Obviously, that would be fantastic if it happened. But we have dozens upon dozens of examples that it doesn’t happen… search up the most expensive medical therapies / procedures / treatments and you can see many many situations where there are great new medical solutions, that only go to a small fraction of those who need them…
Why would longevity be any different? Perhaps since aging is universal you would have more people searching for work-arounds, but many medical procedures are just very complex and costly to do and there is no workaround.
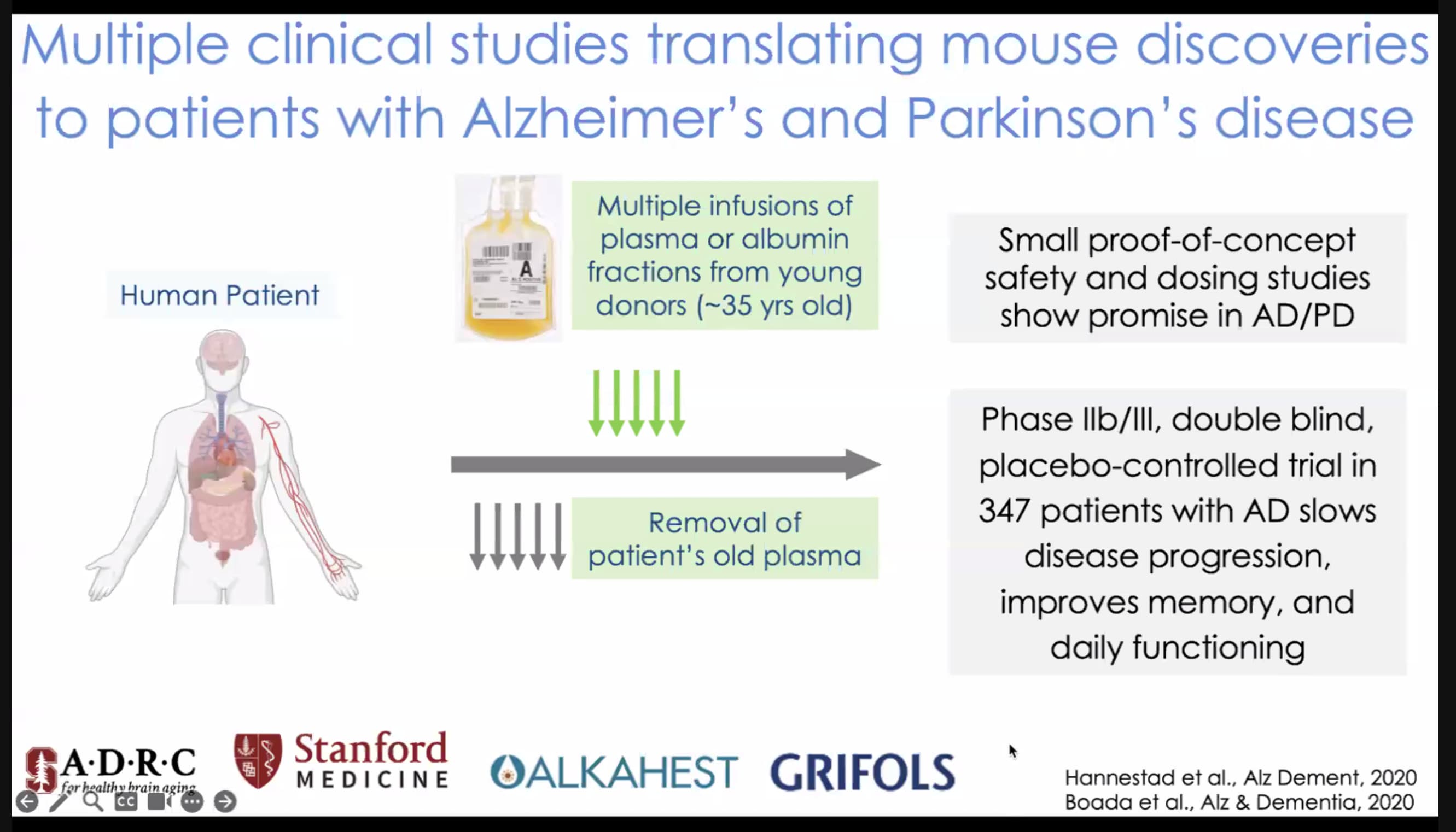
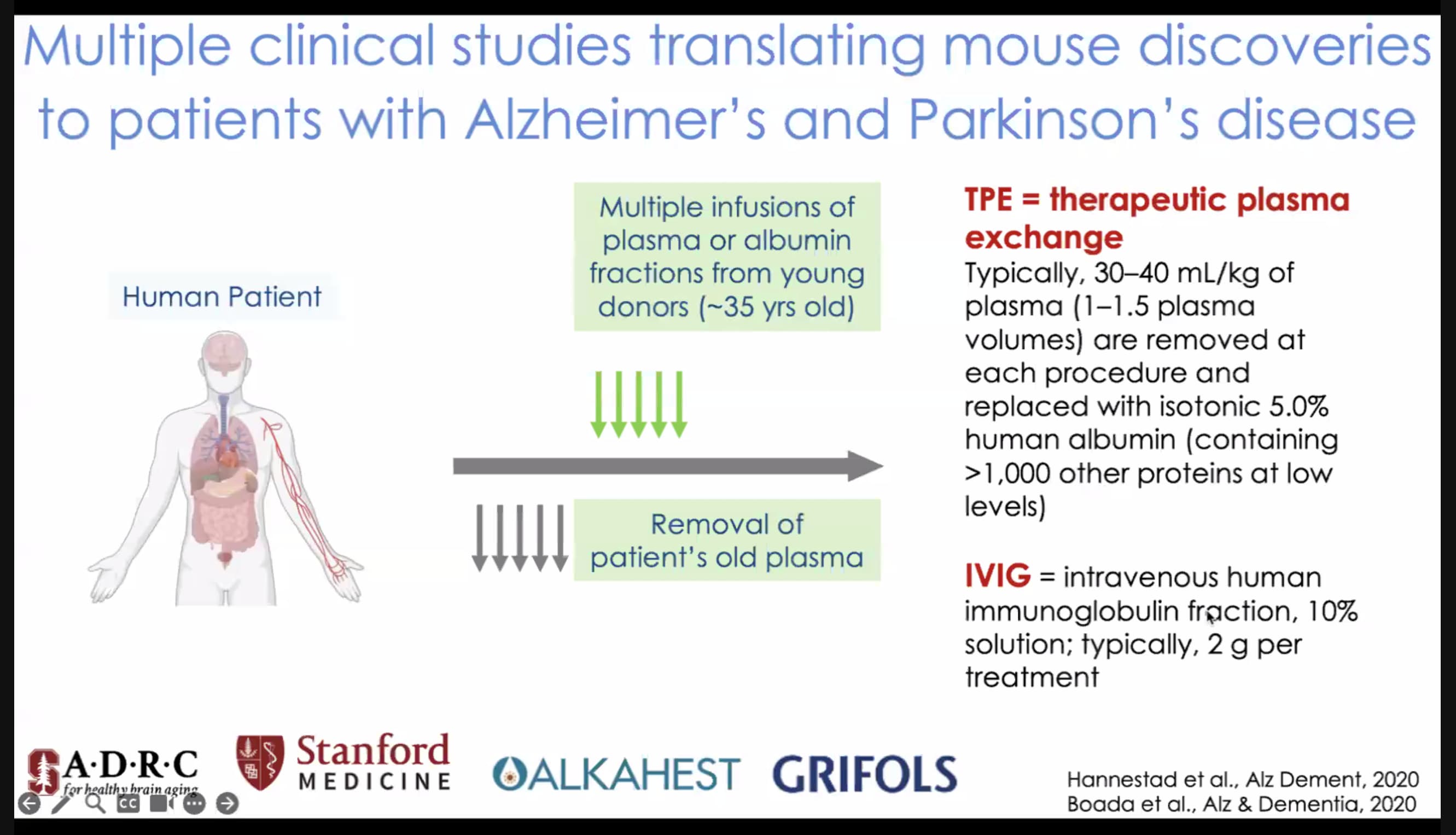
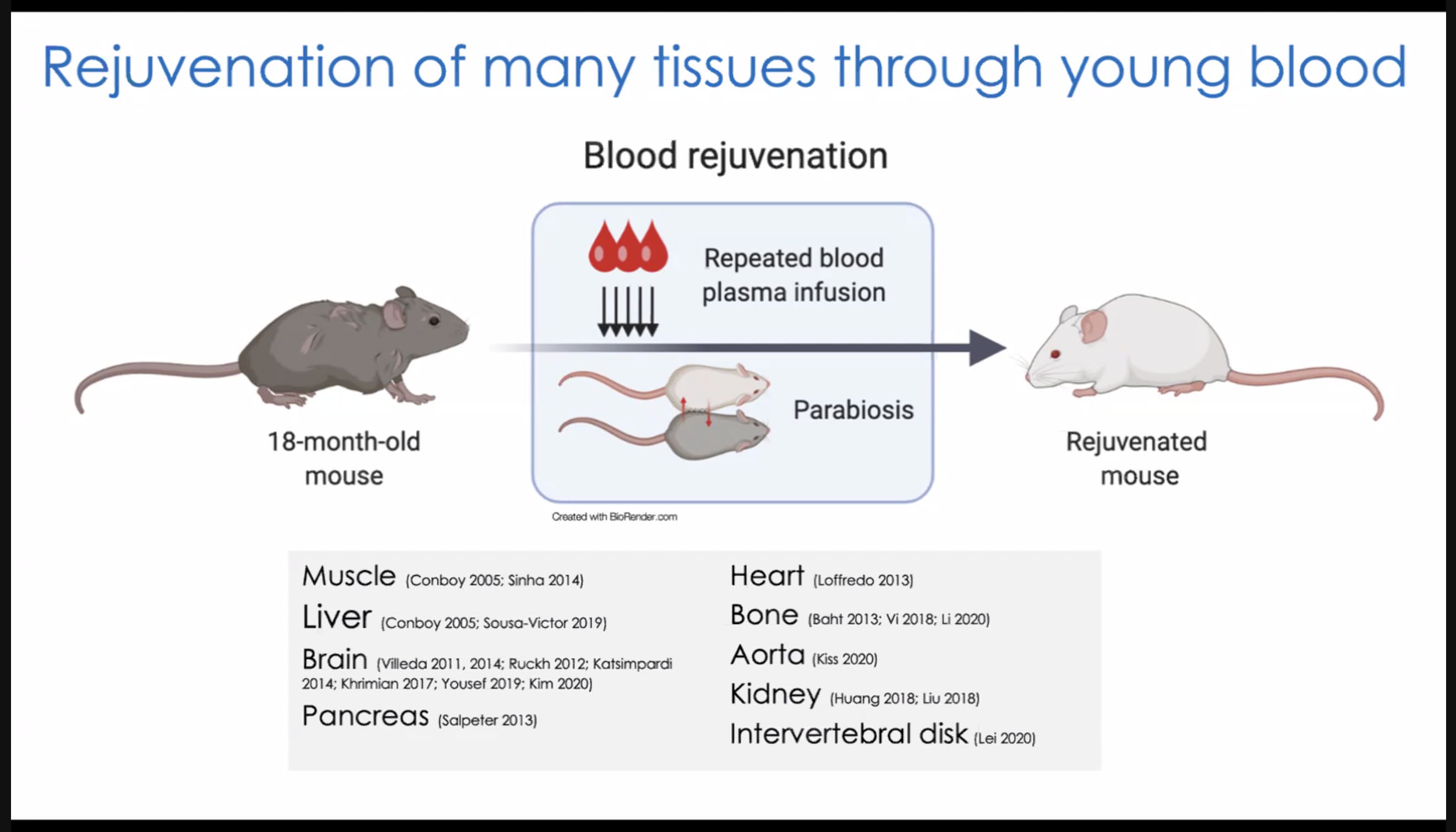
I’ll post the slides from Tony Wyss-Coray’s presentation at the Harvard Aging Symposium later - but he’s seen great results with Therapeutic Plasma Exchange and Young Blood… great improvements in all organ functioning including brain. Regular TPE is going to likely make a big difference in many aging people’s lives in the future… the optimal treatment regimen may be monthly or more frequent. At $6,000 per treatment (and the issue of being limited by the number of young blood boys you can get the blood from) suggests that it will be expensive for many years… I don’t see anyone at Longecity coming up with quick and dirty and cheap replacements any time soon…
More Examples below:
- Hemophilia B therapy costs $3.5 million per dose
- More gene therapies expected in 2023
A gene therapy considered to be the world’s most expensive drug raises questions about how to pay for it, and the federal agency overseeing Medicare and Medicaid could play a central role in ensuring patient access to potentially lifesaving medicines.
