I have a box of Livalo here that expired in 2017.
Do you guess it might still have enough efficacy remaining to use as a trial to see if I still react poorly to statins?
I have a box of Livalo here that expired in 2017.
Do you guess it might still have enough efficacy remaining to use as a trial to see if I still react poorly to statins?
I don’t think the expiry dates matters that much for meds:
You should do a blinded experiment to control for the placebo and nocebo effect which are powerful. Depending how long until you have the effect you’ll have to use one bottler longer until you check.
If I were ever able to get mine to 70, you’ll never hear me complain about it, ever LOL. Moving to 4mg might work but that seems to be the upper limit and sides may creep in at that level, so If I were you, I’d change nothing (for a while) unless it keeps moving higher (on your next test) especially given the fact that your joints seem to be loving Pita at 2mg. Just MO.
Scientific American magazine this month:
Immune system overreactions may be the true culprit of cardiac illness—and lifesaving drugs can calm them down
Doctors have been drilled for decades on the four big risks for heart disease, which kills more Americans every year than any other illness. The fearsome foursome: hypertension, smoking, high levels of “bad” LDL cholesterol and type 2 diabetes. Yet for just as long cardiologists have seen patients who have none of these problems die from heart ailments. And the heart specialists haven’t had the slightest idea why.
Up to a quarter of the people admitted to hospitals for heart attacks don’t have any of these four risk factors. Mysteriously, these “low-risk” heart disease patients actually have the worst outcomes. A 2023 analysis found that hospitalized acute coronary patients without any of the four hazards were 57 percent more likely to die compared with those who had at least one.
If the big known risk factors miss one in four patients, they still predict trouble as expected for the remaining three. That’s a good record. But it also means that of the roughly 920,000 Americans who die of cardiovascular disease every year, about 230,000 of them will have done so for no understandable reason.
This deadly puzzle has haunted cardiologist Paul Ridker for years. “I remember saying to myself that there must be some other fundamental determinant of heart disease,” says Ridker, who is director of the Center for Cardiovascular Disease Prevention at Brigham and Women’s Hospital in Boston.
Dozens of studies and clinical trials later, Ridker thinks he has found the missing piece. His work, along with that of other researchers, now suggests that chronic inflammation—a prolonged and body-damaging state of immune system activation—may be the hidden factor that accelerates cardiovascular problems to a dangerous and deadly state. When cholesterol builds up in the arteries, it shape-shifts into a sharp and jagged form the body no longer recognizes, provoking the immune system to wage war against it and blood vessels. It is a battle with no winners, and the wreckage it leaves behind ends in heart attacks and strokes.
Initially treated with skepticism, this idea now is becoming widely accepted by other scientists. Heart disease is “a disease of inflammation,” says Kathryn Moore, director of the Cardiovascular Research Center at New York University’s Grossman School of Medicine. And in the fall of 2025 the American College of Cardiology recommended that health-care providers routinely screen patients for inflammatory proteins.
Read the full story: The hidden cause of heart disease is inflammation
The ApoB result came back at 58. It’s usually about 10 points higher than LDL but this time is was only 1 point higher for whatever reason.
So if I understand correctly:
So, most likely, if you increase pitavastatin to the max dose (4 mg), you might get apoB back below 50?
Yes that’s all correct and that’s what I am hoping for. I am still waiting to hear back if my cardiologist will raise my dose to 4mg (they’re being slow on the health portal) but if it’s an issue, I’ll just order it myself from an Indian pharmacy so I can take the higher dose.
OK thanks. Stupid question but… can’t you just take two pills of 2 mg?
Yea but if I do that, I’d run out of them before I was allowed to refill the prescription
Ah OK, makes sense. Sorry, I’m not used to prescriptions ![]()

The prevailing clinical paradigm for managing cardiovascular disease—waiting for established atherosclerosis to manifest before aggressively intervening—is fundamentally flawed and actively costing lives. For decades, target thresholds for Low-Density Lipoprotein Cholesterol (LDL-C) have been physiologically mismatched to the actual biological requirements of human lipid homeostasis. The core thesis of the reviewed material is that “normal” cholesterol levels (100–130 mg/dL) are pathogenic, and the widely accepted clinical target of <70 mg/dL provides a false sense of security, allowing for the silent, continuous accrual of subclinical plaque.
