Sure, but there is no proof of safety for berberine like there exists for pharmaceuticals. Nor proof of efficacy for outcomes.
I and others have observed that we know much more about metformin that we know about berberine. The LLM summary I posted yesterday reiterated that point and I don’t know anyone who would disagree with it, including those of us who choose to take berberine as I did for several years.
With all of this said, I do not see the relevance of your comment when my comment was focused entirely on the relationship between berberine and prolonged QTc intervals.
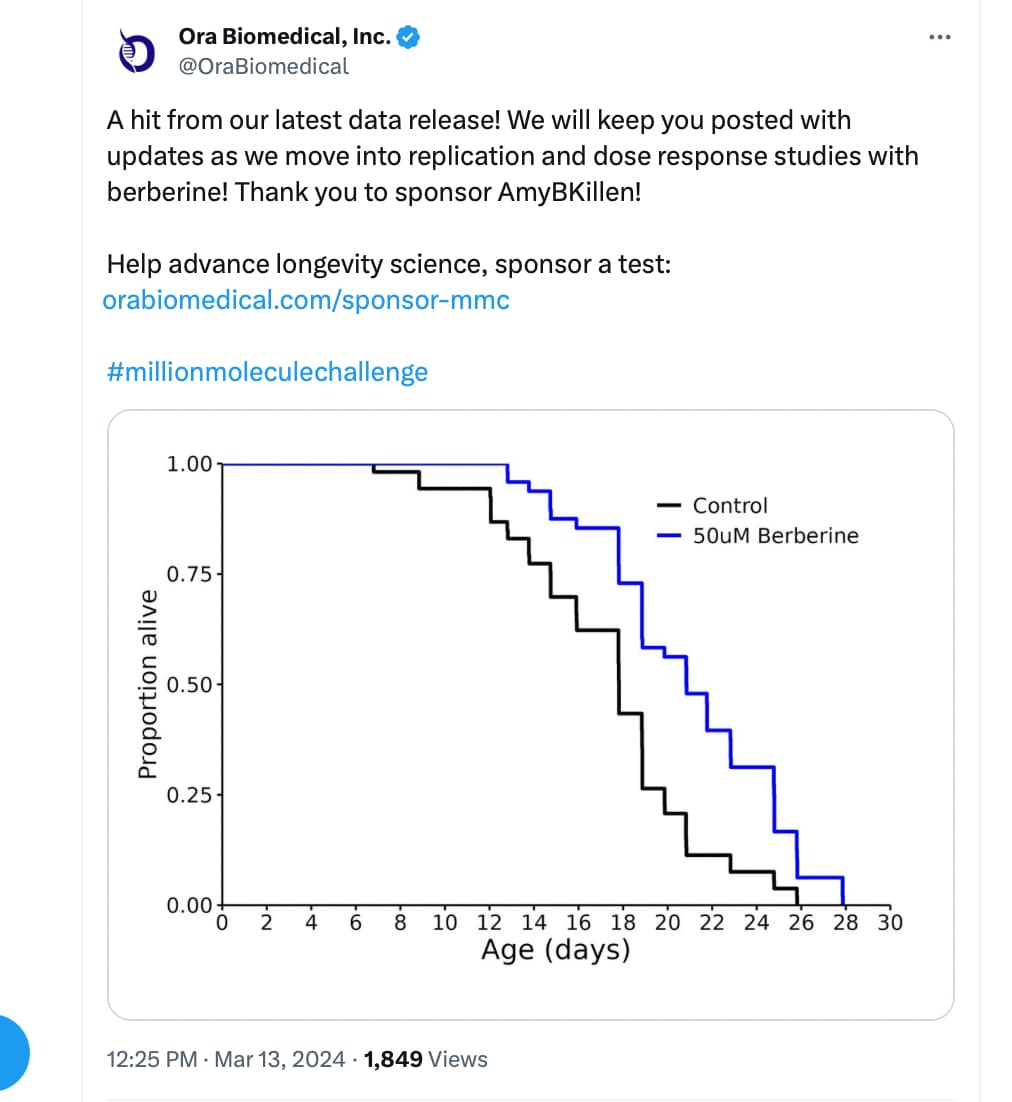
Some good news from nematodes (tiny worms). Thanks @AmyK !
