Off the top of my head I can’t think of a single research study on SGLT2 inhibitors in otherwise health individuals (perhaps @adssx can remember if there are any in healthy people).
There was an AgelessRx trial on canagliflozin in healthy people earlier this year. It was a small n trial, so I don’t know if they were powered for any reasonable efficacy signal, but I suppose we’ll learn what they found eventually.
“we don’t simply assume benefits from biomarkers”: then how do you measure benefits?
All drugs need to go through phase 1 with healthy volunteers. So we have data on healthy volunteers. But these are biomarkers.
SGLT2i are actually an exception, as they’re approved for three conditions: diabetes, heart failure, and chronic kidney disease. So you can see that they improve glycemia for people with CKD but without diabetes and vice versa.
If someone asks a doctor to prescribe a SGLT2 drug, which SGLT2 medicine should one use? There are so many links and studies that it is difficult to find out the best option. Or is it even known yet?
Our best guesses now would be either empagliflozin (which I use), dapagliflozin or canagliflozin (ITP). Each has their own advantages and disadvantages.
SGLT2 has been identified as being overexpressed in a diverse set of cancers. Retrospective data has demonstrated a correlation between the use of SGLT2 inhibitors and a reduced incidence of lung cancer. We explored the association of SGLT2-coding gene SLC5A2 with the transcriptomic, genomic, immunological landscape and outcomes in a subset of solid tumors.
SCL5A2-H across all investigated tumors was associated with increased immune infiltrate and a T cell-inflamed phenotype in addition to improved survival in multiple cancer types. Future research on SGLT2 should delineate its role in cancer formation versus its association as a potential positive prognostic marker.
So high expression of SGLT2 (through the SLC5A2 gene) is associated with better immune response and improved survival in several cancers? This could imply that inhibiting SGLT2 might reduce these beneficial effects? Or did I misunderstand
Yes, with pleasure. For me, it is difficult to run in zone 2 at a meaningful speed. Even a minimal slope in “my” forest, where I always run, would catapult me into zone 3 or even higher. On the days when I take empagliflozin, my heart rate in cardio mode drops by 10-15 beats per minute, allowing me to run at a higher speed or overcome slopes without having to walk or leave zone 2 (which, in my case, ends around 130 bpm). And for those, who has difficulties running in zone 2 - knows, that is big change.
