Carnac the Magnificent…
The answer before the question is asked.
I see, government regulations ASAP…as people advertise/posting about private one to one blood component sharing.
It will not take long.
Carnac the Magnificent…
The answer before the question is asked.
I see, government regulations ASAP…as people advertise/posting about private one to one blood component sharing.
It will not take long.
Okay, okay! ![]() But, those are pretty specialized cases representing the few, not the masses.
But, those are pretty specialized cases representing the few, not the masses.
Some are are more niche, some broader… heart disease is the number one killer…
And while @A_User is right that there will be situations where biohackers may be able to duplicate the therapy much cheaper for a small group of biohackers and their families, it doesn’t scale to larger percentages of the population simply due to Intellectual Property laws…
Look at all the IP that Stanford University, Tony Wyss-Coray and Griffols have around Plasma, and TPE etc. They aren’t going to just take mass copying or use of these protocols, and knowledge without some compensation… we have an entire legal system set up to manage this type of thing, its not just going to go away.
So the biohacker approach may work for many of us here in this forum, it doesn’t address the 99.99% of the population that isn’t a biohacker, doesn’t want to be a biohacker, and doesn’t live in areas like the SF Bay Area or Boston or London (or academic centers where there are adventurous biology PHDs) where there is a critical mass of bioengineering expertise to be able to leverage this type of knowledge.
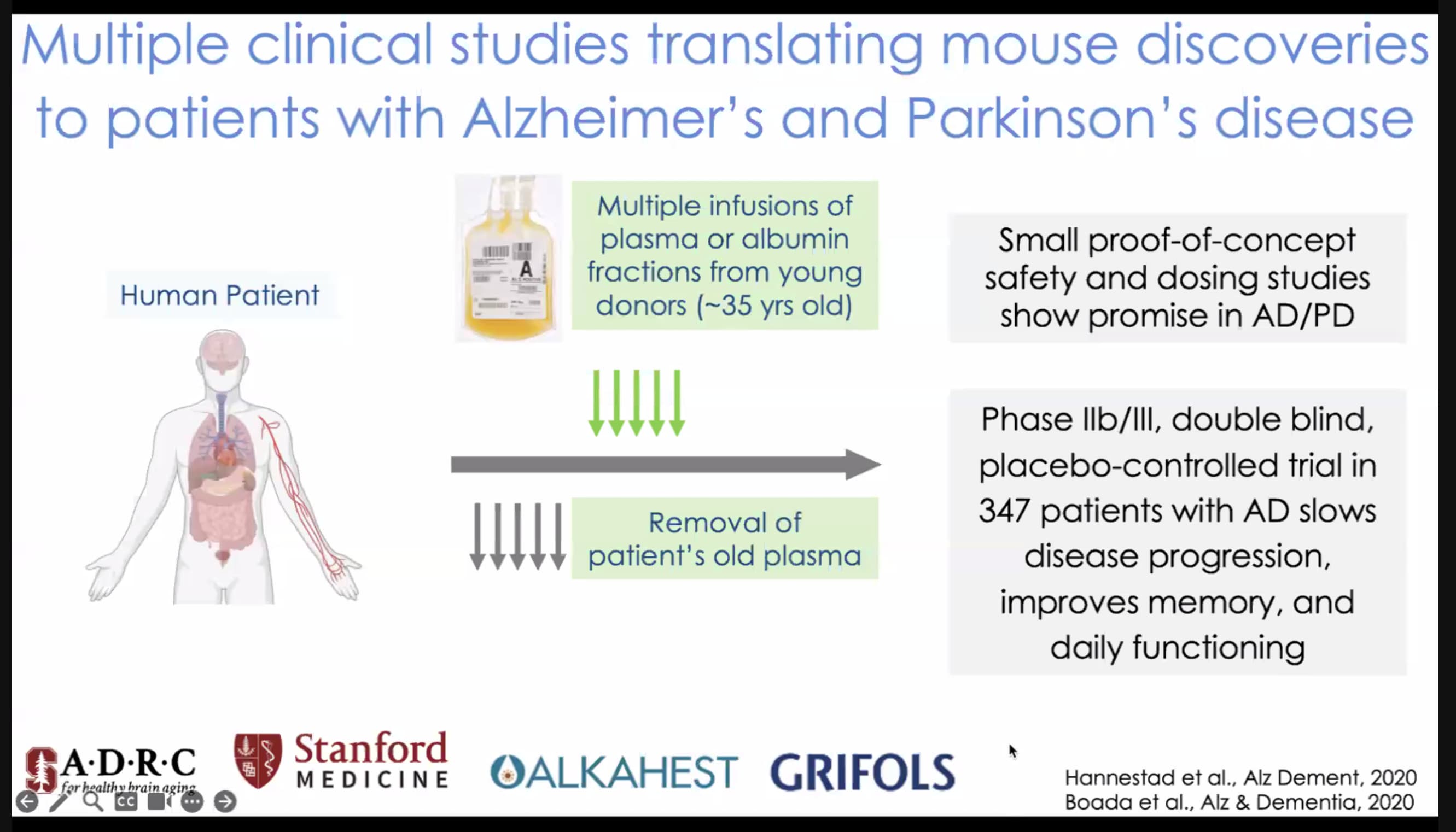
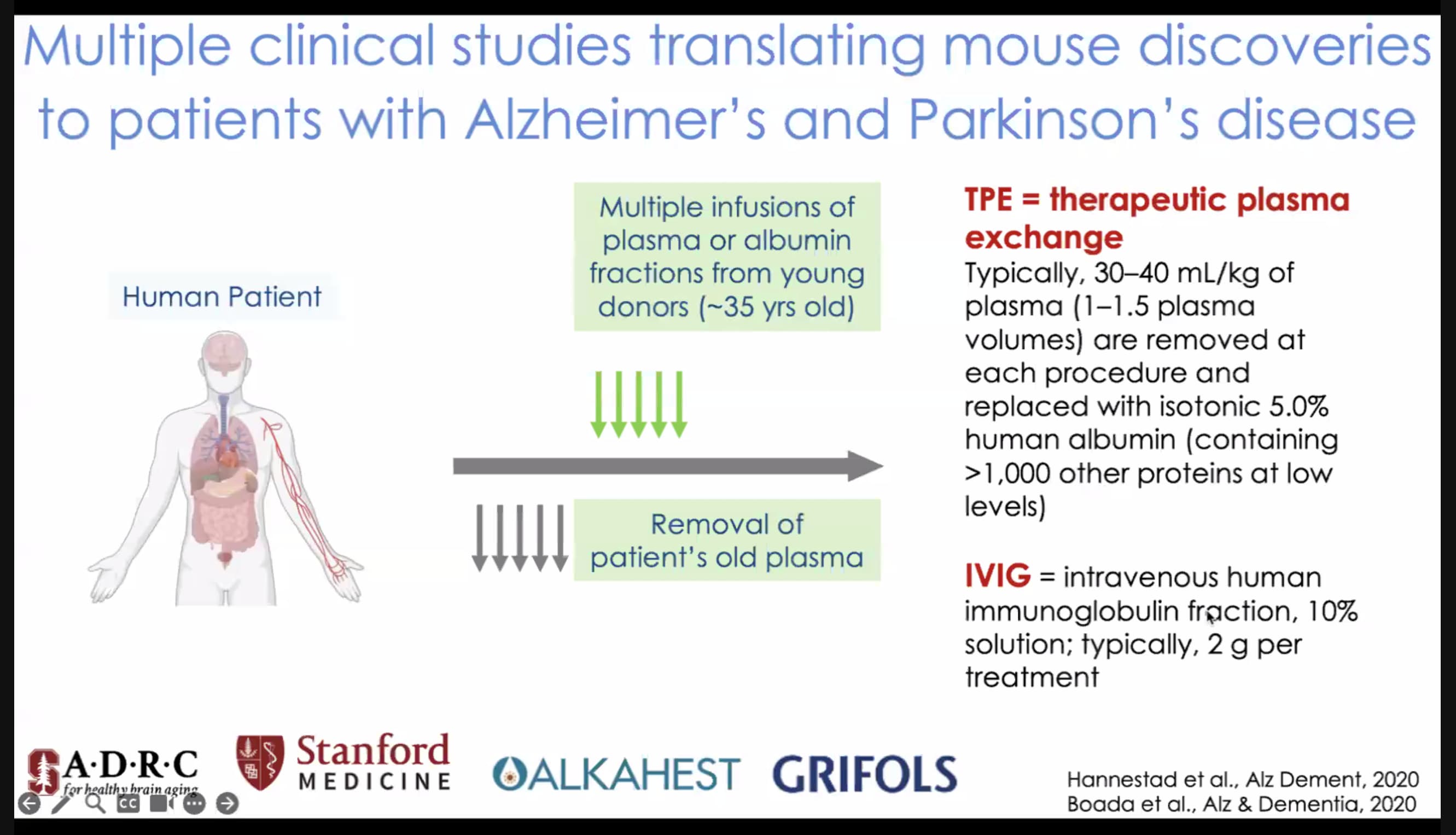
And… this is real today… here is a slide from Tony Wyss-Corray’s presentation today, good results from multiple therapeutic plasma exchange (plasmapheresis)… in recent clinical trials. If it improves things for peole with PD and Alz, there is a very high likelihood that its going to boost the performance of non-diseased people…
And TPE results in thousands of proteins transffered via Albumin… this is not something that is going to be made synthetically by biohackers any time soon.
Tony mentioned the potential to be doing TPE on a daily basis or every few days… to get maximum benefit. How many people will be willing to pay $150,000/month to do this?
And its not like prices have come down much for Plasma Exchange. Its been around for 20 years+, its widely used in many serious conditions, and its still priced in private clinics at $6,000 per session.
This is available to Bryan Johnson today… how long will it be before you have access to this at a price you can afford, do you think?
