ketoconazole does not only affect oral though the factor of say ‘multiplication’ is more than for injections. I have just recently read articles(s) on that very thing - injections of rapa compared to with keto… and not and it had a very definite increase in effect such as blood levels, peak concentrations etc.
@Bicep please do not heed any advice from this wacko.
His information on isopropanol is exrtremely uninformed an inaccurate, as he seems to just willy-nilly Google shit without even bothering to READ THE SCIENCE!
For instance, this is factually incorrect:
He just googled “isopropanol LD40” and the first result of that is dermal LD50 on rabbits, which is 12.8 g/kg. That is not oral LD50, and it certainly isn’t injected LD50 which provides even more bioavailability than oral (meaning a smaller dose is equal to a larger oral dose).
If you compare that to the oral LD50 of ethanol, which is 7-12 g/kg in mice, then you can see how Dan came to the conclusion that isopropanol’s LD50 is twice that of ethanol. That is incorrect.
The opposite is actually the case - isopropanols oral LD50 in mice is ~5 g/kg. In other words, the LD50 of isopropanol is half that of ethanol.
Anyone with basic knowledge of biochemistry knows why - longer chained alcohols produce metabolites that are increasingly toxic to the body. The same goes for the opposite direction with methanol, having one carbon atom fewer than ethanol, which metabolizes to formaldehyde in your body.
Isopropanol thankfully does not metabolize into anything as horrible as formaldehyde, but it is avoided in pharmaceutical preparations for many reasons. For one, because ethanol exists! Isopropanol comes with far more side effects than ethanol, which is why it’s avoided whenever possible. The only reason Dan uses it is because he literally buys 70% rubbing alcohol from Walmart. Not joking. Here’s his post:
Furthermore, the paper he is citing that uses isopropanol is a purely explorative developmental study. In other words, just proofs-of-concept. They weren’t even tested on mice, just cell lines.
These formulation studies are done as a demonstration to say “hey it’s possible,” not as a direct-to-pharma preparation. For fuck’s sake, Dan, it says FORMULATION DEVELOPMENT in the title! Along with the words “Toxicity and Assessment!”
But you intentionally left out that last part of the title. The full title is:
Rapamycin-Loaded, CapryolTM 90 and Oleic Acid Mediated Nanoemulsions: Formulation Development, >>>Characterization and Toxicity Assessment<<<
I don’t know if you are being intentionally deceitful by omitting such an important detail, being that this is a toxicity study. I don’t know if you’re just ignorant or maliciously trying to cause harm to others in this forum by spreading misinformation. But to be honest, both cases are equally as bad.
It is often the people who refuse to seek modern, science-based medicine that end up reintroducing measles to the world.
I don’t know why you have a grudge against medicine. I have my own grievances against the system, but it is almost entirely due to the regulatory restrictions that hinder medicine, not the medicine itself.
That is exactly what you are doing. You’re throwing out all of these wildly incorrect, demonstrably false facts that have no citations, no evidence, and no reasoning other than “for the kicks.”
You have rejected every single citation, fact, and evidence that I have provided you. You seem to just believe what you want to believe, not based on proof, but on what you feel.
And you aren’t successful. You injected yourself with non-sterile tapwater from the Philippines and use Walmart rubbing alcohol in your injections, too. And surprise surprise, you got an infection from that!
Shallow and trite? So this statement of factual medical reality, is shallow and trite? And not backed by proof? Are you joking?
No, it is NOT more likely! Where are your sources? Your math?
This is demonstrably false!
An estimated 1.3 million lives in the US are lost due to unsafe injection practices, mostly related to opiates and drug abusers (which may fit your description, given your past psychedelic/ketamine injections).
Compare that to annual automobile-related mortalities in the US in 2020:
A total of 35,766 fatal car accidents for 2020. Since you won’t do the math, I’ll do it for you:
Your unsafe injection practices make you 36 times more likely to die than car accidents. Now, let’s factor in the estimated number of injection drug users within the US, which was projected to be about 3,694,50 in 2018:
Now, not all of these persons who inject drugs (PWID) do so in a dangerous and abusive manner, but let us assume the worst case scenario that all of them are drug abusers.
That means you have an annual risk of injection-related death of approximately 1 in 3 PWID. I hope you can see now why unsafe injections are such a crisis in the US and worldwide. It kills so many people that we literally have to sweep dead people off the streets in many cities of the US. This is one of the reasons why cities like LA are such hellholes nowadays.
Which is why we have to look at the data and do the math. What you’re doing, as I have calculated, isn’t something that might happen. It is extremely likely to happen, especially if you continue this behavior. This is why I am telling you to seek medical counsel. You need both mental care and drug rehabilitation.
No, it is the fact you don’t know it that demonstrates to me your lack of knowledge on what you are doing. You bragged about being able to do a simple high school derivation of calculus as if that makes you an expert, yet you can’t even recognize one of the most basic of pharmaceutical equations.
That equation was for plasma concentration, by the way. The fact you didn’t even bother to Google it speaks volumes of your willingness to actually research and validate information.
Quantum level biological chemistry? What the hell is that? Do you even know what you’re talking about? I hope you aren’t being serious.