@adssx - hmm, I read it as SGLT2i inhibiting cancer formation. If SGLT2 is overexpressed in cancer, inhibiting it seems like it should inhibit cancer rather than promote. And if SGLT2i promote T-cell infiltration of the tumor, then it’s promoting an immune response, and so increaing survival of the patient. That’s how I read it, but if course I could be wrong.
No, no noticeable changes. My resting HR is already rather low with 53 bpm, and no further improvement. It seems, that empagliflozin improves for me efficiency or cardio system.
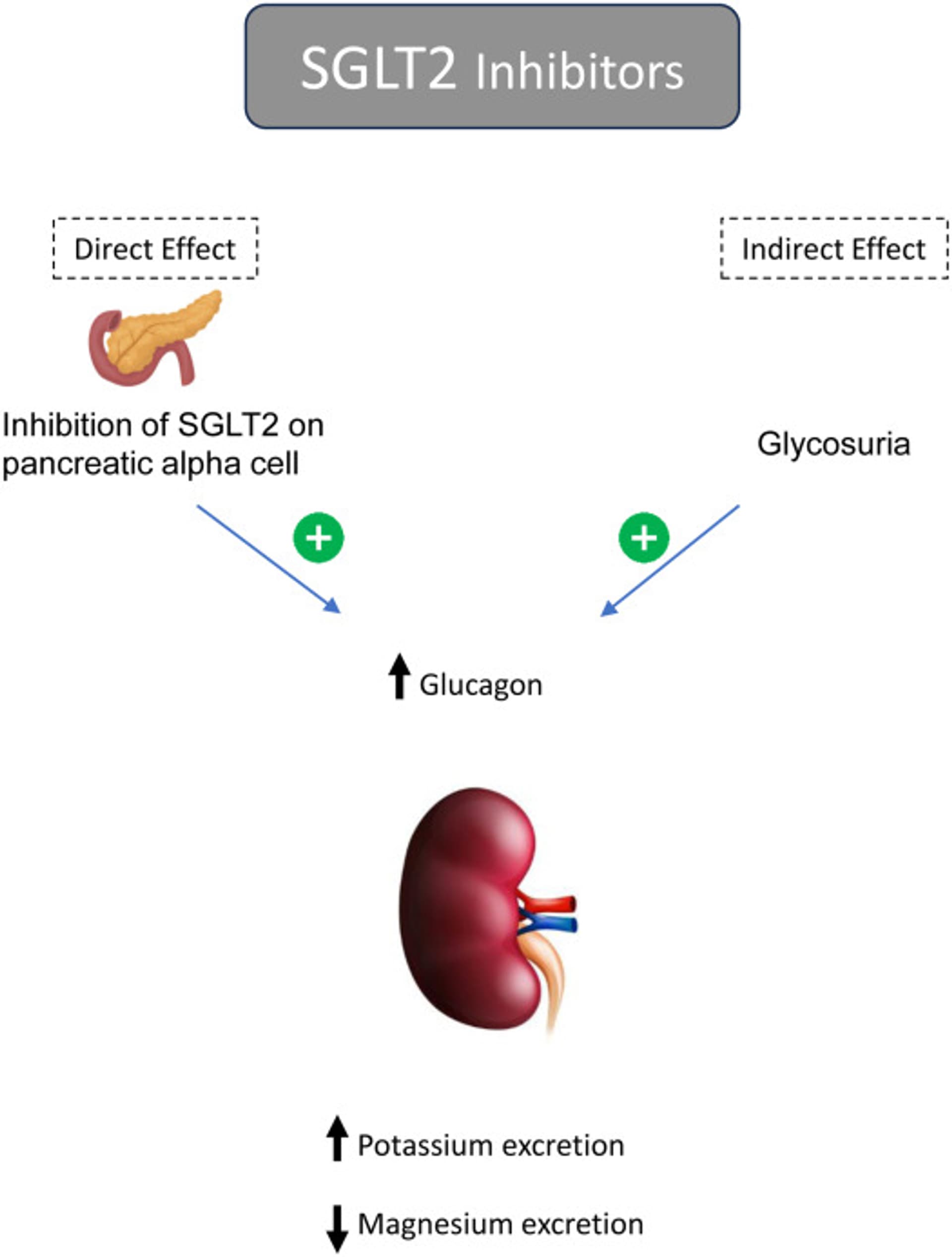
We have reported that initiation of SGLT2 inhibitors can dramatically improve severe hypomagnesemia in patients with or without diabetes. As noted in a recent review, meta-analyses of randomized clinical trials have reinforced that SGLT2 inhibitors decrease the risk of hyperkalemia and correct hypomagnesemia.
The beneficial effect of SGLT2 inhibitors on magnesium balance in patients with diabetes with or without hypomagnesemia has been noted as a class effect in recent meta-analysis data from randomized clinical trials. Some reports have demonstrated their role in treating refractory hypomagnesemia in patients with or without diabetes.
After propensity score matching, compared with the non-SGLT2i group (n = 2813), the SGLT2i group (n = 707) exhibited significantly lower recurrent IS rates (3.605% per year vs. 5.897% per year; hazard ratio: 0.55; 95% confidence interval: 0.34–0.88; p = 0.0131) and a significant reduction in all-cause mortality (5.396% per year vs. 7.489% per year; hazard ratio: 0.58; 95% confidence interval: 0.39–0.85; p = 0.0058). No significant differences were observed in the rates of acute myocardial infarction, cardiovascular death, heart failure hospitalization, or lower limb amputation.
Among 44 651 patients, 22 100 initiated SGLT2is, and 22 551 began DPP4is. After weighting, the incidence rate of MLO in the SGLT2i group was 3.8 per 1000 person-years, and it was 3.9 per 1000 person-years in the DPP4i group, resulting in an adjusted hazard ratio (aHR) of 0.82 (95% CI, 0.60-1.10). SGLT2i initiation was not associated with cirrhosis (aHR: 0.77; 95% CI, 0.55-1.06) or hepatocellular carcinoma (aHR: 0.99; 95% CI, 0.47-1.83) separately. Subgroup and sensitivity analyses did not yield significant results.
Our study helps fill this knowledge gap by indicating that SGLT2is do not lower the risk of cirrhosis or HCC compared with DPP4is. This finding is in contrast to previous research, including a systematic review and meta-analysis of randomized controlled trials showing that dapagliflozin improves liver studies, such as alanine aminotransferase (ALT) and aspartate aminotransferase levels,31 and the E-LIFT trial, which found that empagliflozin reduces liver fat and improves ALT levels in T2D and MASLD patients.