Full article: World’s Most Expensive Drug Revives Push for New Payment Models
Where are the biohacker efforts to provide low cost versions of these drugs?
The 10 Most Expensive Drugs in the US
Key takeaways:
- Zolgensma is the most expensive drug in America, with an average one-time cost of $2.1 million.
- Since September, six of the most expensive medications in the U.S. have seen a price increase.
The GoodRx Research team regularly tracks the most expensive medications filled at local pharmacies in the U.S., and drugs on that list have only gotten more expensive since we began tracking their prices. The list’s top 3 drugs — Zokinvy, Myalept, and Mavenclad — all cost over $60,000 for a typical monthly supply. However, these are the most expensive drugs filled at pharmacies, and patients self-administer them on a regular basis.
With more approvals of expensive infusions, cancer treatments, and gene therapies, we wanted to track the most expensive drugs, including those not available from a pharmacy. We call these drugs “healthcare provider-administered drugs,” because only a medical professional can administer them.
Many of the most expensive drugs are taken for an extended period of time, and costs quickly add up. This analysis ranks drugs by their annual cost for a typical course of therapy. Prices are based on the drug’s list price — which is the price that the pharmaceutical company assigns as an official price to a drug — then adjusted for the annual timeframe to create a comparable benchmark.
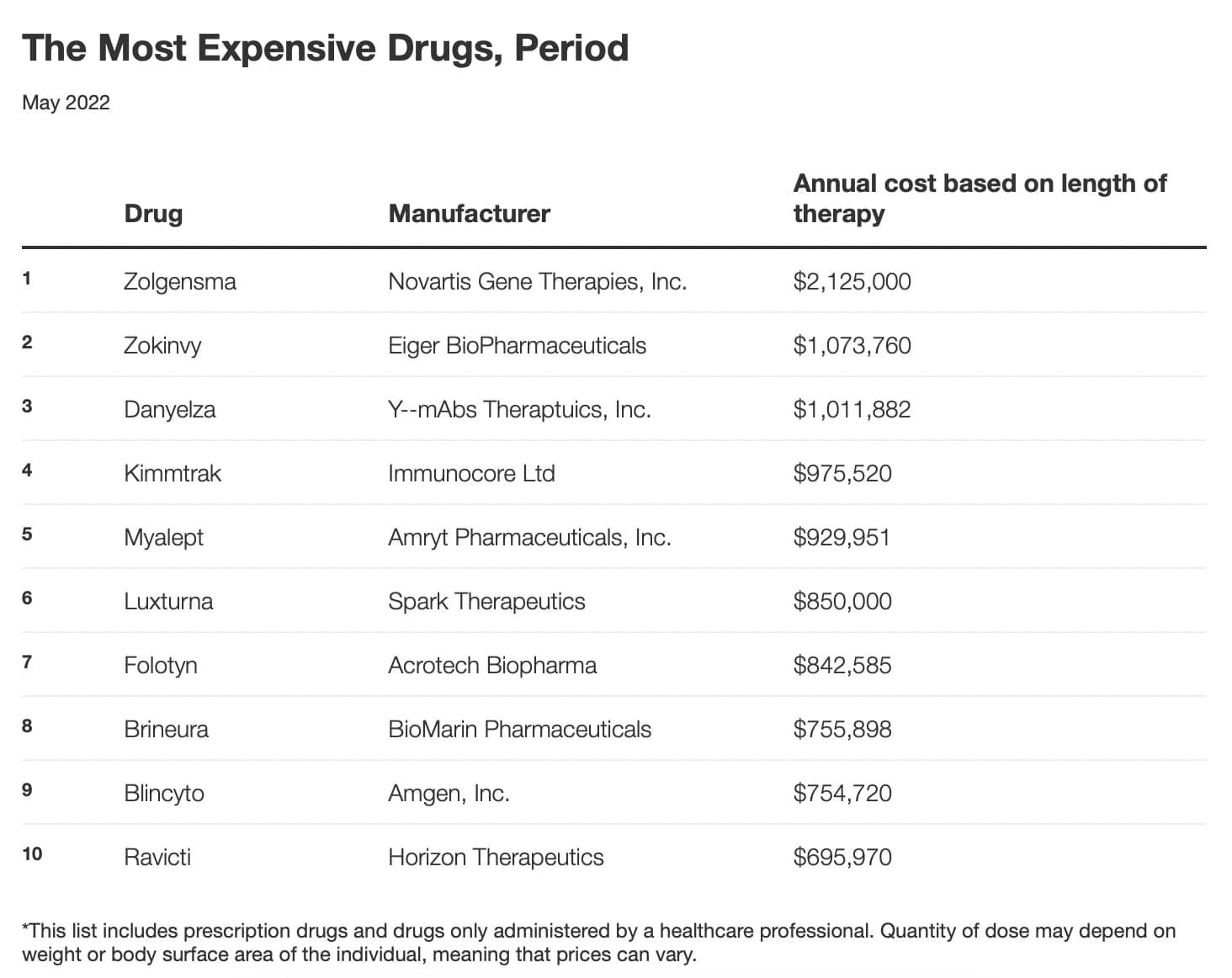
See full article: 10 Most Expensive Drugs in the US, Period - GoodRx
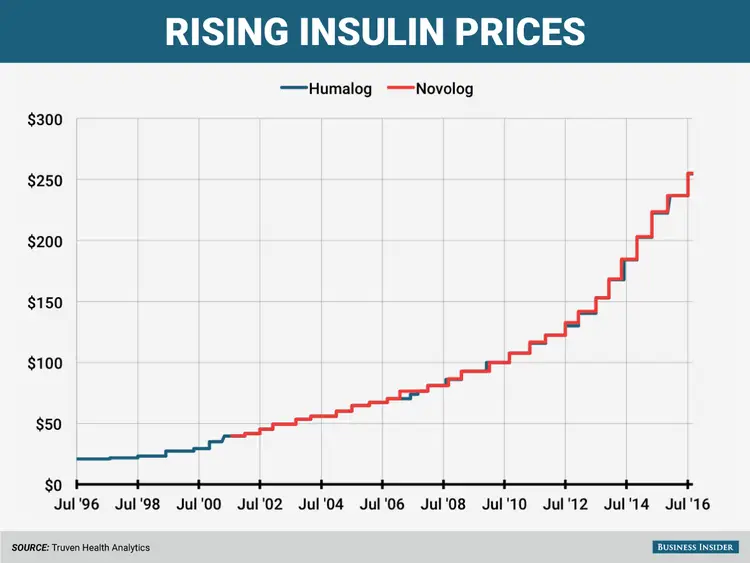
Why do you think these pricing trends of the past 30 or 40 years are going to change any time soon?
