I’m expecting it to be lower ![]()
1 Like
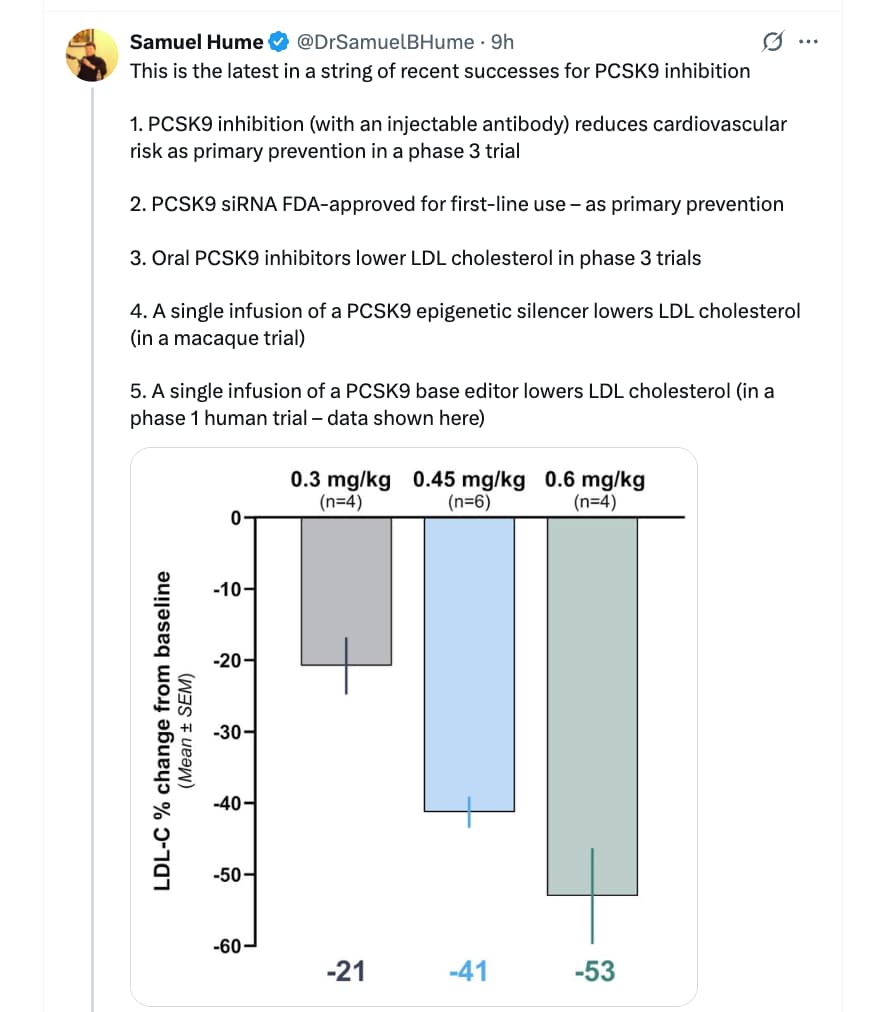
Nick Norwitz our lovable mischief maker has another curveball interview with noted skeptic cardiologist Bret Scher. They get into the PCSK9i and Alzheimer Disease MR study, statins and GLP-1RA and other areas.
I Interrogate a Cardiologist | Dr. Bret Scher on Cholesterol, Heart Disease & Alzheimer’s (Nick Norwitz)

2 Likes
When I was taking rapamycin daily (1mg daily 2 weeks, 1 week off), my hsCRP went down from 0.3 to 0.15. Unfortunately, I don’t have weekly tests to track it closely, but at the time I was doing monthly labs and the decrease seemed pretty stable.
Now that I’ve paused rapamycin, my hsCRP usually sits between 0.2 and 0.3 again. Very small fluctuations, probably insignificant and maybe hard to say it was just rapamycin.
3 Likes
Why did you pause Rapa after 1mg/2 weeks - 1 week off?
@relaxedmeatball
I looked up labs when crp was tested…
HS CRP .7 03/2018
CRP .8 07/2018
does not say it was HS, so I’m calling it out incase it makes a difference).