See full presentation here (scroll down): Harvard / Glenn Aging Conference, online, Monday. May 22 - #9 by RapAdmin
There will be people that will go to Countries{India, South America, Eastern Europe and many other] will hire a person 16 to 18 year of age, pay them a few hundred dollars a week to be their “stand by” on beck and call to “donate” blood component.
This is not any sophisticated equipment, plenty of dialysis equipment available on the secondary market for .10¢ to
15¢ on the dollar.
There are personal dialysis units the size of a business brief case.
Consumables component items not that expensive.
And the entire procedure is not that difficult.
OK - lets look at these in more depth…
The total available market (TAM) is different than the total addressable market … people can’t get clean water in most of Africa, so they are out as far as addressable market, as are many other areas.
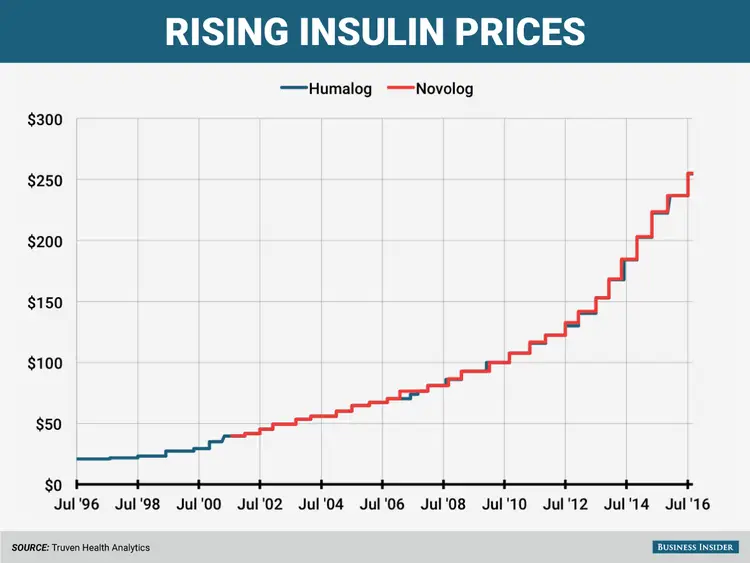
And realistically - aging doesn’t become a worry for most people until say… 40 or so. So - its really the developed world, over the age of 40. So perhaps 500 million to a billion people. This is about the same size as the diabetes market I suspect - and the price of insulin has continued to rise dramatically over the past 20 years, so simply having a large addressable market doesn’t seem to equate to lower or even decreasing costs:
It’s probably not going to be treated with surgery.
