I have a bit of a dilemma. My LDL is a bit high 124 last reading, but more concerning is my HDL very low at 38, but surprisingly my LP(a) is supper low at 11. triglycerides is optimal/normal at 55 and ApoB a bit high but normal at 78. so based on these what do you guys think are my risks? Should I worry about my high LDL or the low Lp(a) and other good indicators are enough to counter the negative effects of high LDL? I hear that Lp(a) and ApoB are more important than LDL, and finally what is a good medication that helps increase HDL.BTW, I started Ezetimibe 10mg, and Pita 2mg after my last lab work (three months ago) and expect them to lower my LDL level some (will measure in next month or so) but is there something else that helps with HDL?
Note that raising hdl doesn’t lead to improved clinical outcomes for CVD. See Effect of HDL-Raising Drugs on Cardiovascular Outcomes: A Systematic Review and Meta-Regression
Wow, very interesting. So, I guess leave HDL alone and just focus on lowering LDL seems like a more reasonable approach.
You can ignore lp(a) as a risk factor. It is largely genetically driven and only 20% have elevated lp(a). That will never be you. I wish I had addressed my elevated LDL-C much sooner than I did. I used to have scores similar to yours. Sometimes lower and often higher. Non-HDL-C is a better marker of risk and yours is not optimal.
do you inject it yourself? I would rather just take my statins by mouth that have to do injections.
I haven’t had any side effects at all. My statin doesn’t give me any effects either.
Yes it’s a self injecting pen. Very easy and painless. But it does give me sides that lasted a few day. Statins give me even more sides that last as long as I take them.
I did have a thread about this a while ago - about the budgeting/ROI of longevity interventions.
For example, we know sleep is “good for you”. But you could make a major gain by sleeping 1h less per night, from age 18 until 85. That equates to 24,455 extra waking hours, or almost 3 years of conscious time.
So if you want to sleep 1h extra per night, you’d better make sure it gets you back much MORE than 4 extra years of life, otherwise you have a net loss.
You can run similar calculations for exercise at 150 minutes per week. 7,800 mins per year, or 522,600 minutes you’d spend from 18-85. That’s 362 days in total. So getting the recommended 150m/week of exercise is probably a really good ROI. But exercising 2 hours every day would take ~5.6 years of your time.
That said, I think you kinda disprove your point in your post. The people you know lived WAY longer than average by doing nothing special, which means they had good genetics. New research reckons that 50% of your total natural lifespan is dictated by genetics. And for extreme outliers like hitting 100, the genetics is an even bigger part.
I recon the main value of being health conscious is avoiding early death. You could consider that preventable, but it might only be preventable thanks to 2026 modern medicine. In 1950 that would have been your natural lifespan, possibly through no fault of your own. We’re in the CVD thread, which can give you the impression that it’s all preventable, but don’t forget the cancers that hit young people, middle-aged people, infections etc. And even in CVD, plenty of people have arrhythmias which can cause sudden death, valve problems, aortic aneurysms, basically through no fault of your own. If you’re born with some variant of KCNA5 which gives you a dodgy potassium ion transporter in the heart, you have a ticking time bomb in your chest that no amount of clean eating or exercise will defuse.
Great question. (FYI I am a PhD, researching cardiovascular disease, but not an MD)
I think it’s safe to say that HDL-C number doesn’t matter really. Your HDL-C function matters, but we can’t measure it. Raising HDL-C might make you feel happy about the number of paper, but doesn’t give any cardioprotection whatsoever. However, low HDL-C is generally a biomarker that something is a bit wrong.
So should you be concerned about HDL-C of 38? Kinda, I think. It can be affected by insulin resistance.
Your Lp(a) is super low. Congratulations.
Triglycerides also good.
And your LDL (124) and ApoB (78) can definitely be lower if you want to be optimal.
Important questions are: what is your age, and have you ever had a CTCA or calcium score done?
Thanks for your very detailed and informative answer. I’m 60 and no I haven’t done a CTCA or calcium scan (one of those days I will), but I’ve been health conscious for a very long time, last 35 years and doubt I am in bad shape CVD wise as I have always stuck with healthy fats and vegies and lean meat.
As far as your other views i.e. sleeping one hour less, or time spend exercising etc… I agree with you with caveat of what’s the opportunity cost. Take for example spending time at gym. Ok, I’m not much the exercising type but there are other notable benefits of me being at the gym (as opposed to maybe watching tv) as for example looking (definitely not creepy staring) at that 25-year-old girl’s perfect body shape (mesmerized at God’s perfect creation LOL) and casually socializing with other likeminded dudes in there, so yeah I’ll take that any day to seating on a couch and staring at a blank screen LOL.
