When I took 1.25 mg/day, lunalae appeared on my fingers; they disappeared when I stopped. I stopped because I felt weird in my heart (very subjective, yes, but it does seem to have negative effects per this recent paper: MAO-B inhibition by selegiline blunts cardiac functions improved by high-fat diet: Role of inflammation, apoptosis, and calcium-handling 2025) and wasn’t sure about long-term safety. Unfortunately, we’ll only get the ITP results in September 2028…
5 Likes
started taking 1.25 mg after seeing Paul Keisow’s talk. No noticeable effects after 3 weeks but I am looking for long term benefits as have a family history of PD
2 Likes
There’s no evidence that selegiline can prevent PD before diagnosis or slow it down after diagnosis. For PD prevention, I would look at:
- SGLT2i (dapagliflozin or empagliflozin)
- Telmisartan
- Amlodipine
- UDCA
- Avoiding statins
- Lithium orotate
- Rapamycin
See the dedicated thread: Parkinson's disease
6 Likes
I’m still taking 1.25mg tabs every morning upon waking. I think I have been taking this for almost ten years now. I don’t notice anything from it, but I’ve also been using it for such a long time.
3 Likes
It would be interesting if you were to stop it for couple months to see if you notice anything different.
BTW, since you started it such long time ago what was your reason (initially) for starting it?
1 Like
For the sake of completeness, one can add a couple more things which are not decisive in any way, but might be helpful in some cases, just really throwing the kitchen sink at this terrible disease. One is to top up vitamin b1/b2 (I mention both because taking larger amounts of one can imbalance the other) to at least RDA. Keep inflammation low, perhaps add astaxanthin, maintain gut integrity against LPS with some probiotic additions or even direct tributyrin, avoid pesticides in general maybe eat organics in F&V. And super speculative - add some magnesium threonate (I’ll post a study in the PD thread). There’s a bunch others, but all speculative.
1 Like
I initially started it because I saw an article in Life Extension magazine when I really started to get into health and they made it sound really good so I ordered some. I did stop at one point and then started it again. I can’t say I noticed too much of a subjective difference either way.
2 Likes
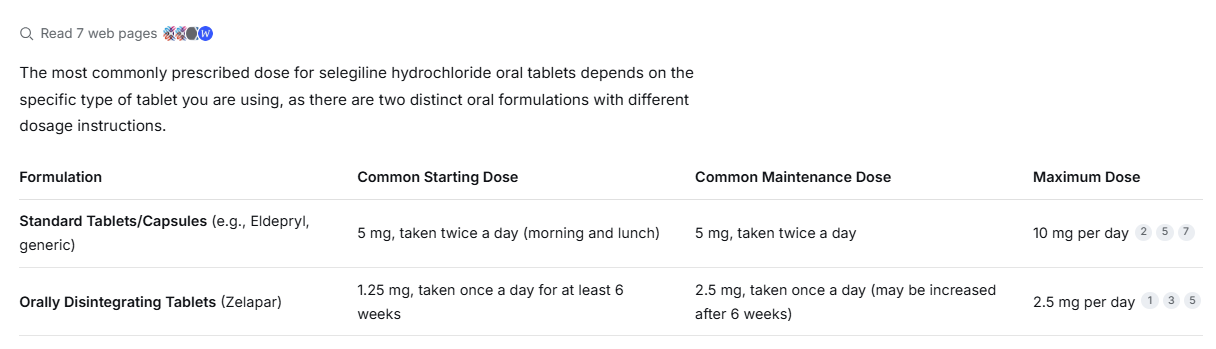
After reading grok’s answer to what I asked, I think I will increase my dose to 2.5 mg. I feel like the 1.25mg isn’t really doing anything. The human equivalent doses used in the studies were mostly 1.5-3mg for a 70kg human (I’m 94kg)
Grok
The evidence for selegiline (L-deprenyl) extending lifespan in animals is moderately strong overall, primarily driven by a 2025 meta-analysis synthesizing decades of rodent data, though results show notable variability and are weaker/less consistent in non-rodents. 
