The absorption issue has been studied ad nauseum and there’s no evidence for it having any clinical relevance, though I’m aware that they keep saying it. A shame.
1 Like
Doesn’t inositol upregulate Phosphoinositide 3-kinase - Wikipedia ?
IP3 DAG Calcium Pathway - YouTube
Thanks for the reply and good to know that no evidence exists on that absorption issue.
Either way, for those who don’t want to add ever more supplements but are interested in those particular protective effects, that is a dish high in the IP6/Inositol combination.
Alzheimer’s disease
Alzheimer’s disease involves the progressive degeneration of the brain, severely impacting mental faculties.[16] Since the Ca2+ hypothesis of Alzheimer’s was proposed in 1994, several studies have shown that disruptions in Ca2+ signaling are the primary cause of Alzheimer’s disease. Familial Alzheimer’s disease has been strongly linked to mutations in the presenilin 1 (PS1), presenilin 2 (PS2), and amyloid precursor protein (APP) genes. All of the mutated forms of these genes observed to date have been found to cause abnormal Ca2+ signaling in the ER. Mutations in PS1 have been shown to increase IP3-mediated Ca2+ release from the ER in several animal models. Calcium channel blockers have been used to treat Alzheimer’s disease with some success, and the use of lithium to decrease IP3 turnover has also been suggested as a possible method of treatment.[17][18]
Once active, VPS34 phosphorylates the lipid phosphatidylinositol to generate phosphatidylinositol 3-phosphate (PtdIns(3)P) on the surface of the phagophore. The generated PtdIns(3)P is used as a docking point for proteins harboring a PtdIns(3)P binding motif. WIPI2, a PtdIns(3)P binding protein of the WIPI (WD-repeat protein interacting with phosphoinositides) protein family, was recently shown to physically bind Atg16L1.[60] Atg16L1 is a member of an E3-like protein complex involved in one of two ubiquitin-like conjugation systems essential for autophagosome formation. The FIP200 cis-Golgi-derived membranes fuse with ATG16L1-positive endosomal membranes to form the prophagophore termed HyPAS (hybrid pre-autophagosomal structure).[61] ATG16L1 binding to WIPI2[62] mediates ATG16L1’s activity. This leads to downstream conversion of prophagophore into ATG8-positive phagophore[61] via a ubiquitin-like conjugation system.
Okay, IP3 is common (and used in intracellular pathways). IP6 doesn’t seem to be common. It’s the number of phosphate groups attached
strong text

PTEN acts as a tumor suppressor gene through the action of its phosphatase protein product. This phosphatase is involved in the regulation of the cell cycle, preventing cells from growing and dividing too rapidly.[8] It is a target of many anticancer drugs.
The protein encoded by this gene is a phosphatidylinositol-3,4,5-trisphosphate 3-phosphatase. It contains a tensin-like domain as well as a catalytic domain similar to that of the dual specificity protein tyrosine phosphatases. Unlike most of the protein tyrosine phosphatases, this protein preferentially dephosphorylates phosphoinositide substrates. It negatively regulates intracellular levels of phosphatidylinositol-3,4,5-trisphosphate in cells and functions as a tumor suppressor by negatively regulating the Akt/PKB signaling pathway.[9]
1 Like
It’s unclear if inositol cleaves into PIP3 or inorganic phosphate, but it could happen, so I’d be careful
Thanks. It’s complicated but worth considering.
Glycosylphosphatidylinositol-specific phospholipase D1 (GPLD1) hydrolyzes inositol phosphate linkages in proteins anchored to the cell membrane. Mice overexpressing GPLD1 show enhanced neurogenesis and cognition
Interesting post! What about taking IP6 with Rapa? Any side effects?
I found this review/pro-opinion about myo-inositol. it could be a candidate substance for the ITP
4 Likes
From the paper
Factors that deplete inositol include:7 9 64 65
- Insulin resistance
- Elevated glucose levels
- Low sodium intake
- Caffeine (coffee, tea, etc)
- Kidney damage
- Intestinal damage
- Lithium
- Valproic acid
- Magnesium deficiency
5 Likes
The findings and insights from the people contributing to Rapamycin News are astounding. The contributors have greatly influenced the supplements and dosages that I take to stay healthy and hopefully extend my lifespan.
“Everything old is new again”
I notice daily clickbait articles and ads on my phone and computer.
Inositol was a minor fad way back in the days when I was following Durk Pearson and Sandy Shaw.
In any case, I remember taking inositol for quite some time. As with many of my supplements back then, I discontinued it because I felt no subjective results.
From the article, it is obvious that I was taking too low of a dose.
Maybe it’s time to revisit it.
This time I will take 4 grams daily for a while and monitor my glucose levels.
I think that inositol might be a good supplement for older people who gradually become more insulin-resistant
From other articles I have read this morning it may also have mental health benefits and may be a treatment for ADHD. Some forms of inositol may have anti-cancer properties.
5 Likes
@desertshores Huberman recommended myo inositol a few years ago. I took it for a while when I listened to him. I never noticed anything but I am thinking about starting again based on the paper.
Let us know what you find out!