I agree with everything you say here, and yes, you are right it is thanks to 2026 modern medicine that I think many of the aging maladies can be definitely delayed (and perhaps prevented). In 1960 Genes took priority when it came to living long, today I think poly-pharma (and what is widely known and accepted such as moderate exercise and eating healthy) is equally (maybe even more important) than the genes. In other words, you can fix most of what you didn’t get in gene pool by being proactive and takings certain meds to prevent early death. Obviously, we can never play God or Masters of everything, because there are always chances of things known or known happening (i.e. certain cancers, accidents, wars, pandemics etc…) but for the main culprits such as diabetes, stroke, CVD and to some extend neurophysical diseases are largely preventable (given the state of the modern medicine and the ease of getting information).
I don’t think this view is correct. The percentage of people living to 100+ is growing and not because we suddenly have better genes. Most of the longevity calculators estimate that I will live past 100 and they are not factoring in rapamycin, sglt2 drugs and other interventions
Here is an ai view:
It is a common belief that the “longevity lottery” is won purely through DNA, but recent data and projections suggest that while genetics play a role, the environment and lifestyle are increasingly the primary drivers for most of the population.
The short answer is yes, the percentage and absolute number of people living to 100+ is growing rapidly—and it is projected to skyrocket over the next few decades.
1. The Numbers: A “Longevity Revolution”
The global centenarian population is experiencing what the United Nations calls a “longevity revolution.”
- Past vs. Present: In 1950, there were only about 2,300 centenarians in the U.S. By 2024, that number grew to over 101,000.
- The Quadruple Effect: The U.S. Census Bureau and Pew Research project that the number of American centenarians will more than quadruple by 2054, reaching roughly 422,000.
- Global Scale: Globally, there are about 722,000 centenarians today. This is expected to grow to nearly 4 million by 2054.
Current Centenarian Density (per 10,000 people)
| Country | 2024 Estimate | 2054 Projection |
|---|---|---|
| Japan | 12 | 40 |
| Thailand | 5 | 49 |
| United States | 3 | 14 |
| China | <1 | 6 |
2. Genetics vs. Lifestyle: The 2% vs. 17% Rule
Recent large-scale studies have begun to quantify exactly how much “blame” or “credit” we can give to our genes. A landmark 2025 study from Oxford Population Health (published in Nature Medicine) analyzed data from nearly 500,000 participants to settle this debate:
- Genetics: Accounted for less than 2% of the variation in the risk of death.
- Environment & Lifestyle: Accounted for 17% of the variation.
- The “Proteomic Age” Gap: Researchers now use blood protein levels to measure “biological age.” They found that factors like smoking, physical activity, and socioeconomic status create a gap between your chronological age and how fast your body is actually wearing out.
The Caveat: While lifestyle dictates who reaches 85 or 90, scientists still find that for the “super-centenarians” (those 110+), specific protective genetic variants become much more significant. For the average person aiming for 100, however, the “input” (lifestyle) matters more than the “blueprint” (DNA).
3. Why is the growth so “spectacular” now?
The reason we are seeing a spike isn’t because our DNA changed, but because of a “statistical wave” combined with medical progress:
- The Baby Boomer Wave: The largest generation in history is currently entering the age brackets where 100 is the next milestone.
- Delayed Onset: We are getting better at “compressing morbidity”—the period of time a person spends ill at the end of life. Instead of dying of a heart attack at 70, medical interventions (like statins, better BP management, and stents) push that event into the late 80s or 90s.
- Biohacking & Prevention: There is a growing shift toward viewing aging from a statistical and scientific point of view—focusing on VO2 max, muscle mass retention, and metabolic health—which is moving the needle for more people than ever before.
Would you like me to look into specific biological markers or “ageing clocks” that scientists are currently using to predict who is on track for a 100-year lifespan?
