There are no biomarkers in an otherwise healthy individual to be lowered that is as powerful as apoB to prevent health decline and increase longevity. I think I have summarized the most important of the current information in this thread, if I missed anything you can post it here.
ApoB is the Rate-Limiting Step in prevention of cardiovascular disease, which is the primary cause of death in the U.S. and across the world. The leading cause of death today, with 17.9 million deaths yearly, 1 in 5 people die from it (1). Although a multi-factorial process, it can be controlled and prevented by this single factor.
There are untold amounts of people who survive their heart attack or stroke but are maimed for life with diminished quality of life. As such, even though reducing apoB improves lifespan, preventing heart attacks and strokes are worthy in of itself especially if the prevention strategy has a proven net benefit by reducing all-cause mortality.
The importance of apoB comes from the way it affects the disease process unlike any other factor, it is the bottleneck factor, which is limited enough, halts the progress of the disease. So although the disease is multifactorial, if you stack the cards in the direction of lowering apoB, the other factors don’t matter as much if you did it early enough.
It’s Rate-Limiting Because of Genetic Studies
We know that people who genetically, are born with lower apoB levels have much lower amounts of heart disease. Because these genes are randomly assigned at birth, as people don’t choose a partner based on genetic apoB levels, these studies have in a sense been subject to randomization which is important to find cause and effect.
ApoB is the more accurate measurement taking the place of LDL as the new rate-limiting factor. They can mostly be used interchangeably but apoB is measuring the actual factor while LDL is simply a marker (2).
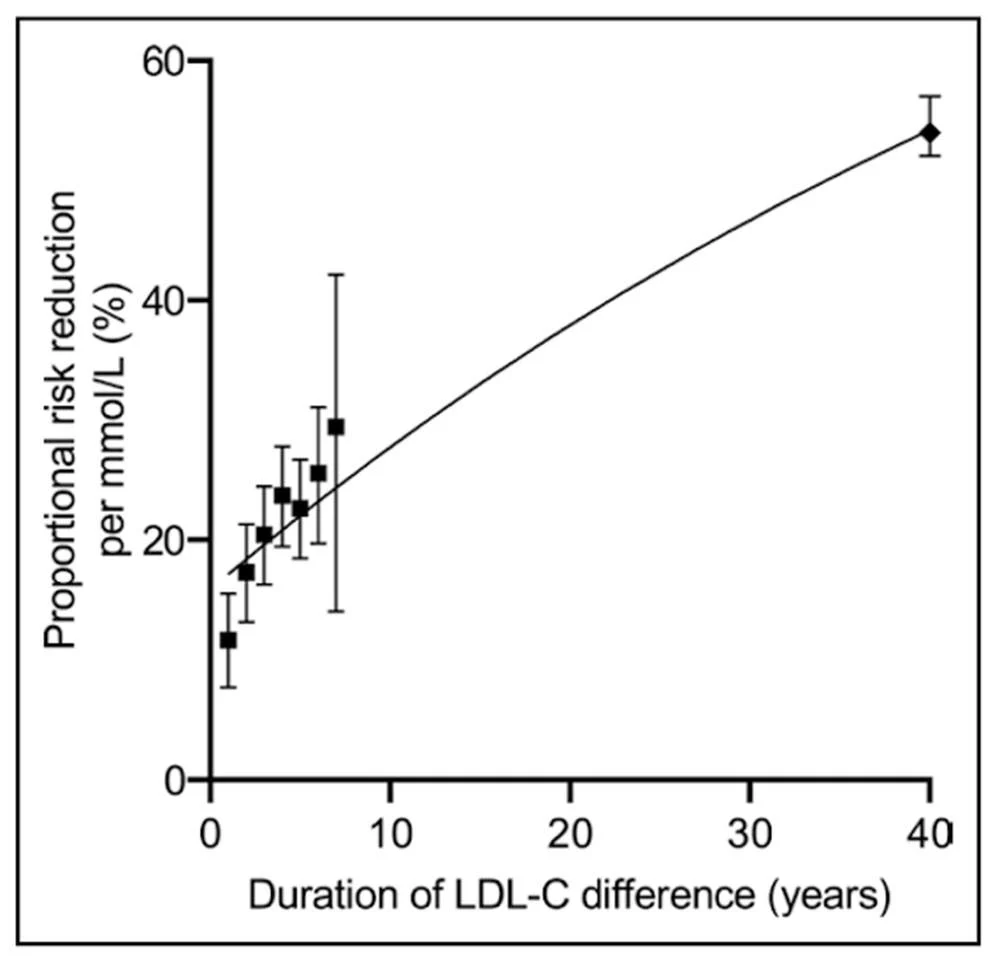
If you place the genetic reduction on a curve, you will see that even a small lifelong 38 mg/dl reduction in LDL reduces cardiovascular events by over 50% (3). In the graph you can see this point at 40 years out.