HS CRP 1.0. 01/2022
HS CRP .9 07/2022
CRP (not HS). 1.3 12/2022
HS CRP .90 03/2023
Started colchicine summer of 2023
Started rapa spring of 2024
CRP ‘cardiac’ .7 07/2024
CRP ‘cardiac’ .75 02/2025
PS
@RapAdmin, or everyone,
did anyone wind up finding a good program to keep track of our labs?
4 Likes

Clinical Trial Overview
- A new clinical trial investigated the effects of exercise on artery plaque in patients with significant plaque buildup and angina, all of whom were on lipid-lowering treatments.
- Participants were randomly divided into two groups: a control group that received standard care advice and an intervention group that participated in a supervised high-intensity interval training (HIIT) program.
- The control group followed guidelines that included a healthy diet, smoking cessation, regular exercise, and management of blood pressure and glycated hemoglobin levels.
- The intervention group engaged in a structured HIIT program, which included treadmill or stationary bike workouts with specific heart rate targets.
HIIT Program Details
- The HIIT program consisted of a 10-minute warm-up at 60 to 70% peak heart rate followed by cycles of high-intensity and recovery periods.
- Each cycle included 4 minutes at 85 to 95% peak heart rate followed by 3 minutes at 60 to 70% peak heart rate, repeated four times, and concluded with a 5-minute cooldown.
- Participants completed this workout twice a week under professional supervision and were encouraged to perform additional HIIT exercises at home.
Results of the Study
- After six months, the study measured the plaque size in arteries, revealing no significant changes in the control group, while the HIIT group showed a notable reduction in plaque size.
- The largest lesion in the HIIT group reduced from an average of 49.5% of the artery lumen to 48.3%, indicating a 1.2% decrease in plaque size.
- This 1.2% reduction in plaque size is significant, as similar reductions in other studies have correlated with a 20 to 25% decrease in the risk of cardiovascular events.
Understanding Plaque Composition
- While plaque size reduction is important, the composition and structure of the plaque are critical factors that influence its stability and risk of rupture.
- Plaque can become more stable without necessarily shrinking, which means it could even increase in size while becoming less dangerous.
- Further research is needed to explore how different types of exercise, such as cardio versus weight training, affect plaque dynamics and overall cardiovascular outcomes.
Mechanisms Behind Plaque Reduction
- The HIIT group also exhibited significant reductions in body mass index (BMI) and waist circumference, suggesting that weight loss may contribute to the decrease in plaque size.
- Interestingly, there were no significant changes in hemoglobin A1c, LDL cholesterol, or APOB levels between the HIIT group and the control group, which is noteworthy given the established role of lipid-lowering treatments in reducing plaque.
- All participants were on lipid-lowering treatments, maintaining their LDL cholesterol around 80 mg/dL, a level known to halt plaque growth.
Implications for Future Research
- The study raises questions about the potential additive effects of combining exercise with lipid-lowering therapies to achieve more significant plaque regression.
- Future research is needed to determine if lower lipid levels combined with exercise could lead to faster plaque reduction or if both interventions operate through similar mechanisms.
- Understanding these dynamics is crucial for developing effective treatment strategies for patients with cardiovascular disease.
Conclusion and Further Resources
- The results of this trial are encouraging, indicating that HIIT may play a beneficial role in managing arterial plaque among high-risk patients.
- For additional insights on lowering APOB through lifestyle changes and effective workouts to reduce blood pressure, viewers are encouraged to explore related video content.
Note: Dear all: Just a quick clarification regarding the “peak heart rate” mentioned in the video. Multiple viewers asked if several minutes at 85-95% “peak heart rate” isn´t too strenuous, especially for patients with heart disease.
Although the study Methods aren’t entirely clear, it seems they performed a ramp test prior to the study to determine each participant´s exertion limit. This test started at a comfortable intensity, which was gradually increased every minute until the participant stopped due to exertion (or until VO2max was achieved).
It seems, then, that “peak HR” refers to the highest HR recorded during this test before the participant chose to stop it.
In HIIT, it is customary to calculate “maxHR” by subtracting age from 220. It appears “peak HR” used in this study is unrelated to this calculation, and is instead a personalized measure obtained empirically. In other words, two participants with the same age could have wildly different “peak HRs” depending on their condition. This allowed them to tailor the exercise to each person’s ability and tolerance.