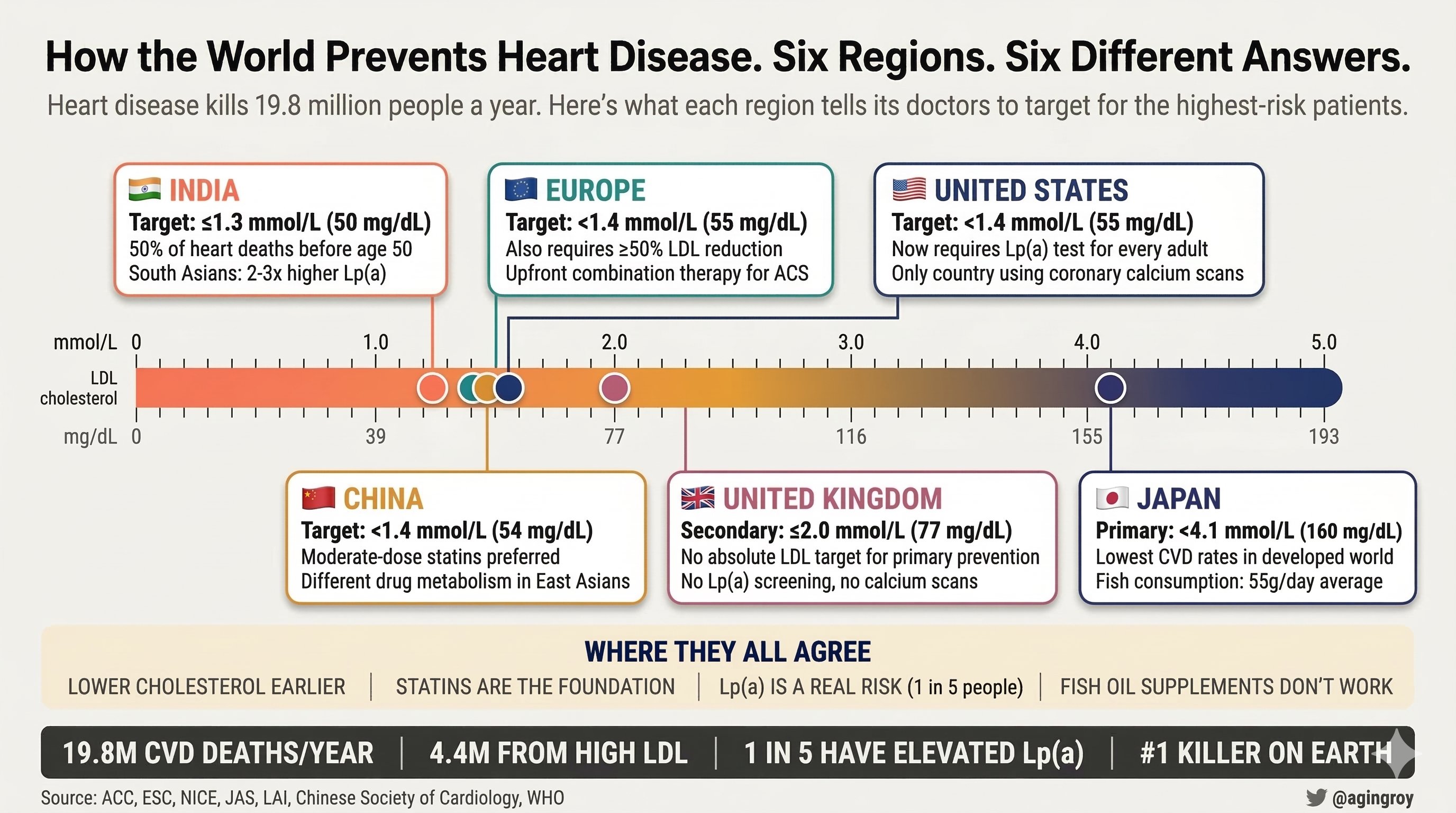
Six countries. Six different answers to the same question: how do you prevent a heart attack? Heart disease kills 19.8 million people a year. More than any other cause. Every major medical body has a rulebook for preventing it. They don’t agree.
The US (@ACCinTouch, @American_Heart) just updated its guidelines for the first time in 8 years. → They now require every adult be tested for Lp(a), a genetic risk factor that affects 1 in 5 people and doesn’t respond to diet or exercise. If yours is elevated, your heart attack risk at least doubles. Most people have never been tested. Europe (@escardio) also recommends testing. The UK? Doesn’t mention it. Cholesterol targets tell an even bigger story:
India targets the lowest numbers in the world: below 1.3 mmol/L (50 mg/dL) for high-risk patients, even lower for extreme risk. Half of India’s heart attack deaths happen before age 50. South Asians carry 2-3x higher Lp(a) levels than Caucasians.
Japan is the most conservative for primary prevention: 4.1 mmol/L (160 mg/dL). Japan also has the lowest heart disease rates in the developed world.
The US is the only country tying treatment decisions to coronary calcium scan scores. Europe and Asia don’t.
China uses lower statin doses than the West because East Asian populations metabolize the drugs differently. Same pill. Different blood levels.