(from the Financial Times of London):
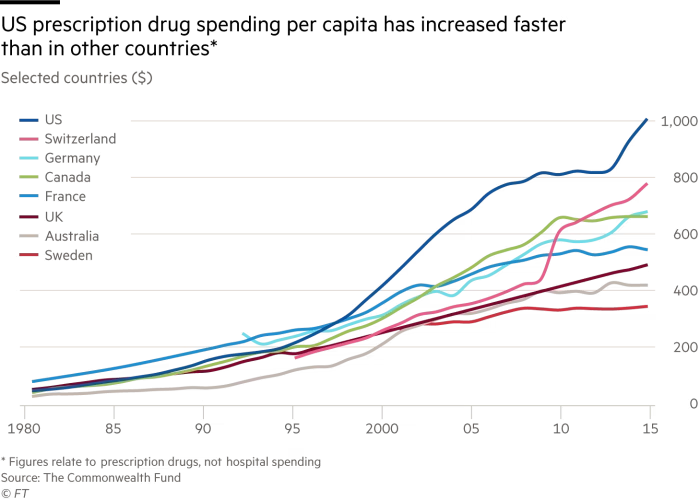
How quickly have the prices for these treatments come down in the past 10 or 20 years? How many people go without?
Top 10 Most Expensive Surgeries
Surgical interventions are the most expensive procedures. Their cost is estimated not only by the complexity of the procedure, the equipment used, etc. but also by preliminary training, postoperative rehabilitation, the work of maintenance personnel, etc. Some operations are so expensive that they can cause a small personal financial crisis, even with insurance. Only a large wallet (really big) and a bit of luck will save here. Today we are speaking about the top 10 most expensive surgeries in the world.
10 medical procedures that cost way too much
7. Open heart surgery ($324,000)
Sometimes the heart needs to undergo some operations since many factors affect its health. As they say, sometimes prevention is needed, and sometimes – repair. The range of open-heart surgery starts from installing a new artificial heart valve to working in the coronary artery to improve blood flow. The complexity and danger of the operation depend on the specific procedure. The costs depend on this, as well as on the time of preparation before and rehabilitation after surgery. And do not forget about constant monitoring by doctors.
5. Bone marrow transplant ($300,400 – $676,800)
Bone marrow transplantation is not a very complicated procedure. Depending on the donor, surgery may not even be necessary. Bone marrow can be obtained by transfusion of a patient, only intravenous access is needed. Large costs are obtained in research in the laboratory: the study of bone marrow to find a donor, its collection, testing. Another problem is the donor. If the procedure can be almost painless for the patient, then the donor will have to undergo a rather painful procedure (larger needles in the bone), moreover, this pain can remain for several weeks.
3. Heart transplant ($997,000)
A heart transplant is a surgery to remove a patient’s diseased heart and replace it with a healthy heart from a deceased donor. The danger, of course, is also very high. As in the case of the lungs, we need equipment that will temporarily replace the heart and pump blood through the body. Long preparation, rehabilitation, medications – all this makes the operation very expensive.
2. Transplantation of the “Heart-lungs” complex ($1,148,400)
A heart/lung transplant separately is a very risky operation, and a complex transplant doubles the danger. The main expenses (except for donor organs) are hospital expenses, diagnostics, and laboratory tests. After the operation, an active and complex rehabilitation will be required.
There are many articles describing many patients who changed as individuals after a heart transplant, becoming more like those who owned a new heart than themselves. Some people believe in a soul that lives in your heart, others consider it fiction.
1. Gastrointestinal transplant ($1,206,000)
The gastrointestinal tract is the longest organ in man. The complexity of the operation is that it takes a very long time until section by section is removed. Most often, one can get onto the operating table due to intestinal cancer, a serious injury or a defect, and sometimes due to a particularly vicious infection.
The operation can take a whole day and requires long and serious care after it.
When transplanting the intestinal tract, there may be a need for a liver transplant, as it also suffers greatly due to local problems. The largest expenses (up to $800,000) can go to hospital expenses: research, preparation and postoperative care.
Source: Top 10 Most Expensive Surgeries | High Point Surgery Center Review