Well 67 is higher than 60 but is it significantly higher? I wonder what the increase in risk of a CVD event would be with a 10 increase of APOB (over the optimal of 60) I have to assume very marginal if any? Just saying, but I have noticed some people in here being obsessed with having a certain number for a certain marker and in pursuit of perfection on one marker they end up crewing up some other marker or risk higher than normal side effects.
I started with ApoB of 89, and LDL-c of 124 (five months ago) and on my last test (three days ago) It showed LDL at 82 and ApoB at 72 (after doing 10mg Ezetimibe, and 1Mg Pita with no side effect that i could tell) and I’m on cloud nine already LOL. If I manage to get them both south of 70 with the same dosage and zero side effects, I wouldn’t care if they were 68 or 38 even though I’m fully aware that people are saying having them in the 30’s is best.
What I find in some cases is that let say if your LDL-C is 60-80 your risk of heart attack may be very low let say 7% (this is a made up number to make the point) and then you read studies where they say that if you lower it further to 30-40 if decreases the chance by 10% % as an example) and people take this to be a lot where in fact is very small reduction from 7% chance to about 6.3%. So, while I agree we should shoot for optimal perhaps near optimal may be good enough especially if you happen to be one of the people that doesn’t respond very well to statins or Ezetimibe and it can be achieved with relatively low doses and no side effects.
As a matter of principle, I’ve come to hate perfection, and more times than not in pursuit perfection in one thing/marker most likely you’ll end up screwing up something else.
My concern is that many people may only look at their LDL # and think they are fine. However CVDz is multifactorial…. hsCRP, TG, LDL, ApoB, Lp(a)…… If the studies only discuss LDL they may give some a false sense of wellbeing.
Since we know sdLDL is more atherogenic vs larger LDL particles, it doesn’t help people to fully understand their situation if only LDL is reported.
@Paul will you share a little more about this?
My husband just said he needs to work on his inflammation, so this might be appealing for him to track at home.
hsCRP is a different animal altogether and should be checked routinely (IMO). Though most U.S. insurance companies do not want to pay for it in routine blood tests.
Every paper that I have read says that sdLDL is a better predictor of CVD than the regular LDL test. I do not understand why it is not part of a routine blood test.
"The direct sdLDL-C assay offers several practical advantages: it requires only a small volume of serum or plasma, delivers results within a short time, and remains stable even after multiple freeze–thaw cycles. Intraday variability is minimal, allowing blood samples to be analyzed at any time of day. These features have enabled the widespread adoption of direct sdLDL-C assays in large-scale cohort studies globally, where sdLDL-C has been consistently validated as a significant predictor of atherosclerotic CVD.3Ref2
Apob is even a better: it provides total particle count, which incudes other dangerous particles like VLDL. It has more predictive power than LDL cholesterol, and non-HDL cholesterol. It’s also more cost-effective, and is measured with more accuracy than sdldl. I could see using sdldl as a way to refine your risk profile, but only after taking care of the risk of high Apob.
Thanks
You are correct. I have no medical background and can only parrot what my AI queries tell me. If AI provides relevant citations, in this case 24, I tend to believe the AI.
"* Accuracy : The ApoB test is highly precise and internationally standardized, making it a very reliable measurement.
Stability : ApoB is significantly more stable than sdLDL in a collected blood sample, which makes it much more practical for routine clinical use.
Predictive Value : ApoB is a well-validated, superior predictor of cardiovascular risk compared to standard cholesterol tests. While sdLDL may provide additional insight into a person’s risk profile, ApoB remains the more established and clinically actionable marker for most people."
Many ( ? most ) doctors still do not measure lipids via ApoB (and have no idea about sdLDL)
If ApoB is above target that is almost certainly because there is a disproportionate amount of small particles - sdLDLs.
ApoB represents the total number of lipid particles per unit volume.
LDL assays typically report the weight of lipid particles/ volume - so no info regarding particle number
So you can measure either ApoB or sdLDL to get a better idea of risk.