Source: https://x.com/OraBiomedical/status/1767995488333427038?s=20
6 Likes
Ha! Yay! I actually asked them to run berberine + sildenafil but they made a mistake and just ran berberine. But… statistically significant (3 day!) extension of lifespan! I’m eager to see if adding a pde5i helps or hurts. Go worms!
6 Likes
It seems likely to me that pulsing interventions (e.g. berberine, metformin) which boost akkermansia levels would maintain a benefit beyond the dosing period. But i don’t know how long akkermansia levels would take to return to baseline.
Does anyone know of any berberine - akkermansia gut levels as end point studies. In particular studies which have a post intervention follow up to see if higher akkermansia levels are maintained post intervention.
3 Likes
I could only find two studies that even mentioned berberine+akkermansia and they were not in humans.
“BBR increased beneficial bacteria, such as Akkermansia and Bacteroides, and BRB increased beneficial bacteria, such as Ileibacterium and Mucispirillum.”
“At the genus level, BBR and BRB treatment decreased Lactobacillus and Romboutsia, while BBR increased beneficial bacteria, such as Akkermansia and Bacteroides, and BRB increased beneficial bacteria, such as Ileibacterium and Mucispirillum”
4 Likes
In the end with Berberine and many other molecules you need to either take it or not take it. In looking at it some time ago I did not identify any reasons substantial enough to not take it. Today, however, I watched part of this video which gives some reasons for taking it.
I like it because it is one of many HDAC inhibitors that I take.

3 Likes
There is no proof of safety? No one is checking if people are dying from it, it can be undetectable if the mortality takes long enough.
Absence of evidence is not evidence of absence. You want a large clinical trial to show it’s safe, along with copious mice studies.
1 Like
As I said I did not identify any reasons not to take it. I did a search on Berberine and toxicity. I may have kept some records of what I found, but I have just done another quick search.
Berberine has very low toxicity in usual doses and reveals clinical benefits without major side effects. Only mild gastrointestinal reactions may occur in some patients.
In animal studies, and I mean side effects, not acute toxicity. If you gave 5,000 people berberine it would show what the effects on all-cause mortality, etc, would be.
Oh come on. It’s in food. Can you do that for all of your food too? Even then it would be meaningless for an individual. We’re all different.
They tested the Vax and we have Maddie De Garay still having trouble, while some bizarre hypervaccinator from Magdeberg Germany gets 217 jabs over 29 months and doesn’t even notice anything.
I like testing, I believe science increases our understanding and I work really hard to understand. I think it could be done with less expense and roughly equal results.
2 Likes
I disagree, I think cycling interventions is also an option. Take akkermansia municipalis as example objective. Rhubarb, berberine, pomegranate extract will all have a beneficial impact. So there may be no need to apply antone intervention chronically. And side effects should be lower if individual interventions are cycled for short periods.
2 Likes
Berberine isn’t food, it is a supplement of an extract with zero difference from other active drugs. Whether it is in some berries not many eats(I have found no evidence of this), it is still way of a different concentration. It is like screaming lovastatin is safe because it is in oyster mushrooms. That’s not how anything works.
Food has already been studied in large observational trials and clinical trials and we know what can decrease events & all-cause mortality and have other benefits
There is zero large trials on berberine that aren’t a summation of small trials i.e like mortgage backed securities. If you trust berberine might as well put all your money in a MBS. ![]()

A large trial does measure individual responses too. You can catch side effects that happens 1/5000, if for example so many took berberine in a clinical trial.
But I already can tell I am not going to convince you as you seem like an ‘appeal to nature’-fallacy kind of person, but at least it is for the record.
The timing (including cycling as an option) and quantity are variations on taking it.
2 Likes
I have not looked at the reviews on Berberine to calculate the number of people who have tried it and the size of the trials, but for this statement I assume you have.
How many people have taken it in each trial and why was that not enough?
Supplement companies tend to not be able to afford large trial, it would be surprising if there ever was one, and yes it is correct there has never been a large trial.
Reviews on berberine are the MBS of health / science .