Recent trial data from 2026 provides unequivocal evidence that aggressively lowering LDL-C to ultra-low targets (~40–55 mg/dL) yields profound cardiovascular mortality and morbidity benefits. The VESALIUS-CV trial demonstrated that high-risk primary prevention patients (diabetics without macroscopic plaque) achieved a 31% reduction in major adverse cardiovascular events when LDL-C was driven to a median of 44 mg/dL using PCSK9 inhibitors. Similarly, the ES PAVE trial reported a 33% relative risk reduction in major events when targeting <55 mg/dL versus the standard <70 mg/dL. Furthermore, imaging data from the PESA study indicates that atherosclerotic progression initiates at a plasma LDL-C threshold of approximately 50 to 60 mg/dL.
Achieving these targets does not strictly require cost-prohibitive biologics. The generic agent ezetimibe, which operates synergistically with statins by blocking intestinal cholesterol absorption, remains staggeringly underutilized, prescribed to only 6% of eligible patients. Ultimately, the data demands a proactive, aggressive shift: lipid-lowering intervention must occur earlier in the disease etiology, and physicians must titrate dual-therapy pharmacology to drive ApoB-containing lipoproteins well below conventional targets to successfully arrest atherogenesis.
| Claim from Video | Speaker’s Evidence | Scientific Reality (Current Data) | Evidence Grade | Verdict |
|---|---|---|---|---|
| PCSK9 inhibition dramatically lowers LDL-C and prevents MACE in high-risk primary prevention (diabetics without known atherosclerosis). | VESALIUS-CV trial (subgroup analysis presented March 2026) | Verified. A 2026 subgroup analysis of the Phase 3 VESALIUS-CV trial demonstrated that evolocumab reduced 3-P MACE by 31% (HR 0.69) in high-risk diabetic patients without ASCVD. Marston et al., TCTMD 2026 | Level B | Strong Support |
| Lowering LDL-C below 55 mg/dL is vastly superior to the 70 mg/dL target for secondary prevention. | ES PAVE trial (South Korea, 2026) | Source unverified in live search for full direct publication link, but trial data directly aligns with ACC 2026 abstracts detailing a 33% relative risk reduction in major events at the 55 mg/dL target. | Level B | Strong Support |