A random-effects meta-analysis (published in Ageing Research Reviews) of 22 rodent lifespan experiments (covering mice, rats, and hamsters across 8 strains, 6 countries, 27 years of research, 6 doses, and 2 delivery methods) found that L-deprenyl significantly increases average lifespan with a moderate effect size (standardized mean difference [SMD] = 0.6773, p = 0.0002). There was no significant publication bias, but substantial heterogeneity between studies. Effects were dose- and age-dependent: higher doses and starting treatment later in life produced larger benefits. Short-lived control groups did not explain the results.  
Key supporting studies include:
• Joseph Knoll’s seminal 1988 work (and follow-ups): Male rats treated with 0.25 mg/kg s.c. three times weekly from ~24 months of age showed dramatic extensions (average lifespan ~147–148 weeks in controls vs. ~192–198 weeks in treated; some individuals exceeded the species’ estimated maximum of ~182 weeks). Sexual activity and other markers also improved markedly.  
• Replications by Kitani et al. and others in F344 rats (e.g., 0.5 mg/kg s.c. three times weekly from 18 months): ~10–34% increases in average remaining lifespan, with parallel upregulation of antioxidant enzymes (SOD/catalase) proposed as a mechanism. 
• Positive but smaller effects in mice (e.g., ~7–9% in aged animals at 0.25 mg/kg), Syrian hamsters (especially females at low doses like 0.05 mg/kg), and other rodent strains. 
Limitations temper the strength:
• High heterogeneity: Some studies (especially in mice) found null, minimal, or even negative effects at improper doses (hormetic/inverted-U response—too high a dose can shorten life). 
• One beagle dog study (Ruehl et al., 1997): 1 mg/kg oral daily in elderly dogs (10–15 years at start) showed apparent survival benefit in a subset (80% treated vs. 39% controls survived study period), but reanalysis adjusting for age/sex found only a non-significant trend (limited power, small n).  
• No consistent effects across all protocols or species; mechanisms (MAO-B inhibition, catecholaminergic enhancement, antioxidant upregulation) are plausible but not fully proven as causal for longevity.
Overall, this is one of the more robust pharmacological lifespan datasets in mammals (far more studies than most compounds), but replication inconsistencies and lack of modern standardized trials mean it’s not “conclusive” like caloric restriction or certain genetic interventions. No human longevity trials exist (though selegiline is FDA-approved/safe for Parkinson’s/depression at low doses).
Human equivalent doses (HED) from the effective animal studies are low and overlap with or fall below standard clinical doses.
Allometric scaling (FDA body surface area method: rat Km=6, human=37 → multiply animal mg/kg by ~0.162; adjust for intermittent dosing) from the most common/effective rodent protocols (0.25–0.5 mg/kg s.c. three times weekly, or daily averages ~0.1–0.2 mg/kg) yields ~1.5–3 mg/day oral for a 70 kg (~155 lb) human. This matches statements from summaries of the meta-analysis. 
• Knoll’s classic 0.25 mg/kg rat dose (3x/week) ≈ ~1–1.5 mg/day HED.
• Kitani-style 0.5 mg/kg ≈ ~2–3 mg/day HED.
• These are roughly equivalent to (or below) typical Parkinson’s oral tablets (1.25–10 mg/day) or well below the transdermal patch (6–12 mg/day). The meta-analysis notes that higher animal doses (and later start) were more effective, so the patch range might align better if translating directly. 
Dog doses (1 mg/kg oral daily) scale higher (~30–40 mg/day HED) but are less relevant given the weaker evidence. Low “enhancer-only” doses (e.g., 0.001–0.1 mg/kg in later Knoll work) had smaller or inconsistent effects.
Bottom line: Solid preclinical signal in rodents (meta-supported moderate extension, dose/age optimized), translatable to very low human-equivalent oral doses already used safely in medicine. Human anti-aging trials would be needed to confirm any benefit—none exist yet. Consult a physician before any off-label use, as selegiline has interactions (e.g., with certain antidepressants/foods at high doses).
3 Likes
Did this trial ever take place, and can you share any more info. Thanks,
1 Like
I did take it for a while but haven’t lately. I ended up not noticing much beyond an initial libido boost which was nice but short lived. I never had any interactions with tyramine rich foods when I was on it.