There are likely going to be all sorts of approaches - some are surgery, or other approaches like stem cell therapies, gene therapies, etc… all of which require biologicals manufacturing expertise at scale, and medical expertise to implement at the local level. I see no indication yet that these will come down in price very quickly, if at all. If Insulin, an unpatented “generic” is increasing in price at the level shown above, why would we expect these more Intellectual Property-heavy approaches to therapies to come down in price?
Every insurance company and socialized medicine system in the world will want and maybe even insist its people get this treatment.
In theory… but in practice not so much. In the US, people churn insurance companies so often that the Insurance companies don’t get any benefit from preventative approaches (so the insurance companies don’t invest in them). And in fact the trend is opposite to what you suggest:
Here: https://www.cnbc.com/2023/04/13/health-plans-could-soon-reduce-coverage-for-preventive-care.html
Here: Behind the push to strike down free preventative health care in America | On Point
And sadly, the rest of the developed world - Europe, Canada, Japan, etc. - while they have universal healthcare, they also seem to have the most conservative health care systems. How many years will it be before they cover rapamycin or therapeutic plasma exchange?
The reason drug companies seemly charge outrageous prices for some medicines is of course they sometimes spend billions to get a drug to market that only benefits a small percentage of the population and they must recoup their costs.
Heart disease generally doesn’t become a problem until you are older. Members of my family have had stents, valve repairs, and open heart bypass surgeries all paid for by their insurance. My own Medicare Plus plan would do this for me with relatively modest out-of-pocket expenses.
If drugs can be prescribed for the masses such as the Covid vaccines then the costs will be low for the individual. Early on I was worried that life-extending drugs such as rapamycin would be out of my reach. What I worry about now is that such drugs may become illegal. (Color me a conspiracy theorist ![]() )
)
Does it really matter if a billionaire can live 10 years longer and I can only live 5 years longer because he can afford more expensive treatments? Are you willing to deny everyone in the world 5 years of extra life in order to deny the billionaires of their 10? The argument that we should deny everyone longevity because some rich people will live longer is crazy. Should we stop developing medicines because not everyone can afford a gastrointestinal transplant?
There will be unaffordable longevity interventions and there will always be rich people. But there will also be affordable longevity interventions for the masses (Rapamycin?) You will never be the oldest or wealthiest person in the world. Enjoy what you have and what you can get. Some rich billionaire living to 250 is fine with me as long as I can live to 235. Your life will be of a higher quality than most of theirs anyways. ![]()
Chris,
You’re a finance guy, right?
Life extension therapies are a little like monthly compound interest. At some point, the more frequent and better therapies you get, the better your “total return” (or lifespan).
I’m thinking long term… what if a group of people can lock in a 15% to 35% annual compounded rate of return, while the vast majority of the people can only get 1% to 5%? Over 20 to 50 years what would happen to the relative wealth of those people, if the people getting the highest return already have the greatest amount of money?
So - I’m more concerned about the next 50 years, for society. …
In the Silicon Valley we are all about predicting the future, and trying to see where things are going, and what the opportunities and challenges will be. I can’t see this not becoming an issue. Bryan Johnson is just the start I suspect… of a major wave of activity. Just something we need to watch for I think.
Sure - but what if he lives to 500 or 700 years and you to 120? Is that still totally acceptable to you?