| Plaque formation strictly begins at an LDL-C threshold of approximately 50-60 mg/dL. | PESA Study (subgroup analysis) | Verified. Progression of Early Subclinical Atherosclerosis (PESA) study data indicates that subclinical atherosclerosis progression is rampant at conventional levels and ceases only when LDL is driven below the 50 mg/dL range. PESA Study, JACC | Level C | Plausible |
| Ezetimibe is cheap, effective, and severely underutilized (6% prescription rate). | Anecdotal / General cardiology statistics | Verified. A 2025 meta-analysis confirmed combination statin plus ezetimibe yields a 19% reduction in all-cause mortality over statin monotherapy, yet broad utilization remains clinically inadequate. Mayo Clinic Proceedings 2025 data | Level A | Strong Support |
| Soluble fiber (psyllium husk) actively lowers LDL cholesterol. | General scientific consensus | Verified. A 2025 dose-response meta-analysis confirms psyllium supplementation significantly decreases LDL-C (Weighted Mean Difference: -8.55 mg/dL). Genes & Nutrition, 2025 | Level A | Plausible |
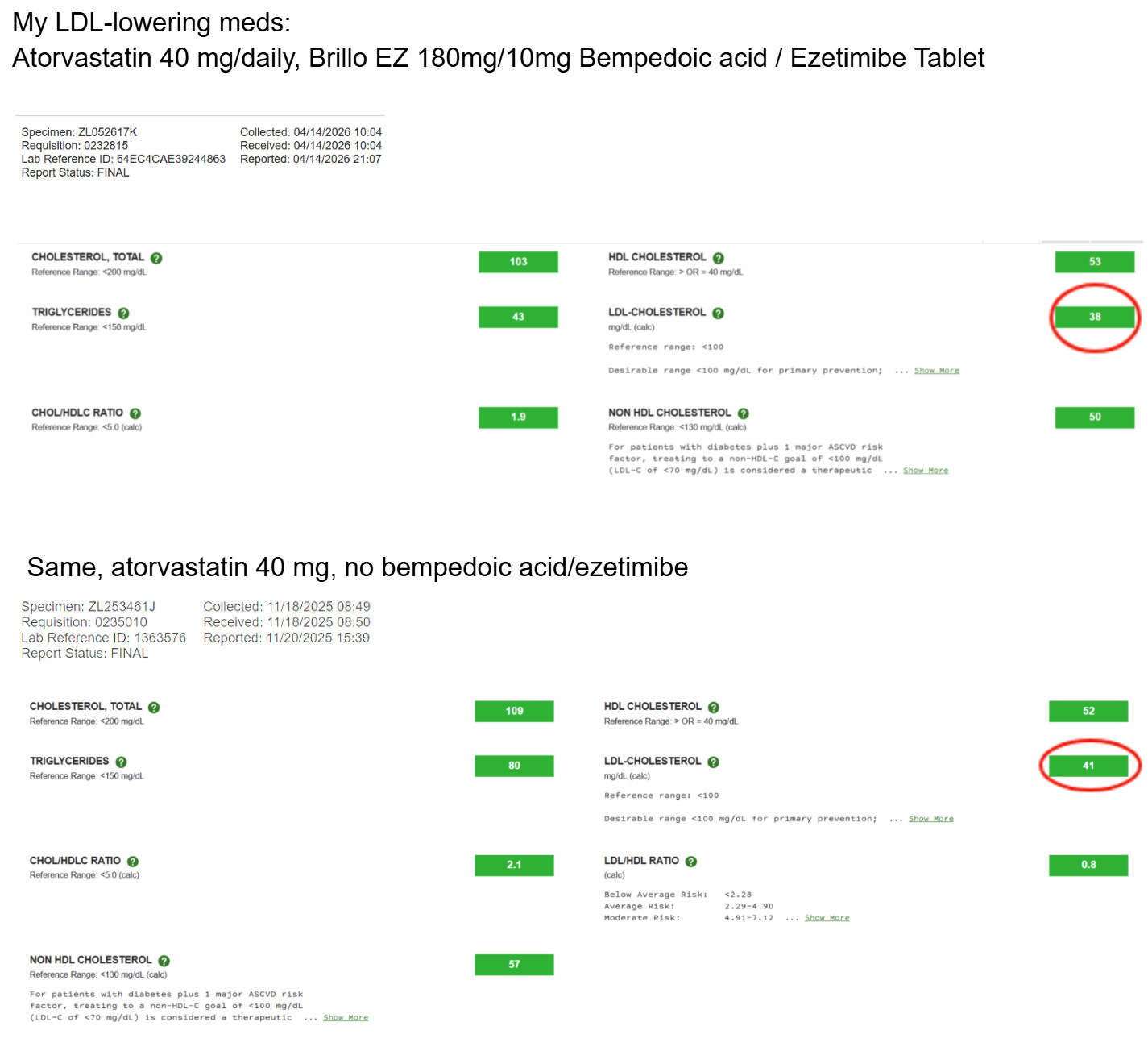
Statins + ezetimibe has been very effective for me. On august 2025, my LDL was 89mg/dL on 10mg rosuvastatin, 6 months later, my LDL is 27mg/dL on a combination of 10 mg rosuvastatin and 10mg ezetimibe.
I have been in the lower is better camp for a long time. Nice to see some justification
IMO: Body weight and exercise do lower LDL, but their effects are modest, and genetics typically dominates the picture for where someone’s LDL actually sits. I believe diet is secondary to these. (Except your diet must allow you to maintain a low BMI.) So take Brillo EZ first, and if that doesn’t do the trick, add a statin.
Unfortunately, I don’t have access to records going back to when I started on atorvastatin, which was decades ago. I stopped using Brillo EZ just because I ran out and forgot to order some more. I recently ordered some more Brillo EZ from India, and I will start taking it again.