2 Likes
Maybe I missed something, but you and others appear to be taking too low of a dose, unless you are taking the orally disintegrating form. Is anyone using the patch form?
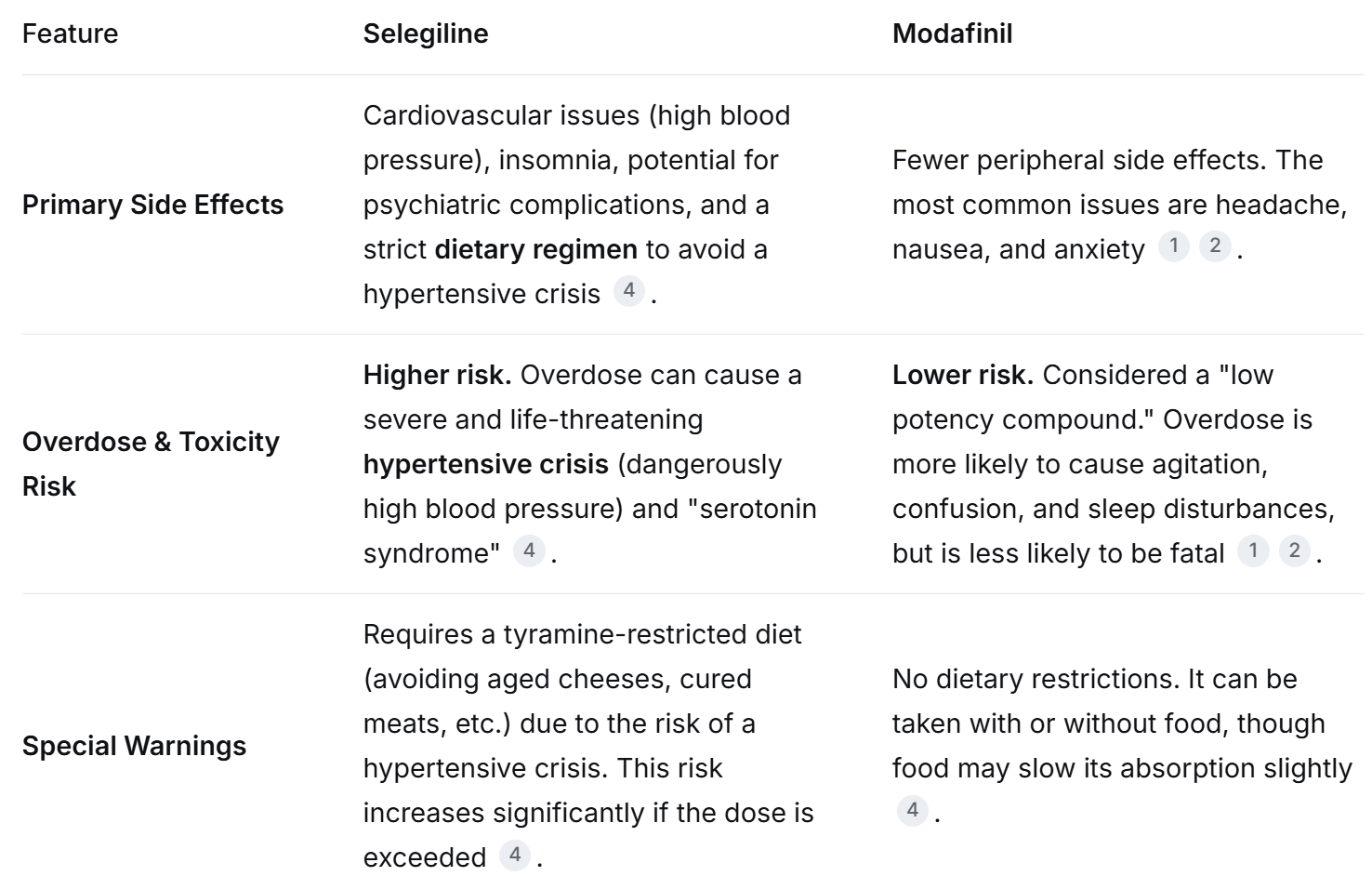
I don’t think it is a high-risk drug, but I commonly eat tyramine-rich foods. Also FWIW: AI thinks that selegiline is the more risky drug for the elderly.
