan extension scales dynamically with the absolute magnitude of low-density lipoprotein (LDL) reduction. The 4S trial achieved an LDL drop of 1.77 mmol/L, yielding 5.6 years of life extended per mmol/L , whereas the LIPID trial achieved a 1.03 mmol/L reduction, yielding 2.7 years per mmol/L.
-
Prioritize Vascular Health Early: Atherosclerosis operates as a primary organ-specific aging bottleneck; initiating lipid optimization early maximizes the area under the survival curve before irreversible vascular senescence occurs.
-
Balance Risks Dynamically: While statins dramatically extend life on average, individual therapy must still balance these multi-year statistical gains against personalized risk profiles, such as potential metabolic or muscle-related adverse effects.
Source
- Paywalled Paper: A method to estimate the mean lifetime survival increase of statin therapy
- Institutions: Medical Data Research Center, Providence Health & Services, Portland, Oregon; Heart Clinic Cardiology, Providence Health & Services, Portland, Oregon; Providence Spokane Cardiology, Spokane, Washington.
Sorry if it was noted earlier (and I missed it) but what is the 4S cohort? What substances did it test/study?
Even Trump takes Ezetemibe.
His cholesterol levels have improved significantly with the help of medication. Trump’s total cholesterol came in at 143, down from 223 in 2018. It had been down to 140 last April. He takes rosuvastatin to help lower his bad cholesterol, known as LDL, and to raise his good cholesterol, or HDL. He also takes ezetimibe to help lower his LDL.
It’s the Scandinavian Simvastatin Survival Study, hence 4S.
Ezetimibe a bust? Very old. Less than 2 minutes long (1:29).
Well-Known Cholesterol Drug Doesn’t Live Up To Promises (via The University of Kansas Health System)