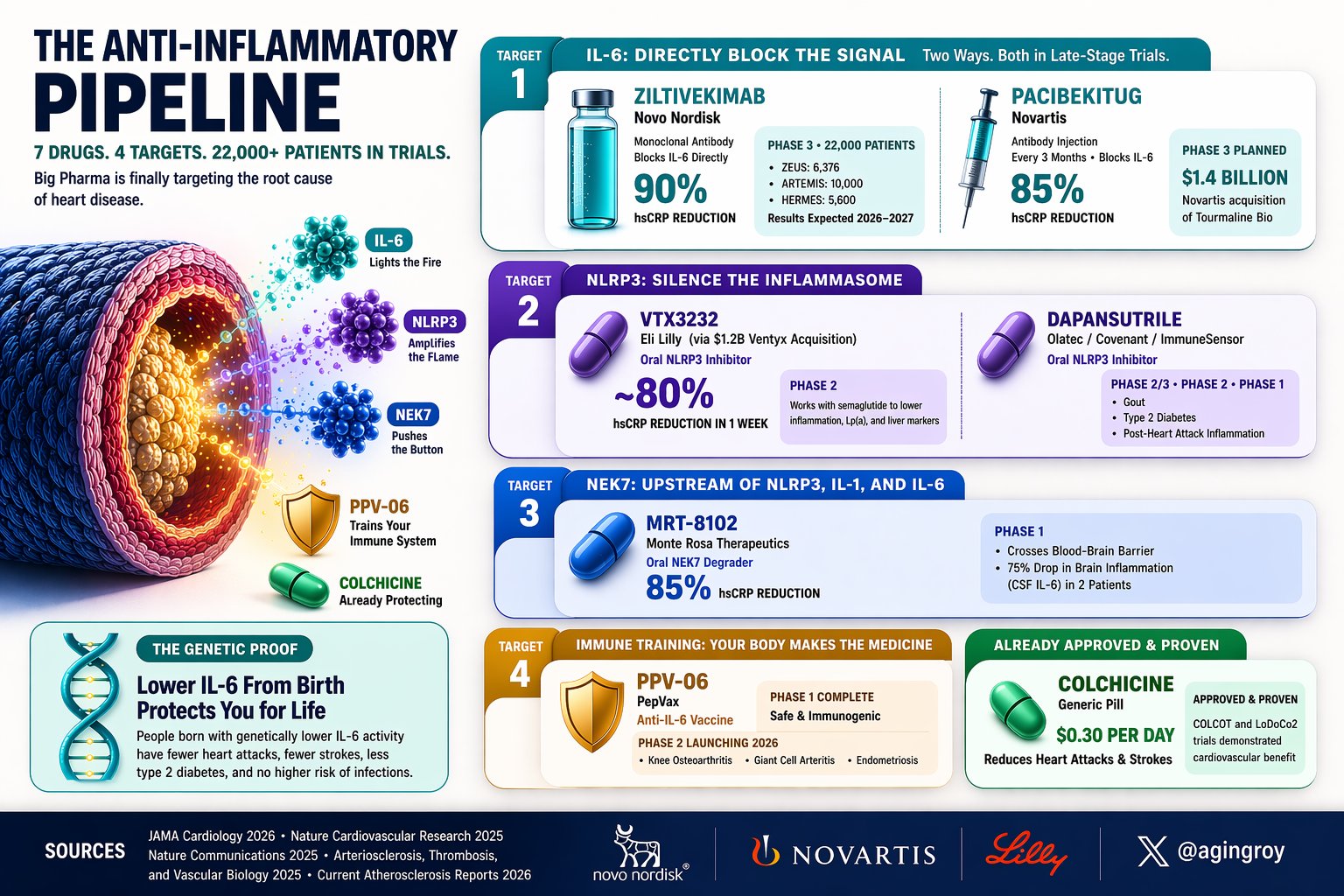
Your doctor measures cholesterol. They don’t measure the molecule that drives most of the remaining risk for heart disease.
It’s called IL-6. It fuels chronic inflammation. For the first time, drugs targeting it are in massive trials. 7 programs. 4 biological targets. 22,000+ patients enrolled.
The injectable IL-6 blockers:
→ Ziltivekimab ([@novonordisk (https://x.com/novonordisk)) drops hsCRP by 90%. Three Phase 3 trials running (ZEUS, ARTEMIS, HERMES), 22,000 patients. Results 2026-2027.
→ Pacibekitug ( @Novartis , $1.4B Tourmaline acquisition) cuts hsCRP 85% with one shot every 3 months.
The oral pills:
→ VTX3232 ( @EliLillyandCo, $1.2B Ventyx acquisition) is an NLRP3 inhibitor. Reduced hsCRP ~80% in the first week. Combined with semaglutide, it beat GLP-1 drugs alone on inflammation and Lp(a).
→ MRT-8102 (@MonteRosaTx) degrades NEK7, upstream of the whole cascade. 85% hsCRP reduction. Crosses the blood-brain barrier, dropping brain inflammation 75% in two patients.
→ Dapansutrile: another NLRP3 inhibitor, Phase 2/3 for gout, diabetes, and post-MI inflammation. The wildcards:
→ PPV-06 isn’t a drug. It’s a vaccine that trains your immune system to make its own anti-IL6 antibodies.
Phase 2 launching 2026.
→ Colchicine: already approved, $0.30/day. Proven to reduce heart attacks (COLCOT, LoDoCo2). Most cardiologists still don’t prescribe it.The genetic proof: Mendelian randomization (Nature Cardiovascular Research, 2025) shows people born with lower IL-6 have fewer heart attacks, fewer strokes, less diabetes. No increase in infections.
Your DNA running a lifelong clinical trial. The next risk factor your doctor will test isn’t cholesterol. It’s inflammation.