The risk of a hypertensive “cheese reaction” from eating tyramine-rich foods (like aged cheese or cured meats) is generally considered low but not zero. Rare cases have been reported, so some caution is still advised.
I was considering trying selgiline, but I think that I will pass for now. Modafinil is serving me well.
2 Likes
I agree with you after doing a little more research the other day and decided to increase my dose to 2.5mg every morning
2 Likes
whatever happened to those two?
I used to follow them
1 Like
@CronosTempi: what are your views on selegiline?
Who are the selegiline users here? @LukeMV: how is your higher dose experimentation going?
I’m considering giving it another try… Of maybe I should just wait for the ITP results but 2y is a long time ![]()
2 Likes
Every biohacker has their own risk tolerance and stack inclusion criteria. This may be surprising to some, but I am pretty conservative wrt. my stack, and selegiline is outside my comfort zone. I regard it as a research molecule. The studies out there are quite unsatisfying and all over the place - nothing there inspires my confidence. Dosing protocols are a huge unknown. DDI potential is high - I prefer to protect the rest of my stack which I have a decent degree of confidence in, and do not see the sense of introducing an unpredictable stranger to our stable little family.
General remark: there are literally thousands of molecules about which there are claims that they are beneficial for something or other. But if I feel that for example my systemic (dry) inflammation is already quite low (hsCRP, IL-6, GlycA, WBC, netrophils etc.), why should I care that Latest Wonder Drug supposedly is “good for dry inflammation”? There are a thousand other “good for inflammation” supps out there - I feel no need to add them to my stack. Same for “neuroprotection”, “endothelium”, “x, y, z”. If my biomarkers are where I want them (example: inflammatory markers) I don’t need more. In the film industry there is an expression describing excessive effects: “a hat on a hat”. I already have a hat, I don’t need to put another hat on top of my hat. This in general is a huge problem in the approach of many biohackers: a shiny new - or old - supp/drug has its 15 minutes of fame and everyone jumps on the bandwagon regardless of whether they need it or not, just because “it’s beneficial for x”… fishoil anyone? “Oh, it’s neuroprotective!”… please🙄.
Why do I need - or want - selegiline? It must show that it does something that no other drug/supp in my stack does, OR does it better than a drug in my stack, and fits within my specific medical situation. And the inclusion bar is VERY high - even ITP results don’t assure inclusion. Metformin + rapamycin give good longevity results in rodents, but I STILL do not take metformin, because it does not fit with the rest of my regimen and personal medical situation.
Of course, selegiline has a PD indication. OK. But, call it prejudice, or excessive caution, but anything that touches dopamine in PD I am super careful and paranoid about (for example levodopa). Furthermore, I want to see long term effects, and lifespan data is not encouraging for selegiline in PD. I have an open mind about deprenyl and PD, but I am pretty cautious about it.
Bottom line: for me selegiline is a PASS at this time.
Sorry for the length, and YMMV - of course others may have a different experience or evaluation, no judgement from me, just giving my one man opinion (and only because I was asked).
1 Like
Thanks. I agree and that’s why I stopped it but a conversation with a researcher yesterday made me question that. Anyway, did you share your whole stack somewhere on the forum?
2 Likes
I haven’t had any side effects at all other than very bitter taste. I am very careful also when it comes to substances that mess with DOPA but this one seems very subtle to the point most may not notice anything, yet it must do something since for me I do get benefits. Comparing it with Modafinil as an example I would not take Moda long term even though the effects are more pronounced but it definitely has side effects and you can easily tell when it wears off whereas Selegiline nothing none just a small but much needed uplift in mood and wellbeing and you don’t feel anything while it wears off. The only time I feel a bit of a difference is if I don’t take it for 3-4 days and then my mood goes I guess to baseline. It is my opinion that everyone should take. Benefits are small but noticeable for me in form of uplifting mood and calmer. I do 1.25mg under the tongue. It is something that I’ll continue for life, definitely.
BTW, what is DDI? (you said DDI potential is high)
Yes. Obviously, my stack is geared to my specific medical situation, genetic vulnerabilities, age (67-68) and obsessions (CVD, brain health, prostate etc.).