Some good news on the horizon with obicetrapib. SYNERGISTIC EFFECT OF OBICETRAPIB AND EZETIMIBE ON CIRCULATING LDL PARTICLES | JACC
Which concludes:
Obicetrapib monotherapy, in combination with HIS, ( High Intensity Statin )and with HIS plus ezetimibe is safe, well-tolerated and produces robust reductions in LDL-C, LDL particles, and sdLDL-C
Obicetrapib should soon be available in Europe with the US to follow ( as usual )
Sure, I bought this device from the link and then you buy tubes. A finger prick fills the tube which is then inserted into the device which uses wifi to transmit results. ESR is just a measure of how much the blood in the tube settles over a specific amount of time. Reacts to supplements I take, illness and even if I measure after a workout it is elevated
Heart Attack Prediction: Why Your “Normal” Lipid Panel Might Be Lying to You
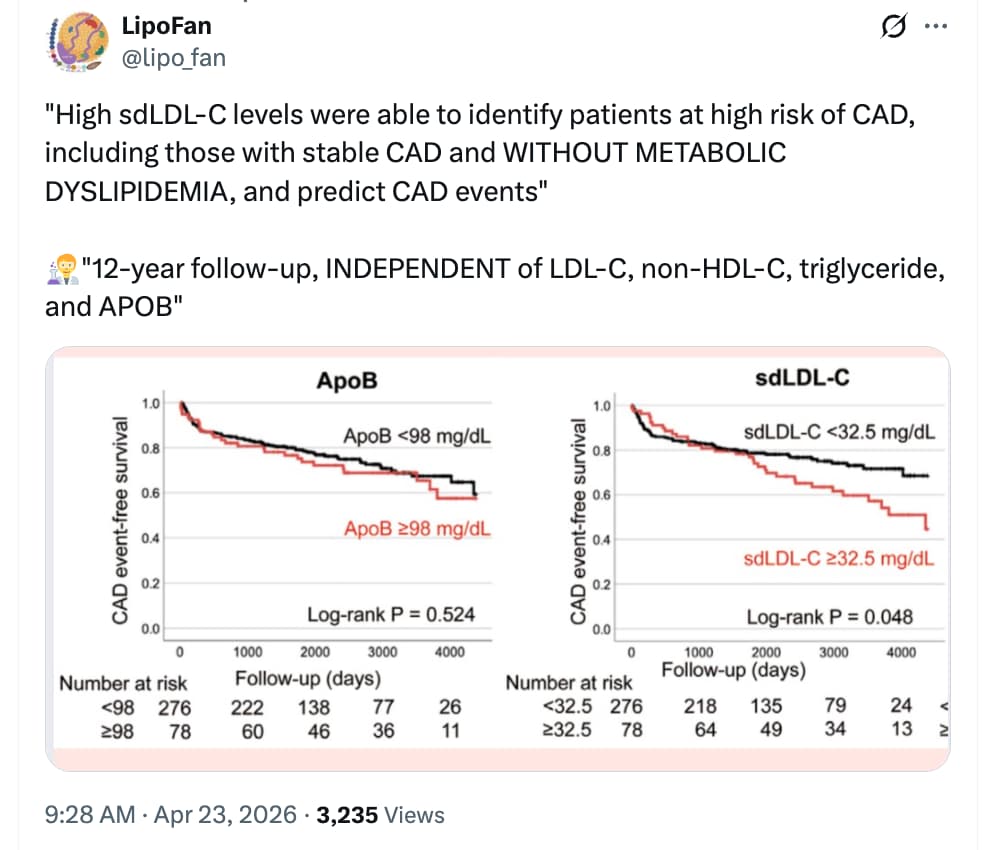
For decades, the “metabolic dyslipidemia” profile—low HDL and high triglycerides—has been the primary red flag for cardiovascular risk. However, a significant cohort of patients suffers recurrent heart attacks despite having “clean” lipid panels. A new 12-year longitudinal study published in the Circulation Journal reveals that a specific subtype of cholesterol, small dense low-density lipoprotein cholesterol (sdLDL-C) , acts as a “stealth” predictor of coronary artery disease (CAD) recurrence, even when traditional markers look perfect.
The research team followed 540 patients with stable CAD who appeared to have low metabolic risk: their HDL was at or above 40 mg/dL and triglycerides were below 150 mg/dL. Over a 12-year period, the study found that patients in the top quartile of sdLDL-C levels (≥32.5 mg/dL) had a 1.6-fold higher risk of experiencing a major cardiac event, such as a heart attack or the need for emergency revascularization.
The “Big Idea” here is particle quality over quantity. While standard LDL tests measure the total mass of cholesterol, they fail to distinguish between large, buoyant particles and the tiny, dense ones. These small particles are far more dangerous because they stay in the bloodstream longer, oxidize more easily, and slip into the arterial walls with ease. Crucially, the study found that traditional markers—including total LDL-C, non-HDL-C, and even the “gold standard” Apolipoprotein B (ApoB)—failed to accurately predict long-term recurrence in this specific “healthy” lipid group. Only direct measurement of sdLDL-C remained a significant predictor, even for those already taking statins.