Disappointing paper on liver function. However, all the HR, even though not statistically significant, are on the side of SGLT2i benefits. We’ll have to wait for the ongoing trials of SGLT2i in NAFLD…
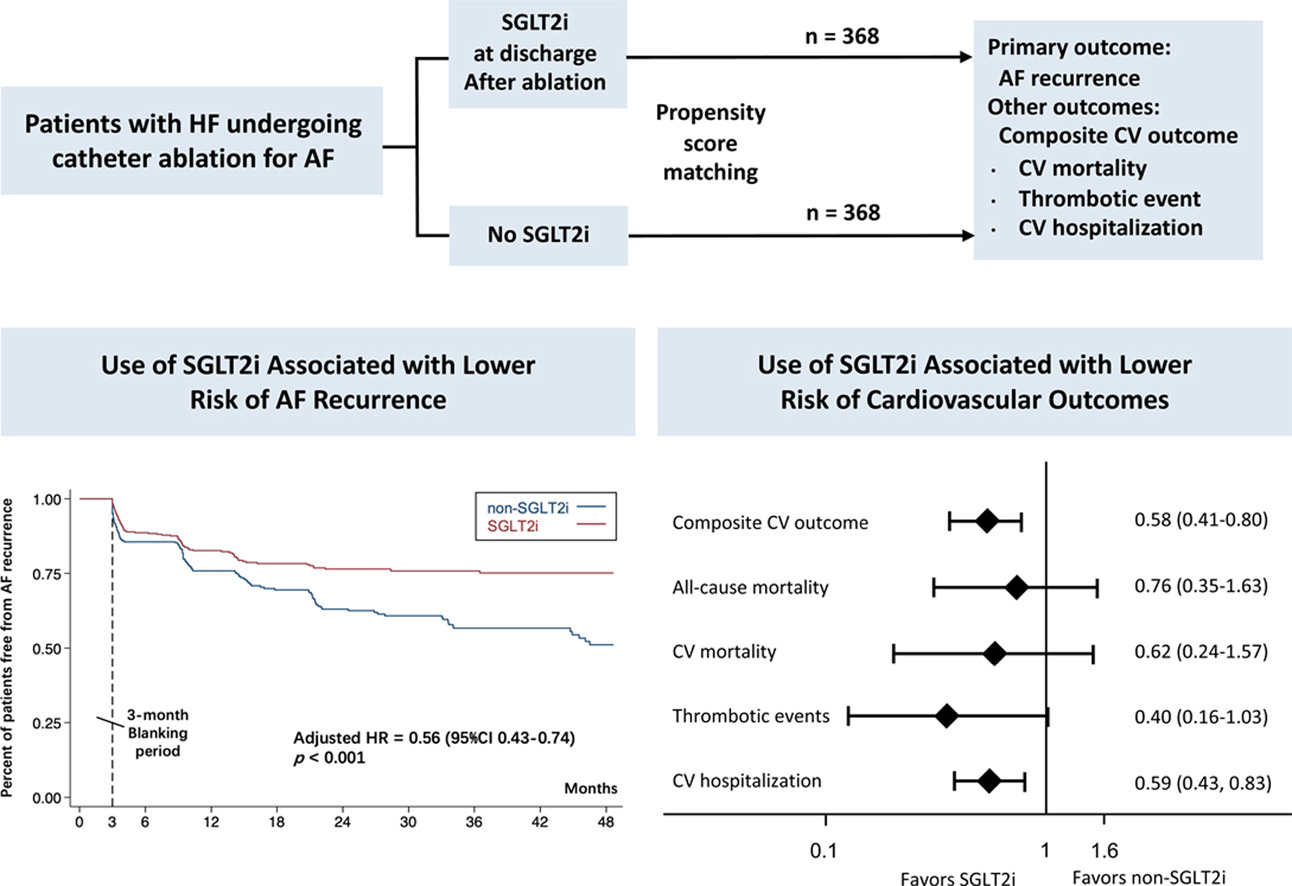
SGLT2i was associated with a lower risk of AF recurrence (adjusted HR = 0.56, 95% CI: 0.43-0.74, P<0.001). The composite risk of cardiovascular death, thrombotic events, or cardiovascular hospitalization was significantly lower in the SGLT2i group compared with those without SGLT2i (adjusted HR = 0.58, 95%CI: 0.41-0.80, p = 0.001). Although there was a trend toward benefits, the differences in all-cause mortality, cardiovascular death, or thrombotic events were insignificant between the 2 groups.
In European populations, SGLT2 inhibitors were significantly negatively associated with TC (OR 0.051, 95% CI 0.006–0.465, P = 0.0082) as well as PTC (OR 0.034, 95% CI 0.003–0.411, P = 0.0079), while no correlation was found with FTC. These findings remained consistent even after applying the Bonferroni correction.
Five RCTs reporting data for 11,211 patients were included in our study. The mean follow-up duration was 43.8 weeks. Our pooled analysis showed that SGLT2 inhibitors significantly reduced the risk of hospitalisations for heart failure (HHF) (RR = 0.76, 95% CI: 0.61–0.88, p = 0.001) in patients with MI. However, the risk of all-cause mortality (RR = 1.05, 95% CI: 0.78–1.41, p = 0.76), CV mortality (RR = 1.04, 95% CI = 0.84–1.29, p = 0.73) and all-cause hospitalisations (RR = 1.06, 95% CI: 0.96–1.17, p = 0.25) remained comparable across the two groups.
on a potentially negative note, I think one of the meds I’ve been taking out of jardiance/rapa/telmisartan/simvastatin/ezetimibe/acarbose may have been contributing to some noticeable muscle loss for me. I’m suspecting the jardiance? https://www.nature.com/articles/s41598-022-21486-9
I’ve read statins could potentially be at play as well. is this something to watch for?
Body by science, which is one strength training day a week. The program believes one set to failure can maximize growth.
I’ve been on it for the past 4 years though, no change. And there has been no change in diet. I’m getting older of course, about to be 46. I guess growth can slow with age?
One difference is I’ve been taking glycine on/off which should actually help with growth I believe
The loss has been IMO slow but accumulative. I wasn’t sure at first, but its gotten to the point where its a bit noticeable
If you’re worried about muscle loss and only strength training one day a week, most training literature would suggest that optimal strength training frequency would be at least 2-3 days per week.
That would be a decent place to start if you’re concerned about keeping a healthy amount of muscle as you get older.