Short version.
Prescription drugs:
1)pitavastatin 4mg/day
2)bempedoic acid 180mg/day
3)ezetimibe 10mg/day
4)telmisartan 80mg/day
5)empagliflozin 25mg/day
6)rapamycin 8mg/1-week
Still doing research, may add imeglimin, may swap olmesartan for telmisartan.
Supps are more fluid, with things added or removed over time and more complicated dosing protocols, but some more stable and regular ones: lithium orotate, carotenoids (astaxanthin, lutein, zeaxanthin, mesozeaxanthin, lycopene), benfotiamine, vit.D3, K1,2, super low dose melatonin (0.3mg/day), ergothioneine, EPA (500mg/2-week), magnesium threonate, and some stuff that is more complicated, occasional or shifting.
@Kelman - Drug Drug Interactions.
5 Likes
I actually stopped taking it because I decided to get on Wellbutrin to boost my mood/energy and you’re not supposed to combine the two. I honestly doubt taking 2.5mg Selegiline would be an issue but I’d rather be safe than sorry. I couldn’t really tell is the 2.5mg was doing anything differently than 1.25mg though. If I ever stop Wellbutrin, I’d start Selegiline back up again.
4 Likes
I hadn’t heard of the energy component. But certainly for the elderly, Wellbutrin would be the safer bet.
Sorry, please describe your experience with Wellbutrin? Did you get some more energy? Did you experience any unpleasant side effects, such as sleep disturbance? What dose are you taking, and how long before you experienced any subjective results?
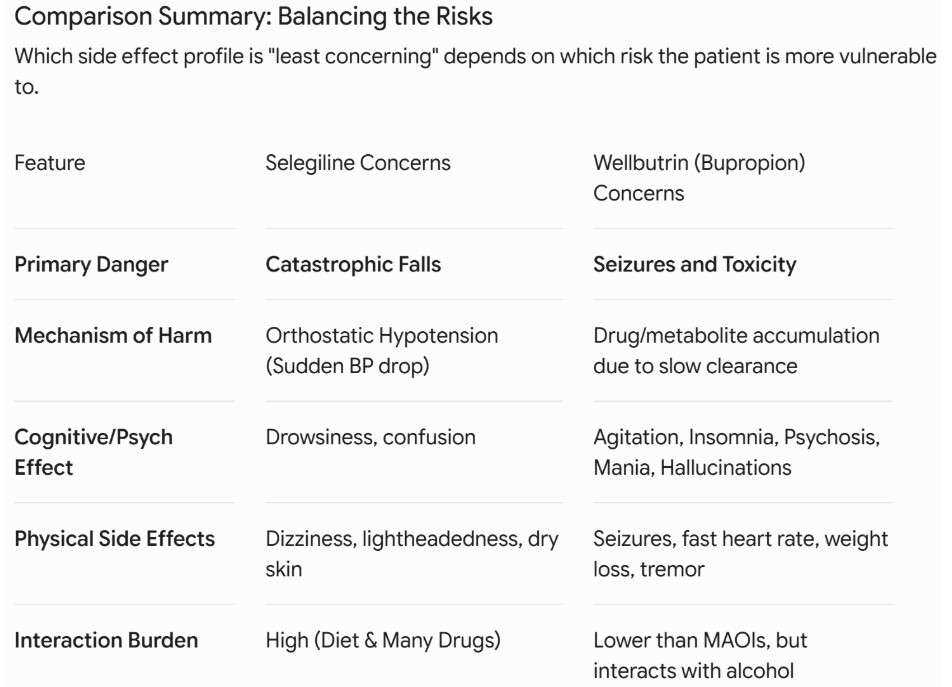
Gemini Pro: Comparison for the elderly
[image]
*Wellbutrin: Seizure Risk (Boxed Warning): Seizures are a known, dose-dependent risk of bupropion, occurring in less than 1% of people at recommended doses, but this risk increases significantly with high blood levels.
*Selegiline: While lower doses of selegiline (especially the patch) have a safer metabolic profile, the risk remains a significant cognitive burden for a patient to manage. Selegiline also has major interactions with many other common drugs (major drug interactions noted with 131 drugs)
2 Likes