It is not enough because you want a large sample size to detect rare events, and outcomes in general. They just look at surrogate endpoints, typically, it is terrible in comparison with other drugs. If you combine a bunch of junk studies in a review, it will just output junk. Just look at the meta analytic reviews for ivermectin and covid and other junk (which failed in multiple large RCT’s): Ivermectin for COVID-19: real-time meta analysis of 101 studies (ivmmeta)
Berberine is an over the counter drug in China and with a long history of use in traditional Chinese medicine. Most of the research has been done there but published broadly.
Just to be clear, is the following study of the quality you say is generally lacking in the research literature? Seems to conflict with your statement that no large studies have been done. But I welcome clarification.
Berberine versus placebo for the prevention of recurrence of colorectal adenoma: a multicentre, double-blinded, randomised controlled study. Chen, Ying-Xuan et al. The Lancet Gastroenterology & Hepatology, Volume 5, Issue 3, 267 - 275. (Jan 8, 2020)
I can’t get the full-text easily but the research design from the abstract below
Abstract : Background
Chemoprevention of colorectal adenoma and colorectal cancer remains an important public health goal. The present study aimed to investigate the clinical potential and safety of berberine for prevention of colorectal adenoma recurrence.
Methods
This double-blind, randomised, placebo-controlled trial was done in seven hospital centres across six provinces in China. Individuals aged 18–75 years who had at least one but no more than six histologically confirmed colorectal adenomas that had undergone complete polypectomy within the 6 months before recruitment were recruited and randomly assigned (1:1) to receive berberine (0·3 g twice daily) or placebo tablets via block randomisation (block size of six). Participants were to undergo a first follow-up colonoscopy 1 year after enrolment, and if no colorectal adenomas were detected, a second follow-up colonoscopy at 2 years was planned. The study continued until the last enrolled participant reached the 2-year follow-up point. All participants, investigators, endoscopists, and pathologists were blinded to treatment assignment. The primary efficacy endpoint was the recurrence of adenomas at any follow-up colonoscopy. Analysis was based on modified intention-to-treat, with the full analysis set including all randomised participants who received at least one dose of study medication and who had available efficacy data. The study is registered with ClinicalTrials.gov, number NCT02226185; the trial has ended and this report represents the final analysis.
Findings
Between Nov 14, 2014, and Dec 30, 2016, 553 participants were randomly assigned to the berberine group and 555 to the placebo group. The full analysis set consisted of 429 participants in the berberine group and 462 in the placebo group. 155 (36%) participants in the berberine group and 216 (47%) in the placebo group were found to have recurrent adenoma during follow-up (unadjusted relative risk ratio for recurrence 0·77, 95% CI 0·66–0·91; p=0·001). No colorectal cancers were detected during follow-up. The most common adverse event was constipation (six [1%] of 446 patients in the berberine group vs one [<0·5%] of 478 in the placebo group). No serious adverse events were reported.
Interpretation
Berberine 0·3 g twice daily was safe and effective in reducing the risk of recurrence of colorectal adenoma and could be an option for chemoprevention after polypectomy.
2 Likes
Be real, no one is going to pay for large clinical trials for supplements that can’t be patented and are sold by a myriad of companies.
The FDA regularly issues warnings on food supplements. Many supplements have been used for decades with no alarms being sounded. For most common supplements I think the risk is very low.
3 Likes
“extended the lifespan of chemotherapy-treated mice and naturally aged mice by ~52% and ~16.49%, respectively. The residual lifespan of the naturally aged mice was extended by 80%, from 85.5 days to 154 days. The oral administration of BBR in mice resulted in significantly improved health span, fur density, and behavioral activity. Therefore, BBR may be an ideal candidate for the development of an anti-aging medicine.”
2 Likes
NIH does have funds for conducting the kind of research we are talking about and they have a special reporting arm for substances such as berberine. I have not tracked down the funding but they may have been involved in some of the research we have seen. Depending on the administration in charge, the federal government can have an incentive to investigate such interventions because they create competition to prescription drugs and in doing so can exert downward pressure on prices.
Meanwhile, there is no silver bullet here. In specific circumstances, there are good reasons to take berberine and good reasons not to take it. Arguments on which side is better might not make sense based on what we know and don’t know.
1 Like