They aren’t “know it alls,” the only one acting like a know-it-all is YOU. And like I said before, those doctors obviously know how to derive a simple calculus equation. Whereas you cannot even recognize the plasma concentration formula, a damned introductory pharma equation that you could’ve Googled. I didn’t even ask you to solve it, or derive it, just to name it. And you didn’t.
Danny boy, when they tell you not to inject yourself with tap water from the Philippines, perhaps you should listen.
Now let me turn one of your one-liners unto you.
I asked you to name a basic pharma equation, and you couldn’t come up with an answer on the spot. What does that say about what you know?
9 Likes
Isn’t that mostly because of drugs laced with or usage of Mexican fentanyl made with Chinese precursors?
1 Like
That is one factor among many. Like I said before, I just made an estimate because there are far too many variables to make an accurate projection. Overdosing from miscalculated at-home measurements, infections and death from non-sterile needles and/or drugs, etc.
Also, as you said yourself, that fentanyl had Chinese precursor chemicals. The purity of such precursors often determines what toxic byproducts are produced, such as formaldehyde. Dan gets almost all his chemicals from China, as he says himself, and he does nothing to verify their purity.
What Dan is doing is a combination of the worst unsafe injection practices.
-
He is likely doing everything non-sterile
-
He purchases from foreign countries (China) with no assurance as to their quality and/or contaminants, and uses concerning budget ingredients like Walmart isopropanol in his injections
-
He doesn’t seem to understand how to measure out dosages and since he refuses to interact with any doctors he has zilch in regard to monitoring his own biomarkers for anything dangerous. So, he is at risk of OD’ing, which can be seen in his excessive 20-30 mg per 5 days injection routine of rapamycin
-
He takes and has taken a myriad of drugs which are easily abused, such as psychedelics, ketamine, growth hormone, etc.
3 Likes
He’s got to be trolling us?
7 Likes
O_o
This person is FU.
If he in not, he is writing this to get attention.
Why use your time and energy to try explaining?
If people ignore him all on this forum would be better off.
This is my view.
5 Likes
I am concerned for his well-being and health, and he is also posting a lot of factually incorrect information that can potentially cause serious harm if taken as advice.
But yes, you are right. I shouldn’t be spending this much time and effort. I’ll leave Dan to his posts for now.
I hope he is. The alternative is horrifying.
4 Likes
I really appreciate you giving us all the benefit of your expertise in this. Don’t worry about me though, I don’t inject.
I raise mushrooms and it took me a very long time to figure out how to make a petri dish sterile. Of course being a farmer I cut all the corners and it didn’t work. Sterile in my basement is very hard work. In my case making these mistakes just means contaminated spawn which gets dumped in the garden. BTW I did eventually get it, I’m looking at 15 beautiful petri dishes of Loin’s Mane and not a speck of contamination in any of them. If I want uncontaminated water I use UVC light and pressure cook. That’s for a mushroom.
I wish I could remember what percent of Rapa gets absorbed the way we do it with the biocon oral route. It has to be less that 14 % or Agetron’s 7x is obviously wrong because you can’t absorb more than 100% no matter how much gfj you drink.
3 Likes
No problem, and also it’s nice to see a mushroom grower in this forum! And Lion’s Mane, too! Very cool stuff ![]()
Sterile work is indeed a PITA, and it also took a long time before I got my cultures right - though I was growing HeLa cells instead of spores like you are. Mushroom growers actually share a lot in common with pharmaceutical scientists for that reason. In fact, a local grower once helped me build a sterile prep space for a high school laboratory so they could do petri plate lessons. Much respect to the growers ![]()
Also, I think Agetron’s 7x is in regard to his own bioavailability. Rapamycin typically has an oral bioavailability of 10-15%, but we all have different absorption profiles based on diet, genetics, etc. I think he just had a rather poor absorption that was dramatically increased by GFJ.
However, that is with a single dose. When you take multiple doses over time, there will be some leftover rapamycin in your system from your previous dose. This is what is known as a trough level or therapeutic dose window. So, depending on when Agetron measured his levels, he could have actually been seeing the collective rapamycin in his system being dumped by GFJ at once. This is why I’m personally not that much a fan of GFJ, as its effect on your drug metabolism/absorption is inconsistent and unpredictable.
3 Likes
I don’t understand how anyone can inject things every five days either way, unless you are or have been a drug abuser in the past and associate injections with positive valence.
1 Like
There actually are millions of injection drug users who use a 5-day schedule or even daily schedule.
The most common example is for HRT, and a few of them are actually in this forum. You’ve probably heard of testosterone replacement therapy (TRT), which is quite effective for older adults whose T levels crater with age.
Some unfortunate folks are also born with hormone deficiencies, in which case they would need to be supplemented with hormone injections.
However, these people usually do it under a prescription and with the careful monitoring of a medical professional. These people are separate from the PWID statistics I posted earlier, which are more about those who abuse injectable drugs.
3 Likes
I meant in the case there is an alternative, like oral rapamycin or testosterone gels, patches.
It’s specific to this case of course, and can’t be generalized .