The UK doesn’t set an absolute cholesterol target for primary prevention. Uses percentage reduction instead. What they all agree on: lower cholesterol earlier in life, statins are the foundation, and fish oil supplements don’t work.
Source: https://x.com/agingroy/status/2033937569893752985?s=20
The text is actually from Twitter. Could you quote it to make that explicit ?
praluent gave me the ’ soft cough" that i get with some statins. I didn’t get the cough with Repatha but much more severe joint and muscle pain. I think you have to try them all to see what works for you.
I am not sure what the mechanism is for muscle/jt pain for pcsk9i as apposed to statins
My sides on Repatha lasted for 4-5 days only after the first shot. I want to try a longer interval between doses. Has anybody tried it yet? Does it make sense at all?
I found this study the most useful before I started taking statins. I started with the mindset that I wouldn’t have side effects and I didn’t. The same with Repatha. It’s not to say that side effects can’t happen, but it’s not always because of the statin. In the study, the side effects were real, and they stopped when they ceased taking the tablet. But the intensity of the side effects was the same whether they were on a statin or a placebo. And the adverse affects stopped whether they were stopping taking a statin or a placebo.
Presidents are not chosen by random selection, so you cannot ascribe their longevity to a treatment effect. Becoming the president is like becoming an Olympian: it doesn’t happen to just anybody.
Yes. Presidents are following the same path as all wealthy individuals. That means they are living to 95-100 when you can pay for the best treatments. Look at Munger and Buffet for example.
Not sure about billionaires but presidents have extremely stressful lives. Stress kills… but not presidents. Isn’t it odd?
Yep. In fact, I can’t think of a single medication I’ve really had side effects from. Nothing from statins, repatha or ezetimibe aside from massively lowering my LDL-C.
I do believe that some people are generally more sensitive than others though. But whether that’s because of physiological differences (CYP enzyme activities, receptor densities etc) or they are more/less susceptible to placebo/nocebo effects, I’m not sure. People don’t like to admit the latter one, but it doesn’t mean it’s not real.
I also suspect one difference is that their health is closely, actively, monitored by others. There are plenty of wealthy people who die young, die of preventable causes etc, which I presume is because they weren’t paying attention. We have a whole thread about celebrity deaths, as you know.
This doesn’t seem to be correct. There was a big study published in Science just this year:
https://www.science.org/doi/10.1126/science.adz1187
How heritable is human life span? If genetic heritability is high, longevity genes can reveal aging mechanisms and inform medicine and public health. However, current estimates of heritability are low—twin studies show heritability of only 20 to 25%, and recent large pedigree studies suggest it is as low as 6%. Here we show that these estimates are confounded by extrinsic mortality—deaths caused by extrinsic factors such as accidents or infections. We use mathematical modeling and analyses of twin cohorts raised together and apart to correct for this factor, revealing that heritability of human life span due to intrinsic mortality is above 50%. Such high heritability is similar to that of most other complex human traits and to life-span heritability in other species.
So really, it’s around 50%.
What we are getting better at is preventing early deaths - heart disease from statins and stents, cancers by removing stage 1 tumours, infections from antibiotics.
This is interesting, and I think it’s good to look at the guidelines which are most relevant to yourself.
The US certainly has the best experts and evidence - let’s not pretend otherwise. So as a “go to” this is the one I’d follow if you have the resources.
Indians seem to have horrible genetics in terms of CVD susceptibility. On average, they generate plaque 10 years before a western population at the same LDL-C. So targeting lower LDL-C makes total sense IMO, especially when they can accomplish it very cheaply and easily with generic drugs that they make locally. Huge benefit to cost ratio for them.
Japan has famously low rates of ASCVD, which seems highly related to lifestyle. (e.g. Japanese living in America have the same ASCVD risks as caucasians). And by the way, the infographic seems to be wrong, because Japan has plenty of CVD - the high salt diet, lots of hypertension etc still causes CVD.
On the other hand, the UK guidelines are the ones I would put the least faith in. The UK doesn’t use calcium scores as part of an assessment, likely because they are hopelessly short of CT scanners (8.8 scanners per million vs 26/m OECD average). And they have even less radiologists. Patients wait weeks for a cancer scan, let alone a CAC in a young and seemingly healthy person. They’re also cheapskates when it comes to medication. PCSK9i prescriptions are almost never given out. The prescribing criteria are insane (need LDL-C >190mg/dl after maximum statins and other drugs), and it’s prescribed only by specialists. Lp(a) testing is basically unheard of - treated like some sort of experimental, esoteric test rather than routine practice. So I would completely ignore UK guidelines, which are more of a reflection of their terrible system rather than good science.