The points at the beginning of the graph are studies of drugs lowering apoB in clinical trials, they are of shorter duration so the magnitude of the effect is smaller. The clinical trials are also randomized, so able to find cause and effect in a similar way as the genetic studies.
The genetic studies show us the power of it and why they can be a botteneck on the process of developing cardiovascular disease and causing its events. Since the function of these genes are carefully analyzed, we can know if these genes can only lower apoB. That means that despite of the other factors presence, simply lowering LDL if early is enough is good on its own if it’s early enough. Since most of us have atherosclerotic plaque, which is something that is found in even young people, lowering apoB shouldn’t be considered the only strategy. But if you were lucky to be born with a mutation in the PCSK9 gene leading to loss of function of that gene, which led to the development of the PCSK9 inhibitors, you would be pretty much protected from the disease.
Elevated apoB is a really bad time
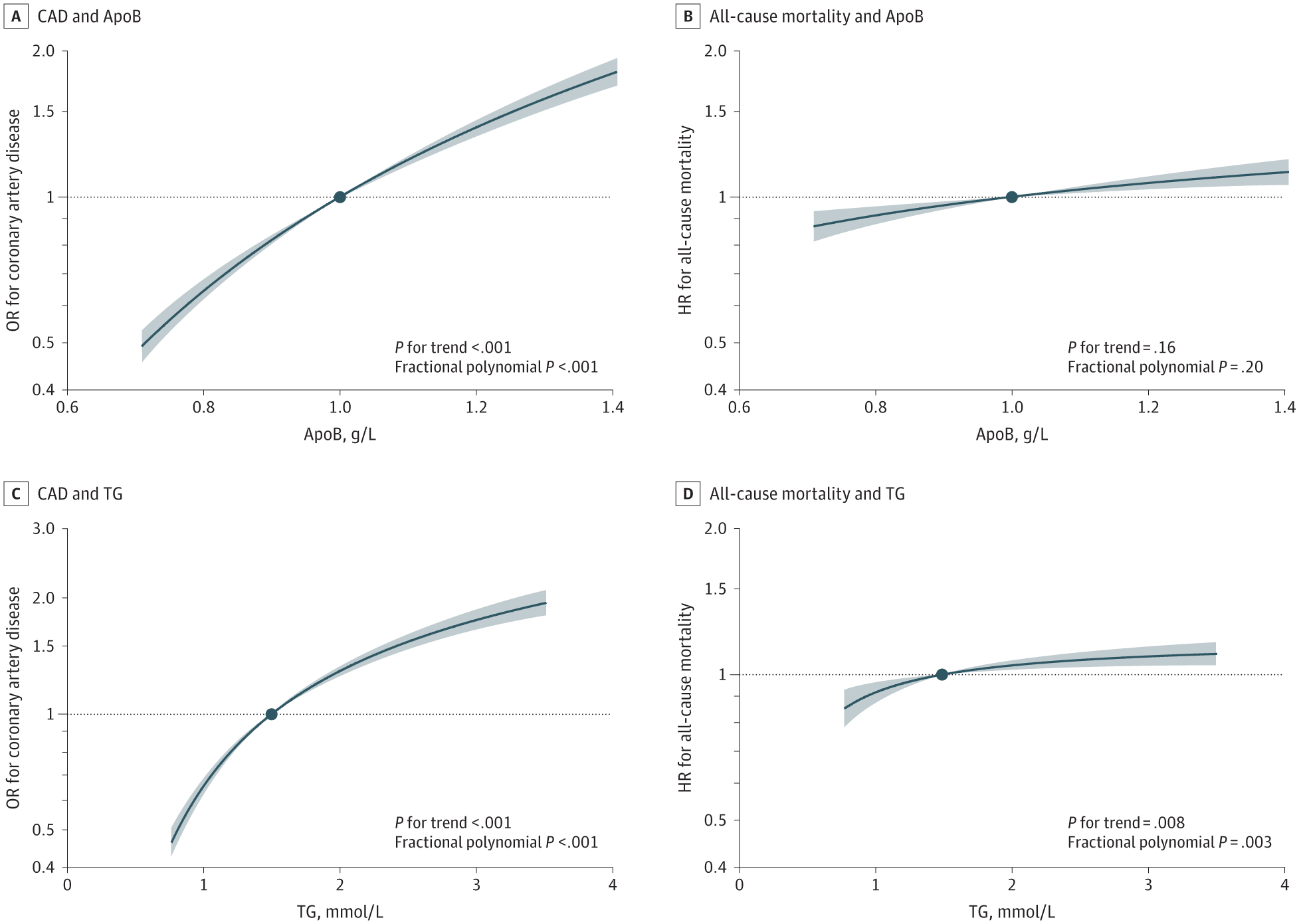
On the opposite side of the coin, since you can prevent the disease so greatly simply by turning the knob on this parameter if early enough, you can also accelerate the process if elevated. If your apoB is increased by 24 mg/dl from the average at 100 mg/dl, you have 60% lower chance of living to 90th percentile lifespan (4). We can see in a similar way events increasing from every amount above 70 mg/dl, where every increase of 24 mg/dl doubles the risk of cardiovascular events (5). The same study shows us also the true relationship between apoB and CAD without any residual confounding in the graph below. This study was not significant for apoB and all-cause mortality, but it was for LDL, most likely because it had a greater ability to detect it. Usually studies have more information on LDL which increases its ability to detect effects on total mortality that overall is affected by so many other things which reduces the explanatory power of apoB. There is the usual saying that even if you prevented everyone from getting cancer, or heart disease, they would only live a few years longer.