Actionable Insights
Direct sdLDL-C Testing: Do not rely solely on estimated sdLDL-C or standard LDL-C panels. This study highlights that direct measurement (using assays like the Denka homogeneous assay) is superior for identifying residual risk in patients who otherwise meet target lipid goals.
Target Thresholds: Aim for an sdLDL-C level below 32.5 mg/dL. Patients exceeding this threshold showed significantly higher rates of acute coronary syndrome (ACS) and revascularization.
Monitor the sdLDL-C/LDL-C Ratio: A ratio ≥0.316 was identified as a significant risk threshold. This suggests that if more than roughly 32% of your total LDL is made of the small, dense variety, your risk profile is elevated regardless of your total LDL number.
Statin Limitations: Standard statin therapy may not sufficiently lower sdLDL-C in all patients. In this study, the risk remained significant for those on statins if their sdLDL-C stayed high, suggesting a need for more intensive or specialized lipid-modifying strategies.
Synergistic Risk: Combining high sdLDL-C with low HDL-C (≤45 mg/dL) increased the risk of recurrence by 2.7-fold. If you have both, aggressive intervention is warranted.
Institution: Showa Medical University, Tokyo, Japan.
Journal Name: Circulation Journal.
Impact Evaluation: The impact score (JIF) of this journal is approximately 2.2, evaluated against a typical high-end range of 0–60+ for top general science; therefore, this is a Medium impact journal within the cardiovascular specialty.
Needs a comparison with apob for predictive accuracy. Also, Apob is standardized and easily available. I’m not sure they;ve settled on a testing method yet for sdldl.
Small dense low-density lipoprotein cholesterol (sdLDL-C) is a specific subtype of LDL particles that are smaller and heavier than standard, large buoyant LDL particles. While regular LDL is often labeled “bad” cholesterol, sdLDL-C is significantly more dangerous because it is “cholesterol-poor,” meaning your total LDL-C levels can appear normal even if you have a high, dangerous concentration of these small particles.
Why sdLDL-C is Particularly Dangerous
Unlike larger LDL particles, sdLDL particles have unique characteristics that accelerate arterial damage:
Prolonged Residence Time: They stay in the bloodstream longer, giving them more opportunity to enter the arterial wall.
High Oxidation Potential: They are highly susceptible to oxidation and glycation, which triggers inflammation and the formation of atherosclerotic plaques.
Arterial Retention: They have a higher binding affinity to the “glue” of the arterial wall (proteoglycans), making them more likely to get stuck and cause blockages.
“Stealth” Risk: High levels can predict long-term coronary artery disease (CAD) recurrence even in patients whose standard markers—like total LDL, HDL, and triglycerides—look healthy.
Availability at Major Labs
Getting sdLDL-C measured is relatively easy, but it is not included in a standard lipid panel. You must specifically request advanced cardiovascular testing.
Quest Diagnostics
Quest measures this through their Cardio IQ® advanced testing line.
Specific sdLDL Test (Code 36406): Directly quantifies small dense LDL particles.
Ion Mobility (Code 91604): This is a high-resolution proprietary method that separates and counts particle subclasses (small, medium, and large) to identify atherogenic traits.
Ease of Access: You can often find these in comprehensive “Cardio IQ” panels, or they can be ordered as stand-alone tests by a physician.
Labcorp
Labcorp primarily utilizes Nuclear Magnetic Resonance (NMR) technology to evaluate these particles.
NMR LipoProfile® (Test Number 123828): This test directly counts the number of LDL particles (LDL-P) and identifies particle size subclasses.
Lipid Cascade (Test Number 123836): This is a “reflex” test where a standard lipid panel is performed first; if the LDL-C is below 130 mg/dL, the lab automatically triggers an NMR assessment to check for high particle counts that standard tests might miss.
Ease of Access: These are standard offerings but require your doctor to select the NMR-specific codes rather than a basic lipid screen.
Takeaway on “Ease”
While both labs offer these tests, they are “advanced” metrics. If you simply ask for a “cholesterol test,” you will likely get a calculated LDL-C value that does not reflect your sdLDL burden. To see this specific data, ensure your order includes either “Quest Cardio IQ sdLDL” or “Labcorp NMR LipoProfile.”
As a Longevity Research Analyst and Procurement Specialist, I have conducted a real-time market audit of the leading third-party laboratory resellers to identify the lowest-cost channels for Small Dense Low-Density Lipoprotein Cholesterol (sdLDL-C) testing.