I’m thinking that Therapeutic Plasma Exchange (Plasmapheresis) / young plasma is increasingly looking like it may be the type of therapy where things start to diverge significantly for people who can afford $50K to 100K/month, and the rest of us.
If people did TPE twice or once every week for 3 hours, starting at age 40, I suspect aging might look very different from what we are used to. And if the benefits derived are a result of a complex assortment of thousands of proteins in Albumin (as Tony Wyss-Coray is suggesting), it may be many decades before any inexpensive synthetic version becomes available…
Its not clear to me how biohackers might be able to “hack” the young blood plasma market to get lower cost access to TPE. (other than nightly transfusions from their kids ![]() )
)

Personally, I don’t think TPE is the key to immortality. I think it will help, but I think Rapamycin is probably just as effective.
Technology is always available to the rich first, but then makes it’s way to the masses. That’s why everyone in the USA has a car, TV, computer, mobile phone, etc… These inventions were only available to the rich at one point. If a new life extension technology came about, I am sure there would be a mass-market alternative available within 10 years. There always has been.
Holding back technology and innovation until it is available to everyone just isn’t possible. For example, what about African countries where stores still don’t sell mobile phones? Should we ban mobile phones until everyone on Earth can afford one?
If someone lives to 700 while I live to 120, I probably wouldn’t know about it. ![]()
Would I be envious of a billionaire who could live to 700? Heck yes. Is it fair? No. What about the trust fund babies who never had to work a day in their lives and can live their dreams? Am I envious? Heck yes. Is it fair? No. Are 3rd world individuals living in squalor or those with horrible diseases envious of us who are healthy, well-off, and living in the first world? Heck yes. Is it fair? No.
I am thankful for what I have and try not to compare myself with others. I will accept whatever gifts and blessings may come my way with thankfulness. After all, no one in the history of mankind will have ever had those technological advances before me. That’s when I realize how much it sucked to be a caveman.
I completely agree with all of this, it is as usual very balanced and well thought out, but I also believe that if TPE can be proven to be effective it will most likely create it’s own industry. It’s true that the price of TPE varies massively all over the world, but I can envisage young people getting paid for plasma and centers being set up all over at volume. I think the market will largely create itself.