Finally, the main takeaway from this study is that physical activity has the potential to deliver some plaque regression. The specifics (type and exact protocol used) may or may not be important (more work will be required to establish this).
Hope this makes sense and thanks to the attentive viewers for the inquisitiveness of bringing this to our attention.
Gil
6 Likes
I followed this schedule for about a year, but I recently paused rapamycin. I had minor surgery that damaged my glossopharyngeal nerve, and I was afraid that taking rapamycin would hinder the regenerative capacity. I plan to resume rapamycin by the end of the year, following the same schedule.
2 Likes
Beth, I am using this app, Carrot Care. It seems good. I use the free version, and I need to input my labs manually. But if I remember correctly, you can take a photo or upload external labs with the paid version. You can set reminders, etc. I am not saying it is flawless, but it does the work.
2 Likes
Thanks so much for sharing Beth! So it overall didn’t change much, but it’s nice and low and stable, which is awesome!
1 Like
Source: https://x.com/DrSamuelBHume/status/1974102926600618094
Related:
Amgen (NASDAQ:AMGN) today announced the Phase 3 VESALIUS-CV clinical trial met its dual primary endpoints demonstrating that Repatha® (evolocumab) significantly reduced the risk of major adverse cardiovascular events (MACE) in individuals without a prior history of heart attack or stroke. The landmark Phase 3 VESALIUS-CV trial enrolled over 12,000 high-risk patients, approximately 85% of whom were maintained on a high-intensity or moderate low-density lipoprotein cholesterol (LDL-C) reducing therapy. Patients were followed for a median of approximately 4.5 years.
Cardiovascular disease remains the leading cause of death worldwide. In 2017, the FOURIER study proved that Repatha reduced the risk of major cardiovascular (CV) events in people with established atherosclerotic disease (ASCVD) and a history of major cardiovascular events, such as heart attack or stroke. The VESALIUS-CV study was initiated to determine if Repatha could also reduce CV events in people without a history of heart attack or stroke. VESALIUS-CV now establishes that Repatha, added to statins or other LDL-C lowering treatments, significantly reduces cardiovascular events compared with standard therapy alone as primary prevention.
The VESALIUS-CV primary endpoints were time to first occurrence of a composite of coronary heart disease (CHD) death, heart attack or ischemic stroke as well as time to first occurrence of a composite of CHD death, heart attack, ischemic stroke or any ischemia-driven arterial revascularization. The results show that the primary endpoints were both statistically and clinically significant. No new safety signals were observed.
4 Likes
It seems a bit suspicious that they didn’t give out the numbers. How significant was the reduction in CVD events over the 4.5 year period? All they say is that it’s “statistically and clinically significant”, so let’s hope they aren’t polishing a turd.
3 Likes
Did you have any side effects when you took Rapa for 2 weeks consistently?
“ Full results from the trial will be presented at the American Heart Association Scientific Sessions on Nov. 8 as part of the session “Groundbreaking Trials in Cardiometabolic Therapeutics,” and will be submitted for publication in a peer-reviewed journal.”
2 Likes
Side effects? None, really. My blood sugar stayed low, lipids didn’t change, and I felt good overall. It was easier to maintain low body fat, and my allergies and seborrheic dermatitis basically disappeared. Something shifted. SB never returned with the same vengeance, and the allergies didn’t either, even after I stopped rapa.
2 Likes
It’s great to hear! I also take it continuously, 0.5 mg, with a similar break. Works well for me too.
3 Likes
A cardiologist told my friend if they combine certain foods at the same meal, within a few months, they can get off statins.
I definitely know that the right foods help most people, but I’ve never heard there is something magical that happens if they are consumed at the same meal, vs just eating the ideal foods 24/7.
Is this a thing?
1 Like
That seems unlikely to me but I’m not a cardiologist! I’m still not buying it though unless someone presents convincing evidence.
4 Likes
My BS detector went off loudly, but I’m always surprised by how much I don’t know ![]()
2 Likes
Anyone have any experience or thoughts on this service? And how it compares to others (pro and con)…


2 Likes