If you are expected to live long you need a low apoB
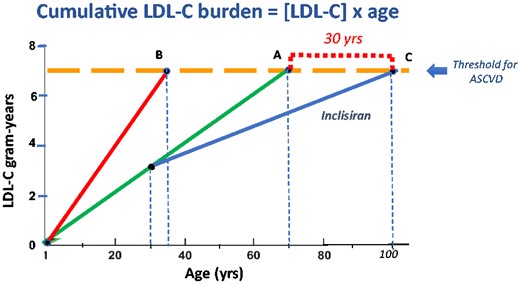
Cardiovascular disease is not an age-related disease, it is a time-related disease. Although the average person wouldn’t live that much longer if they prevented heart disease. Eventually the exposure you have of total atherogenic lipoproteins will catch up with you. From being the potential botteneck on the progression of your cardiovascular disease if lowered enough, it became the bottleneck on your longevity. We know this because this disease develops in youth as well, and in fact, as shown in the genetic studies, is very much dependent on time and your total exposure to apoB. That the youth aren’t spared from progressing with this disease, means you won’t be spared even if your body was returned to a youthful state. Even if you increased your time you could have, your age, the disease would still progress based on the amount of atherogenic particles and your age, eventually reaching the threshold for ASCVD (6).
How to lower apoB
You can discuss that here, what you are doing to lower it, what your apoB is, and discuss about apoB in general. If you find any new studies about apoB feel free to post it here. Genetic or mendelian randomization studies are especially valuable and clinical trials.
(1) Cardiovascular diseases - WHO, 2024.
(2) Apolipoprotein B vs Low-Density Lipoprotein Cholesterol and Non–High-Density Lipoprotein Cholesterol as the Primary Measure of Apolipoprotein B Lipoprotein-Related Risk: The Debate Is Over | Acute Coronary Syndromes | JAMA Cardiology | JAMA Network - Sniderman, 2022.
(3) Cumulative effects of LDL-C reduction in mitigating cardiovascular risk - Peter Attia - Attia, 2022.
(4) https://www.sciencedirect.com/science/article/pii/S2666756821000866 - Richardson et al., 2021.
(5) Dose-Response Associations of Lipids With CAD and Mortality - Yang et al., 2024.
(6) How to live to 100 before developing clinical coronary artery disease: a suggestion | European Heart Journal | Oxford Academic - Braunwald, 2021.