Its interesting… TPE has been around for decades and there is already an industry. And when I went in for my plasmapheresis therapies (purported), they said that the plasma has market has been really tight the past year or two (covid I suspect), with fewer people donating. So the market is already well established, and supply constrained. Of course things could change as markets evolve. I wonder what the critical path items are to supply improvement and cost reduction. The plasmapheresis equipment they use right now is large, bulky and expensive, but it takes a long time to get new equipment through FDA so that probably isn’t going to change much anytime soon.
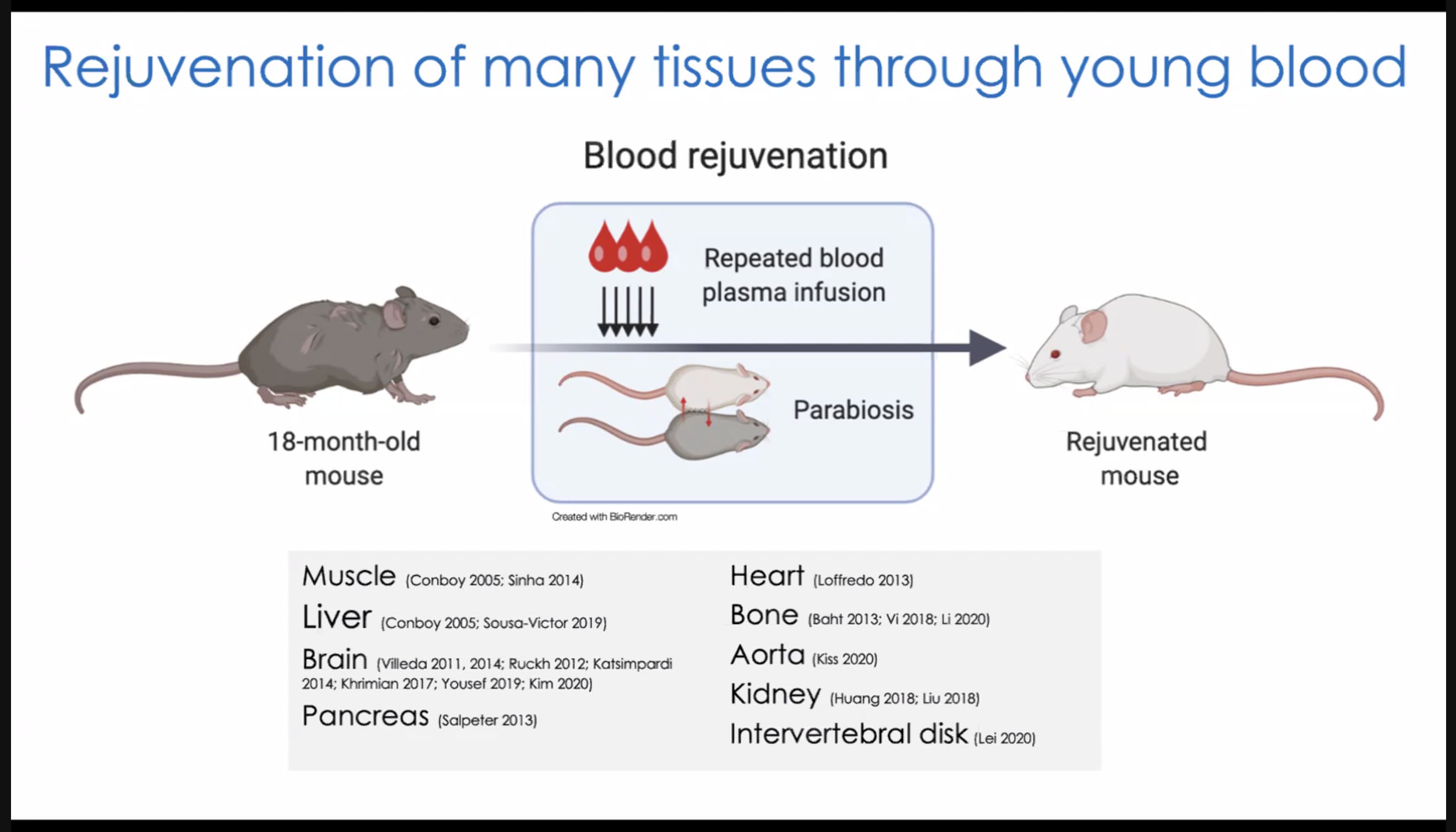
Getting blood donated from people is a pretty old “business”… so is there anything people can do to lower the cost by a significant factor and get greater participation by young healthy people in that market? And for the plasmapheresis for aging market, you want only blood from the youngest, and healthiest people. While Tony Wyss-Coray suggested the median age for blood plasma donors is considered a “young” 35 to 40, I suspect the optimal age for plasma donors in this application is likely much lower, in the 15 to 25 age range. But of course, that blood is even harder to get and even more expensive I suspect.
I feel that once the general public begin to understand that it could genuinely make them healthier for longer and that this is for ‘everyone’ the perception of plasma donation could shift, but maybe I’m just being an idealist. Byran’s TPE might point the way to how to begin to change the perception because it connects in a visceral way. Three generations of a family donating plasma to each other potentially reversing aging is very relatable. I think most people would donate their plasma to help their parents if they believed it would genuinely help stave off their decline.
As for lowering the cost of the equipment, again it’s probably just the fact that the market is small so there’s no real incentive to do so. It’s probably not a hard problem to solve. Admittedly, that may take some time and there are of course lots of regulatory hurdles to overcome.
I’m really curious to see how it plays out.
If they could figure out how to give blood transfusions to wounded soldiers on the battlefield over a hundred years ago, I think they can figure out TPE.
There are clearly different aspects. I think the core aspect of aging which release to Gene Expression is relatively easy to target. However, there are other changes such as DNA damage which are harder to target, but to some extent it might be possible to simply drop the damaged cells more readily than to fix them.
