Oh come on, you have to pee an extra 5 times a day and a couple more at night with empag.
1 Like
Not true for me, but I may be in a specific situation insofar as I have always peed with a fairly high frequency, because I make sure to always drink a pretty high volume of liquids, so I doubt empaglifozin would necessarily increase the already high frequency.![]()
Not for me either
Do they cite the Mendelian randomization showing increased lifespan in males and increased IQ?
If not then it’s a low-quality review.
2 Likes
I noticed no diuretic effect either - which may mean it isn’t really doing much.
If you notice a diuretic effect, isn’t that because you spike your sugars high and subsequently dump them. So everyone is going to be different.
And if you have a strong diuretic effect, definitely keep taking it and maybe up the acarbose or watch sugar intake.
3 Likes
There is no diuretic effect:
1 Like
Not for me either.
Has anyone read the paper? I’ve only been able to read the Abstract, which of course doesn’t mention Mendelian randomization.
1 Like
If it hasn’t already been posted - a short 16 minute talk at ARDD2025 about 8 short term studies experimenting with SGLT2i off-label in “normal” people (younger that 60, no diabetes, no CKD, no HF ):

This can produce valuable information, as there is the core argument, that SGLT2i are simply normalizing detrimental effects of diabetes/CKD.
6 Likes
Thanks for sharing. Gemini summary (bold mine):
- Overview & Aim: The presentation discusses evaluating whether FDA-approved SGLT2 inhibitors (traditionally used for diabetes, kidney disease, and heart failure) can be repurposed as gerotherapeutics to optimize healthspan and lifespan in individuals without these diseases [03:30], [10:23].
- Mechanism: SGLT2 inhibitors work by inhibiting glucose reabsorption in the kidneys, causing the body to excrete glucose through urine [03:44]. This pleiotropic drug lowers blood pressure and offers systemic metabolic and cardiac benefits [04:12].
- Systematic Review Findings: A massive systematic review screened over 44,000 articles, ultimately analyzing 536 human studies [07:19].
- Off-Label Data: Looking strictly at 8 completed trials involving younger, conventionally “healthy” cohorts (ages 30–60) taking the drug off-label, SGLT2 inhibitors showed highly positive, statistically significant improvements across multiple organ systems—specifically cardiovascular, metabolic, renal, hepatic, and adiposity systems [08:31], [09:49].
- Research Gaps: Current off-label data severely lacks insights into how SGLT2i impacts the reproductive, immune, and nervous systems [10:51].
- The HEARTS Trial: To fill these gaps, a multi-disciplinary, 6-month clinical trial is being launched in Singapore [11:53]. It will evaluate the effects of 10mg of daily SGLT2i on healthy individuals (ages 35–65) with an optimal BMI, focusing on VO2 max as the primary outcome alongside digital and biological biomarkers [12:11].
8 Likes
SGLT2i are helpful in heart failure. But is that mostly true only in people with relatively rare genetic defects?
Effects of SGLT2 inhibition on incident heart failure in carriers of cardiomyopathy-associated genetic variants
https://www.nature.com/articles/s41591-026-04439-x
“Among 12,685 patients for whom sequence data were obtained, 121 carried a cardiomyopathy variant (76 dilated cardiomyopathy, 25 hypertrophic cardiomyopathy and 25 arrhythmogenic cardiomyopathy). Over a median follow-up of 4.2 years, dapagliflozin lowered the risk of HHF more strongly in carriers (hazard ratio 0.18, 95% confidence interval 0.04–0.86) than in noncarriers (hazard ratio 0.70, 95% confidence interval 0.57–0.86; P interaction 0.03). Absolute risk reduction was 13.0% in carriers and 1.0% in noncarriers (P interaction 0.03). Most carriers (82%) had no prior HF, and in carriers without prior HF, treatment with dapagliflozin reduced the absolute risk of HHF by 12.8%, compared with a reduction of 0.6% in noncarriers (P interaction 0.01).“
5 Likes
That may (or may not) be ultimately true. But most people here would consider SGLT2i for generally longevity and not specifically heat failure - which is different than ASCVD.
Kidney function in “normal healthy” people declines every year by about 1% of it’s original state - starting from mid age (40/50). So by age 90 you could loose about 50% of your kidney function, despite doing most things right.