As this is a blood diagnostic service, I have prioritized the Total Price and Specific Laboratory Codes (Quest 36406/91604 and Labcorp 123828) as the primary metrics for your analysis.
Top 10 Lowest-Cost Resellers for sdLDL-C & Advanced Lipid Testing
Rank
Vendor
Exact Tests Included
Total Price (USD)
Direct Link
1
GoodLabs
Cardio IQ® Lipoprotein Fractionation, Ion Mobility (Quest 91604)
Lowest Cost Winner:GoodLabs currently provides the most competitive a la carte pricing for Quest’s advanced fractionation ($38.00). This is highly recommended for biohackers looking to isolate the sdLDL-C marker without purchasing a $200+ comprehensive panel.
Shipping & Service Fees: * Walk-In Lab & Ulta Lab Tests: Typically charge a one-time “Lab Processing Fee” of approximately $8.00–$12.00 per order, not per test.
GoodLabs: Prices are generally “all-in” for the markers listed, but verify your local draw site (Quest/Labcorp) fee during checkout.
Own Your Labs: Prices are strictly for self-pay; they do not accept insurance but provide deep discounts for the “longevity community”.
Verification: All products listed are currently In Stock as digital requisitions valid at local Quest or Labcorp service centers.
Geographic Restrictions: Note that Own Your Labs and certain other resellers cannot provide services to residents of NY, NJ, RI, MA, or MD due to state laws regarding direct-to-consumer lab orders.
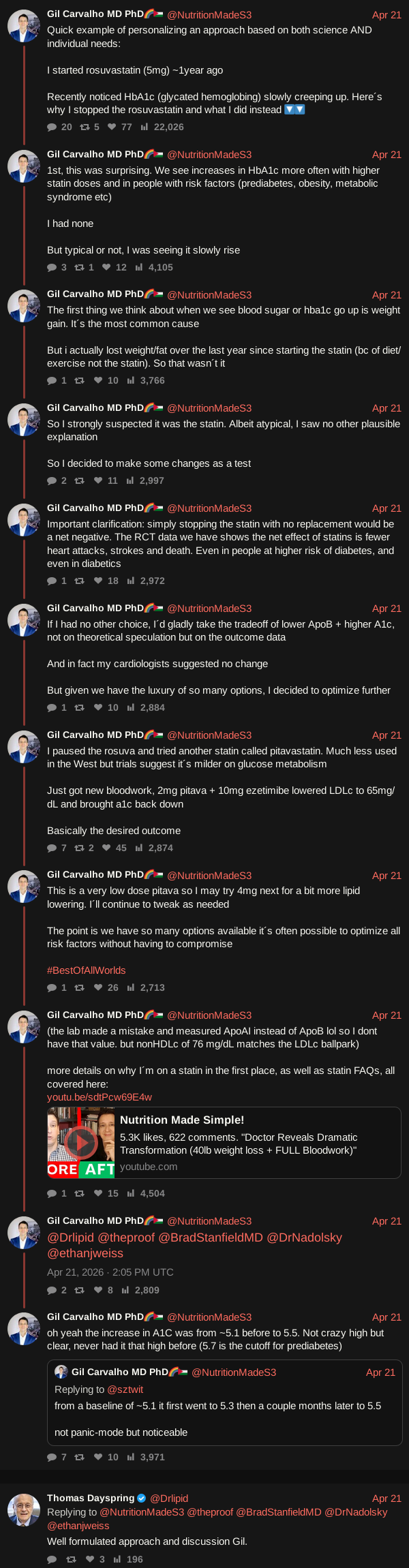
What can I say, I did a ton of research on pitavastatin years ago, switched to it personally (from atorvastatin) and have been a huge advocate of it ever since. I’m glad to see the world catching up to it (especially here in the West), as the impact on glucose is just one of its many, many advantages. But consensus changes slowly, and many are still stuck in the “all statins are the same” bugaboo (like the execrable Nick Norwitz and his anti-statin crusade). That said, all statins have their place, pros and cons. Even pitavastatin - one limitation is that it’s a median intensity statin, topping out at 4mg at the high dose, if you need more you have to go to atorvastatin or rosuvastatin.
Thanks to you (for real) I started Pita (first ever statin) about 7-8 months ago and I’m 100% satisfied and I love it. I also take EZE 10mg and my LDL-c has gone down by more than 40 points (while HDL has gone up by 10), ApoB down by 17 and I’m very close to sub 60 on both and that’s where I like to see them. I’m sure in due time I’ll get there. Btw, I’ve no side effects from either that I can tell.