That does depend, of course, as to whether I am right about the core aspect of aging relating to Gene Expression.
FWIW
“They said that the plasma has market has been really tight the past year or two (covid I suspect), with fewer people donating“
Simple to raise the supply - just raise the price paid to those who donate.
In the UK we don’t get paid a penny to donate and aren’t short of blood, but there would be a flood of it if they started paying!!
If you take Rapamycin, you can’t donate blood.
Looking into this a little more… It does seem that the cost has potential to come down a lot in terms of the plasmapheresis services pricing. Cost of the equipment seems to be in the $30K to $50K range, they currently pay donors (on avg.) about $100 per liter of blood, disposables used in the process are about $1,500 to $3,000 per patient.
Of course overhead is also substantial, as it takes 3 hours or so to do a TPE session, so you have a very limited number of clients that you could cycle through the office in a 8 hour day (2.6 clients per day per machine) - so its hard to make a low price up with higher volume. What is likely needed is a 5 or 10 person plasmapheresis machine, or a low cost home machine. Probably easiest to do a 5 to 10 person machine for the existing companies, as they don’t have the skillset or cost basis for a lower cost home device.
Perhaps this is a service that every gym and healthspa will have in the future. The issue / cost / expertise issue seems to be the venous insertions / draws; you don’t want someone who can’t get the large needles / cannulas into your veins quickly and easily. I had one newbie nurse try twice on one of my visits for TPE and failed both times, before getting a more experienced person. If the nurses make a lot of mistakes, I suspect your arm quickly starts looking like that of a drug addict.
I suspect this type of plasmapheresis equipment is something Bryan Johnson will soon have at his home, with regular fresh plasma deliveries (like milk to the doorstep in the 1950s ![]() )
)
Plasmapheresis Cost:
The cost of Plasmapheresis is quite high. Per session of this method can cost anywhere between five thousand and ten thousand dollars in the United States. In some cases, this process may be required to be carried out repeatedly. It will help if you have a medical insurance to take care of the costs.
From: Plasmapheresis - Ask Hematologist | Understand Hematology
and:
Results
The direct cost of five IVIg infusion sessions totaling 2.0 grams per kilogram (g/kg) body weight was $10,329.85 compared to a series of five TPE procedures, which had direct costs of $4,638.16.
source: Cost-minimization analysis of the direct costs of TPE and IVIg in the treatment of Guillain-Barré syndrome | BMC Health Services Research | Full Text
Today, apheresis is available to patients in some physician practices. With equipment priced at $50,000 or more per machine, disposables costing between $1,500 and $3,000 per patient, plus the cost of adding highly trained professionals to oversee the procedures, apheresis is not something that every office practice can afford to or should offer. However, when office practices find it financially feasible to provide apheresis services and have the required office space and patient volume, it can be a good option for patients and a self-supporting business for the practice.
Source: Apheresis in the Office Setting - PMC
Full analysis here from a UK clinic here:
Convalescent-plasma-A-costing-review.pdf (509.6 KB)
The Apharesis equipment market seems to be about a $3 Billion market already:
Key Companies & Market Share Insights
The market is oligopolistic in nature and is marked by an extensive presence of mergers and acquisitions. New product developments, acquisitions, and strategic alliances are some major sustainability strategies adopted by industry players. For instance, in October 2020, Haemonetics received US FDA 510(k) approval for its NexSys PCS system with Persona technology. In January 2020, Fresenius Kabi spent EUR 30 million in order to build an apheresis and transfusion disposables plant in the Dominican Republic. Some of the prominent players in the apheresis equipment market include:
- B. Braun Melsungen AG
- Haemonetics Corporation
- Fresenius KabiAG
- Asahi Kasei Medical Co., Ltd.
- Terumo BCT, Inc.
- Mallinckrodt
- Nikkiso Europe GmbH
Source: Apheresis Equipment Market Size & Share Report, 2030