This is similar to the rationale for lowering LDL or blood pressure: it’s just a very common issue even in “normal” people. So there may be an incentive to take preventative action, such as SGLT2i. In addition there’s a mild effect on weight loss and blood pressure (which could benefit most “normal” people).
4 Likes
Well, if you are very old and very sick (with multiple co-morbidities), and so ill with HF that you are hospitalized, it’s good to know that SGLT2i can still massively help with ACM (all cause mortality), hospitalization and composite outcomes. Observational study.
Efficacy and Safety of SGLT2 Inhibitors in Heart Failure: Observational Evidence in Geriatric Patients-AGING-HF
“SGLT2i use was associated with lower risks of all-cause mortality (hazard ratio, 0.67 [95% CI, 0.46-0.98]; P =0.031), HF rehospitalization (hazard ratio, 0.64 [95% CI, 0.42-0.97]; P =0.037), and the composite outcome (hazard ratio, 0.60 [95% CI, 0.44-0.82]; P =0.001) at 1 year, after multivariable adjustment.”
3 Likes
What many here are more interested in, is the effect of SGLT2i in nondiabetic conditions and what the possible mechanisms might be.
Mechanisms of heart failure and chronic kidney disease protection by SGLT2 inhibitors in nondiabetic conditions
https://journals.physiology.org/doi/full/10.1152/ajpcell.00143.2024
“This review provides an analysis of the multifaceted mechanisms underlying the cardiorenal benefits of SGLT2i in HF and CKD outside of the T2D context. Eight major aspects of the protective effects of SGLT2i beyond glycemic control are explored: 1 ) the impact on renal hemodynamics and tubuloglomerular feedback; 2 ) the natriuretic effects via proximal tubule Na+/H+ exchanger NHE3 inhibition; 3 ) the modulation of neurohumoral pathways with evidence of attenuated sympathetic activity; 4 ) the impact on erythropoiesis, not only in the context of local hypoxia but also systemic inflammation and iron regulation; 5 ) the uricosuria and mitigation of the hyperuricemic environment in cardiorenal syndromes; 6 ) the multiorgan metabolic reprogramming including the potential induction of a fasting-like state, improvement in glucose and insulin tolerance, and stimulation of lipolysis and ketogenesis; 7 ) the vascular endothelial growth factor A (VEGF-A) upregulation and angiogenesis, and 8 ) the direct cardiac effects.”
2 Likes
As much as I hate to add another daily pill to my regimen, it’s hard to ignore SGLT-2 inhibitors.
Going to a low-dose version because weight, A1c, glucose and insulin sensitivity are already well under control through a GLP1 agonist. In addition, studies that activate the following pleitropic effects :
-Ampk activation
- Ecm remodeling of kidney, heart, liver
- senomorphic effects
Show that these are already activated at the minimum dose, as long as SGLT-2 receptors are sufficiently saturated to induce glucose excretion.
Curious about where egfr settles for me. After about 8 months on a GLP1/GCGR agonist, egfr rose to the mid 110s, supporting preliminary evidence that these drugs increase egfr through non-pathological hyperfiltration. SGLT-2 inhibitors initially lower it, although they stop the decline.
6 Likes
EGFR is just estimated. Any time you lose muscle mass or even just decrease protein intake, your eGFR will go up because the estimate is based on creatinine which is a muscle breakdown product.
Just like taking creatine will bring eGFR down. So would a hard workout before your blood draw.
Some labs are valuable to trend even while normal but trying to get meaning out of trending creatinine or eGFR is fraught when things are changing.
I say this because GLP-1s usually reduce muscle mass so would be expected to increase eGFR but not actually effect GFR. Even without weight loss, I would expect some effect only on the eGFR. Doesn’t necessarily mean your GFR didn’t go down, but you would need a better test to actually know.