O_o wrote: depending on when Agetron measured his levels, he could have actually been seeing the collective rapamycin in his system being dumped by GFJ at once.
To clarify…I took a Labcorp blood test for trough then took dose. Which was .7
Retested with Labcorp 1 1/2 to 2 hours later for my t-max. 38.2
Trough
T-max
I am fortunate that my PCP assists me as much as possible…literally letting me do two blood draws within hours… he is amazing.
I will be doing a blood draw for trough and then another 2 hours after for t-max of my dose… now 2 mg and GFJ… at a 6x’s increase ahould be at 12 ng/mL… we will see.
4 Likes
And what dose did you take before this pair of tests? And this time you will take 2+gfj?
There is a misunderstanding here about the multiplier, the effective dose, and the blood level.
Say you take 15mg with no GFJ, and blood level comes up 30. Are you saying your body has a natural multiplier of 2x?
Say the same guy takes 3+GFJ and blood level comes up 30. He would have a multiplier of 5. Not 10. He takes 3 and his blood level is 30, but don’t let that confuse you. The dimentions of blood level are in ng/ml blood. The dimentions of the Rapa are just mg. The multiplier just says how well it goes through the gut.
Look forward to learning something from the next test anyway. Thanks,
2 Likes
Thanks for all the detailed information. I have put Dans account on silence for a few months because i feel hes spreading too much misinformation and that he is too reckless in his use of drugs and in his research. I am considering whether to ban him entirely.
He is welcome to read and learn.
11 Likes
Ah, yes, my bad AnUser. I misunderstood what you were saying.
Indeed, most would prefer routes without having to jab a needle into yourself. Self injections are hardcore.
I see now, it’ a c-max value that Bicep was referencing and not a percentage. That makes a lot more sense now. Achieving 7x of your c-max is a lot different from 7x the percent bioavailabilty. My bad, Agetron.
To explain what is happening here, I’ll have to show this chart:
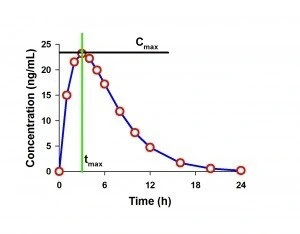
The t-max is simply the time after a dose at which the concentration in blood is at its highest. The value he gave, being 38.2 ng/mL, is the c-max, or the maximum concentration in blood at the t-max.
When you stated an increase in the percent bioavailability, I thought you were talking about the AUC - area under the curve. This is typically what biochemists refer to when saying “percent bioavailability”. That was a misunderstanding on my part when you stated a percentage.
You see, if you derive the area under the curve you can calculate the total amount of drug that was actually absorbed into the bloodstream. So, having a 7x increase in the c-max doesn’t mean you increased the bioavailability by 7x. In order to determine that accurately, you need a LOT more data points in order to fit a curve and derive the AUC.
Now, that is not only expensive and tedious to do, but also quite difficult. I’m surprised that Agetron has a PCP that allowed him to do back-to-back blood draws like that, pretty cool! But I think even his PCP would balk at the idea of taking 12 or more blood draws spread across a single day. So, it’s better to simply look at the peak and trough level as a rough estimate of the increase in bioavailability. You can only plot a triangle on the chart, but it still gives you an idea of how much more you’re getting out of each dose.
That sounds like a reasonable action. Hopefully when he returns, he will have a different perspective on his drug use. I genuinely wish him well, but I’m just not sure I can ever convince him to change his habits.
5 Likes
It’s not your bad, but that what I was meant and it wasn’t totally clear.
I wouldn’t be surprised if Dan was on some kind of drug while writing what he did. Or a manic episode of some sort, based on the writing style.
1 Like
I have a small quantity (1 gram) of LGD4033 in my basement. I have not ingested any of it and I may never do so. There are serious risks with ingesting a powder of dubious origin. The powder came with a certificate from a US lab, but anyone can get certificates printed. I would never have considered taking Rapamycin imported from India if I had not read the positive experiences of users on this forum. Lgd4033 is not even a drug at this point–it is considered a research chemical. This compound may reduce prostate bph, and may prevent, or be useful in the treatment of prostate cancer. LGD4033 also shuts down natural testosterone production and may cause heart or liver problems. This is as edgy as I get. I am looking for drugs that might prove very useful that are at risk of being banned.
Normal oral Rapamycin absorption is about 10-15%
2 Likes
I post last year about performing multiple BT/ what you call back to back.
Coping the testing, like doing GTT
One BD a base, take the rapamycin dose, then one BD 20 min, then 45, then 1 hour, then every hour for 8 hour. Total would be 13BD over 8 hours.{you can do more BD over more/longer time, ever draw cost an additional $66.00] Then you would have an idea on how much is absorbed for that individual using whatever brand of rapamycin.{different brand will show different absorbing rates]
The issue would be the cost,{13 X $66.00] all would be out of pocket. All day at LabCorp with precise times of the BD, either being pierced 13 times or more humane having a catheter installed from the first BD.
Your personalized dosing rate/schedule.
Any self funding volunteer?
Or anyone pick up the cost and I will volunteer?