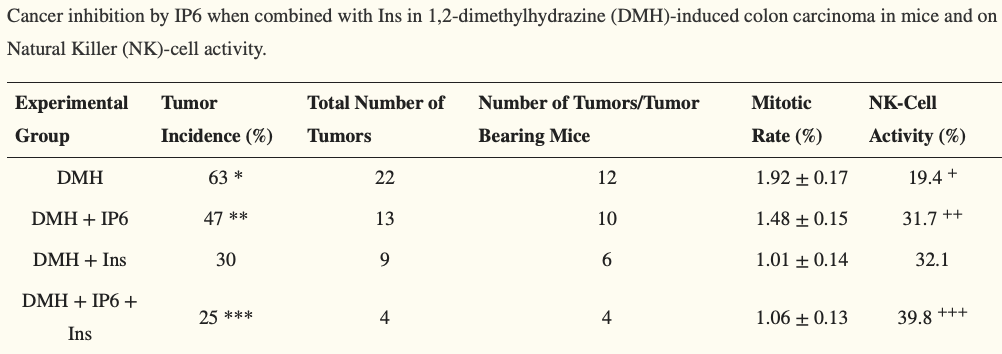
In that paper it looks like myo-inositol is better than IP6 and almost as good as the IP6+myo-inositol combo to prevent colon cancer in mice.
Yes, i have been taking this since huberman mentioned it for sleep. It’s had zero effect on my sleep but I’ve been continuing to take it only because I have a ginormous bottle of it. I was so excited to finish it and never see it again, but now I may think differently.
1 Like
If 4 grams daily of inositol does not lower my fasting glucose and A1c after 30 days I will stop taking it. I am starting tomorrow.
6 Likes
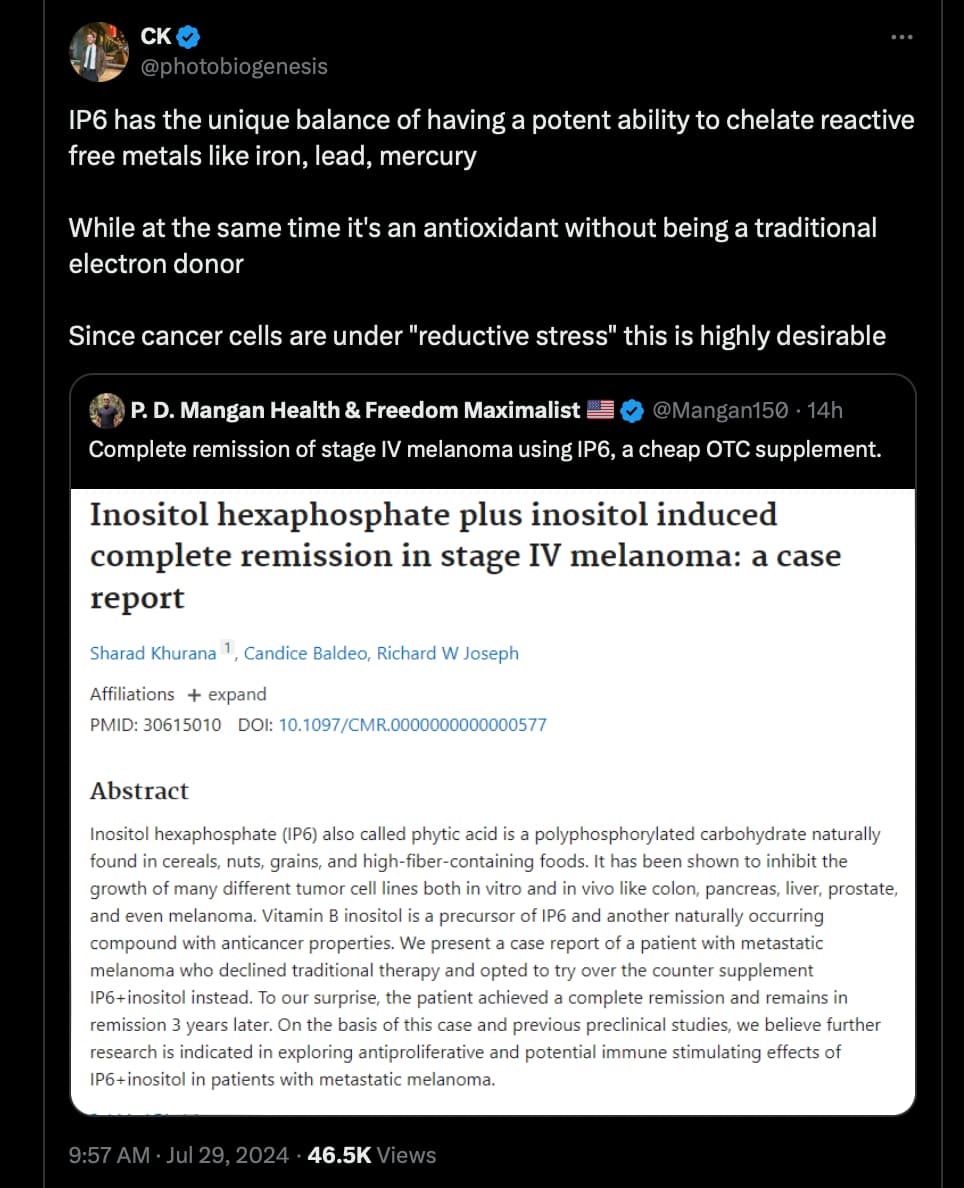
Does anybody know what dose the subject was taking? I can’t find it.
The patient was offered systemic therapy with both immunotherapy and targeted therapy but he declined both and instead elected to pursue the combination vitamin IP6+inositol (800 mg/220 mg), five tablets in the morning and five in the evening daily.
The patient went into complete clinical and radiological remission after being on the vitamin combination for 2 years (Fig. 2). Three years after relapse, the patient remains in complete remission and
continues to take IP6+inositol daily
2 Likes