4 Likes
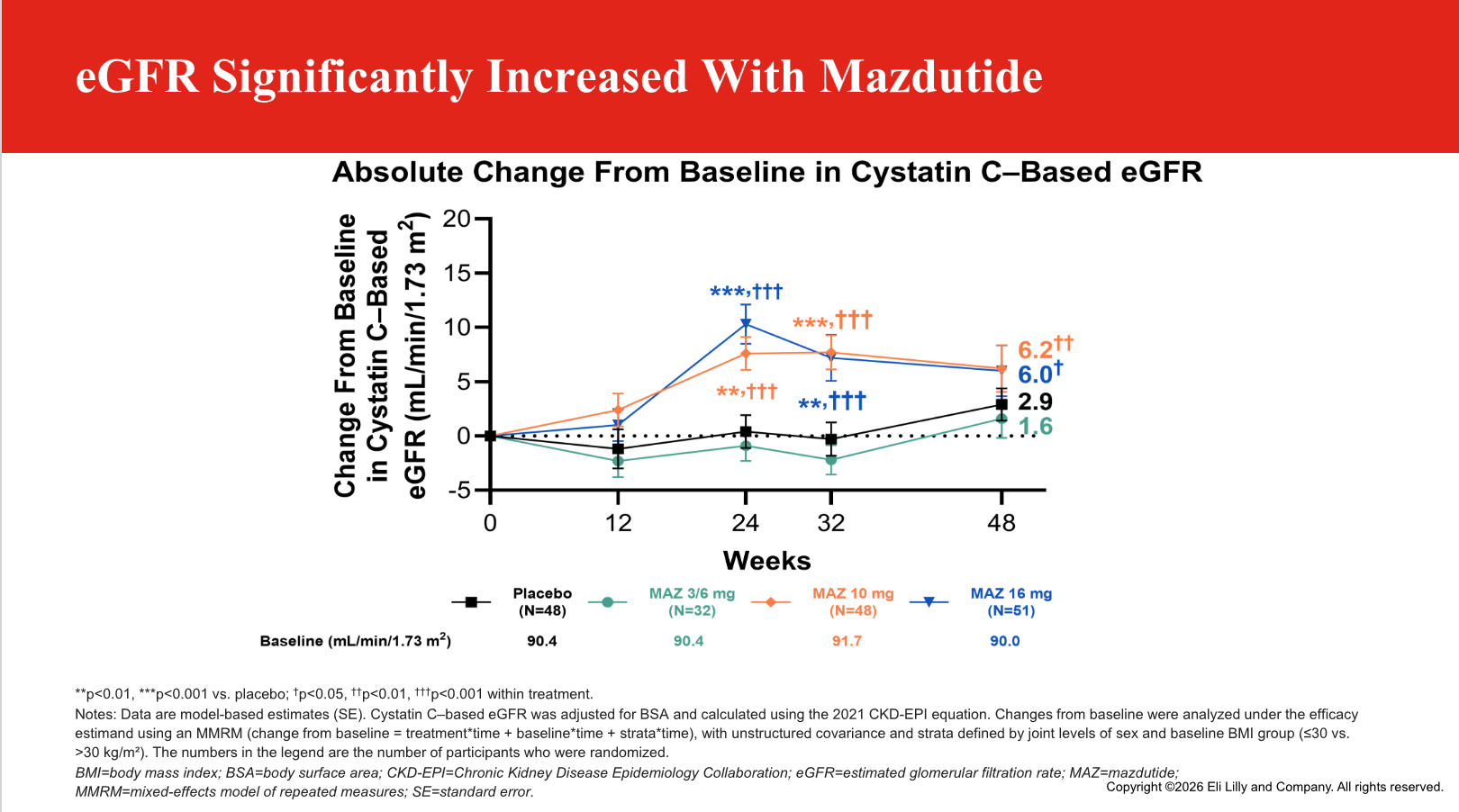
That’s good to know, about egfr, thanks. I’m basing my guess on this slide from phase 3 data on Mazdutide, which demonstrated statistically significant increase in Cystatin C-based eGFR by the end of the treatment period.
Note that:
- peak eGFR increases for the 16 mg dose actually maxed out around Week 24, with weight loss not yet at a plateau.