Source: https://x.com/agingroy/status/2045919203949977773?s=20
I wanted to test IL6 once but I think it was a pretty expensive test so I didn’t bother. I think it mirrors CRP and ESR well enough
Checking on how closely synchronized these inflammatory markers are:
In clinical practice and geroscience, Interleukin-6 (IL-6), C-reactive protein (CRP), and Erythrocyte Sedimentation Rate (ESR) are distinct markers that represent different stages and timescales of the inflammatory cascade. While they are correlated, they are not interchangeable due to differences in kinetics, sensitivity, and biological drivers.
The relationship between these markers is hierarchical and temporal. To understand if one can replace the others, one must analyze their positions in the biological response to a stimulus (e.g., infection, trauma, or cellular senescence).
For general screening of systemic inflammation or “inflammaging,” hs-CRP (high-sensitivity CRP) is the clinical gold standard. However, testing only one marker can lead to diagnostic blind spots.
In most outpatient and longevity contexts, hs-CRP is sufficient. It is more sensitive than ESR and more stable than IL-6. It is highly predictive of cardiovascular risk and all-cause mortality (Ridker et al., 2018).
IL-6 is used when a clinician needs to see the “real-time” inflammatory drive before the liver has responded, or in specific conditions like:
Despite being “old fashioned,” ESR is preferred or used alongside CRP in specific autoimmune conditions where CRP might remain paradoxically low, such as:
| Marker | Biological Source | Sensitivity | Specificity | Speed of Change | Primary Use Case |
|---|---|---|---|---|---|
| IL-6 | Immune/Senescent cells | Very High | Low | Rapid (Hours) | Acute crisis, SASP research |
| CRP | Liver (via IL-6) | High | Moderate | Moderate (Days) | General screening, CV risk |
| ESR | RBC/Fibrinogen | Low | Very Low | Slow (Weeks) | Chronic autoimmune monitoring |
A significant debate exists regarding CRP/ESR discordance. Studies indicate that up to 12.5% of patients show elevated CRP with normal ESR, or vice versa (Kushner et al., 2006).
If the goal is longevity optimization and screening, hs-CRP is the most practical and cost-effective single test. If an autoimmune condition is suspected, or if the user is monitoring a known inflammatory disease, testing both CRP and ESR is required to avoid missing discordant signals. Testing IL-6 is generally reserved for research-grade biological age testing or acute cytokine monitoring.
A nice LDL review. It seems clear that aggressively lowering your LDL lowers risk for MACE. However there are some of us who need more information to better appreciate our risk ( - aside from knowing Lp(a) and hsCRP.) Those with a low LDL may still have an ApoB that isn’t meeting suggested targets. An example is my own situation. High dose Rosuvastatin + Ezitimibe have lowered my LDL to 39. Nice, but my ApoB is still at 67… significantly higher than ideal (<60). This is because I have a type B lipid profile… skewed to having relatively more small dense LDLs (sdLDLs) which are more atherogenic than relatively larger LDLs. Theory goes that sdLDLs are more easily able to enter the vascular wall where the resulting biochemistry creates plaque. I would like to see all these articles on LDL goals and targets also discussing the need for ApoB consideration.
Well 67 is higher than 60 but is it significantly higher? I wonder what the increase in risk of a CVD event would be with a 10 increase of APOB (over the optimal of 60) I have to assume very marginal if any? Just saying, but I have noticed some people in here being obsessed with having a certain number for a certain marker and in pursuit of perfection on one marker they end up crewing up some other marker or risk higher than normal side effects.
I started with ApoB of 89, and LDL-c of 124 (five months ago) and on my last test (three days ago) It showed LDL at 82 and ApoB at 72 (after doing 10mg Ezetimibe, and 1Mg Pita with no side effect that i could tell) and I’m on cloud nine already LOL. If I manage to get them both south of 70 with the same dosage and zero side effects, I wouldn’t care if they were 68 or 38 even though I’m fully aware that people are saying having them in the 30’s is best.
What I find in some cases is that let say if your LDL-C is 60-80 your risk of heart attack may be very low let say 7% (this is a made up number to make the point) and then you read studies where they say that if you lower it further to 30-40 if decreases the chance by 10% % as an example) and people take this to be a lot where in fact is very small reduction from 7% chance to about 6.3%. So, while I agree we should shoot for optimal perhaps near optimal may be good enough especially if you happen to be one of the people that doesn’t respond very well to statins or Ezetimibe and it can be achieved with relatively low doses and no side effects.
As a matter of principle, I’ve come to hate perfection, and more times than not in pursuit perfection in one thing/marker most likely you’ll end up screwing up something else.