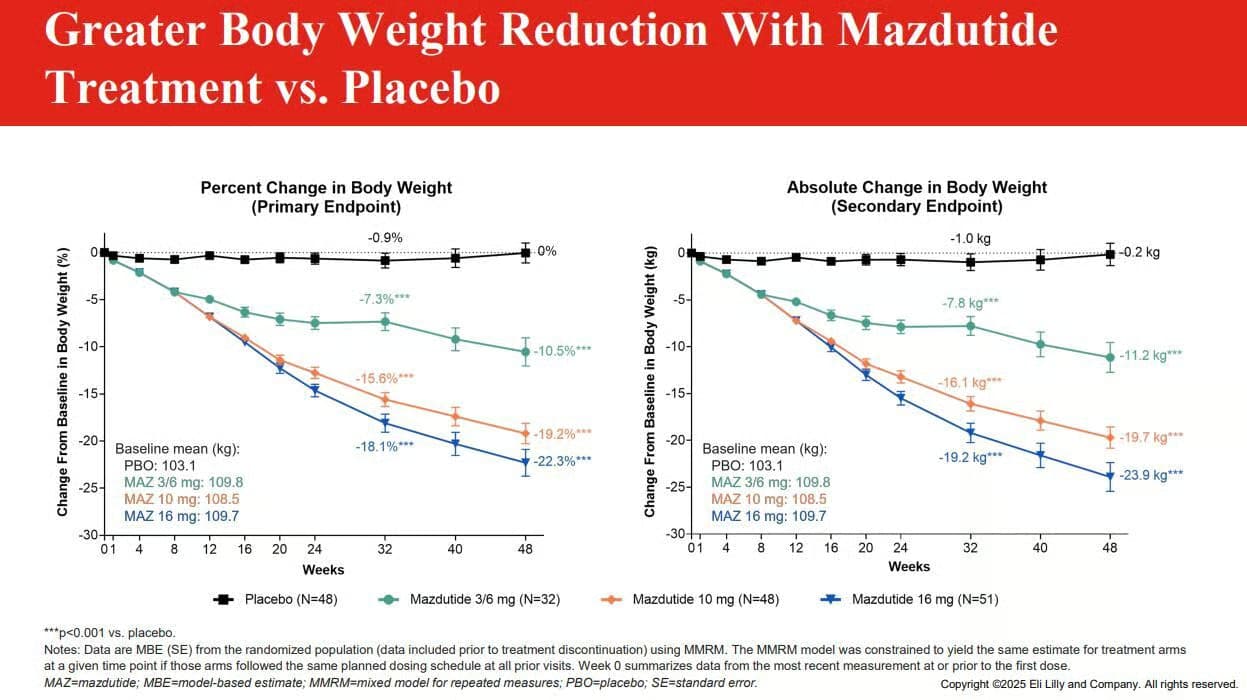
- egfr increase plateaus at higher doses, while weight loss itself shows no plateau
- increase in eGFR happens with a decrease in urine albumin-creatinine ratio (UACR)
All of this suggests a mechanism of increasing egfr independent of weight loss. Looking forward to the published data from Mazdutide and other GCGR agonists, hopefully some time this year.
Slides from ADA 2026:
Weight loss curve for mazdutide
5 Likes
New pre-print paper showing that reducing the dose of canagliflozin in female mice does NOT reduce neurodegeneration (thus suggesting the lifespan enhancement in males but not females is also truly sex-specific and not due to the fact that the drug accumulates to much higher levels in female mice)
6 Likes
Females don’t need any life extension. They live longer than us already LOL
1 Like
New paper pointing to another possible benefit of SGLT2i: slowing down aortic stenosis. Evidence found in mice and observational studies.
https://www.jacc.org/doi/10.1016/j.jacbts.2026.101595
One of the largest studies addressing the relationship between SGLT2i use and the natural history of AS was a multicenter observational retrospective analysis conducted by Shah and colleagues in 2025, which included 11,698 patients with early AS stages, ranging from aortic sclerosis to moderate AS, who underwent serial echocardiographic evaluation over a 3-year follow-up period.13 Among these individuals, 448 patients were treated with SGLT2i for diabetes management. After adjustment for baseline characteristics and comorbidities, SGLT2i therapy was associated with a significantly lower risk for progression to severe AS (HR: 0.61) compared with patients not receiving SGLT2i.13 In addition to the reduced risk for developing severe disease, the rate of echocardiographic progression (assessed by changes transvalvular gradients and valve area over time) was slower in the SGLT2i–treated cohort.
9 Likes