Eggplant and blueberries
I stopped doing keto for a bit 2 days ago (social reasons/free food → enough veggies will elevate BG), blood glucose levels are now more normal (but no glucose spikes). Am just going to wait for ketone esters. I only needed 4 hours of sleep last night! (and very little for most of the past week). Have not been getting hypoglycemic the last two days either (and yes going hypoglycemic does feel bad)
resting heart rate increased to 81.
But again, needing less sleep makes keto worth it in itself so I’ll continue to eat high-fat and avoid legumes and most fruits. A week of constant hypoglycemia might be enough to shift my metabolism into fat-burning mode which is what matters way more than long-term keto.
i did SO MUCH research into eric verdin/juvlabs earlier this week - this could change EVERYTHING. Edward Kmett does ketone esters and he only needs 3-4 hours of sleep per night.
I feel much better now than the beginning of this year.
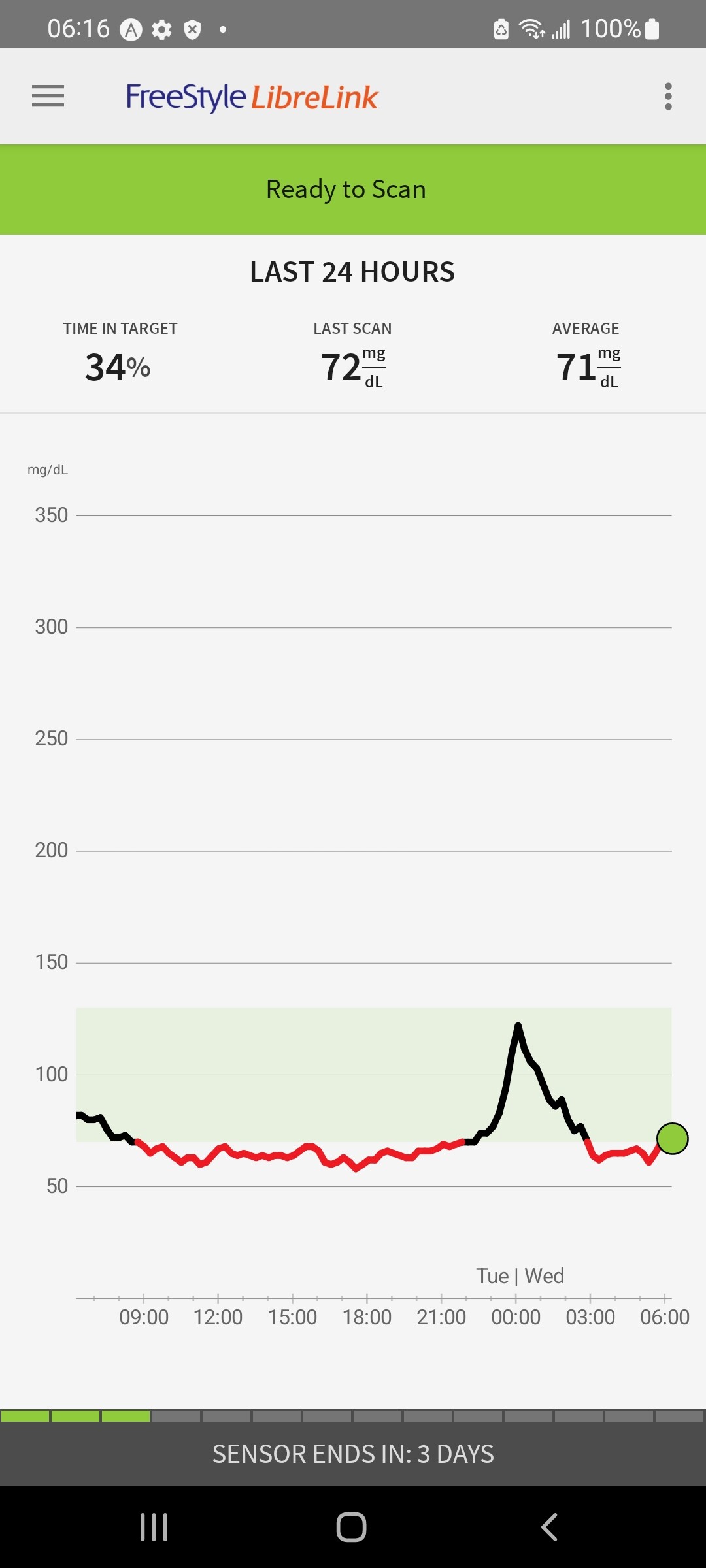
Horrifying surprise… acai berries spiked to 143… then 166… shit… i did like 3 heapful spoons worth of it (which was probably like 5-6 tablespoons total?)
1 Like
I have updated blood tests. All my lab results here - General Health and Longevity - CR Society Forum
High fat/low carb over the past 40 days, but no real change in biomarkers (yet). Intend to continue for a while b/c I like not having to take acarbose/SGLT2 inhibitors and olives make it easy enough to stay low-carb
My RDW went way up and I don’t know why. I wonder if energy drinks (even Rowdy ones) did it in…
If your MCV is changing then RDW should go up whilst it is changing.
OS (bottom one) has FLV % that is too high in one region… other is super-healthy…
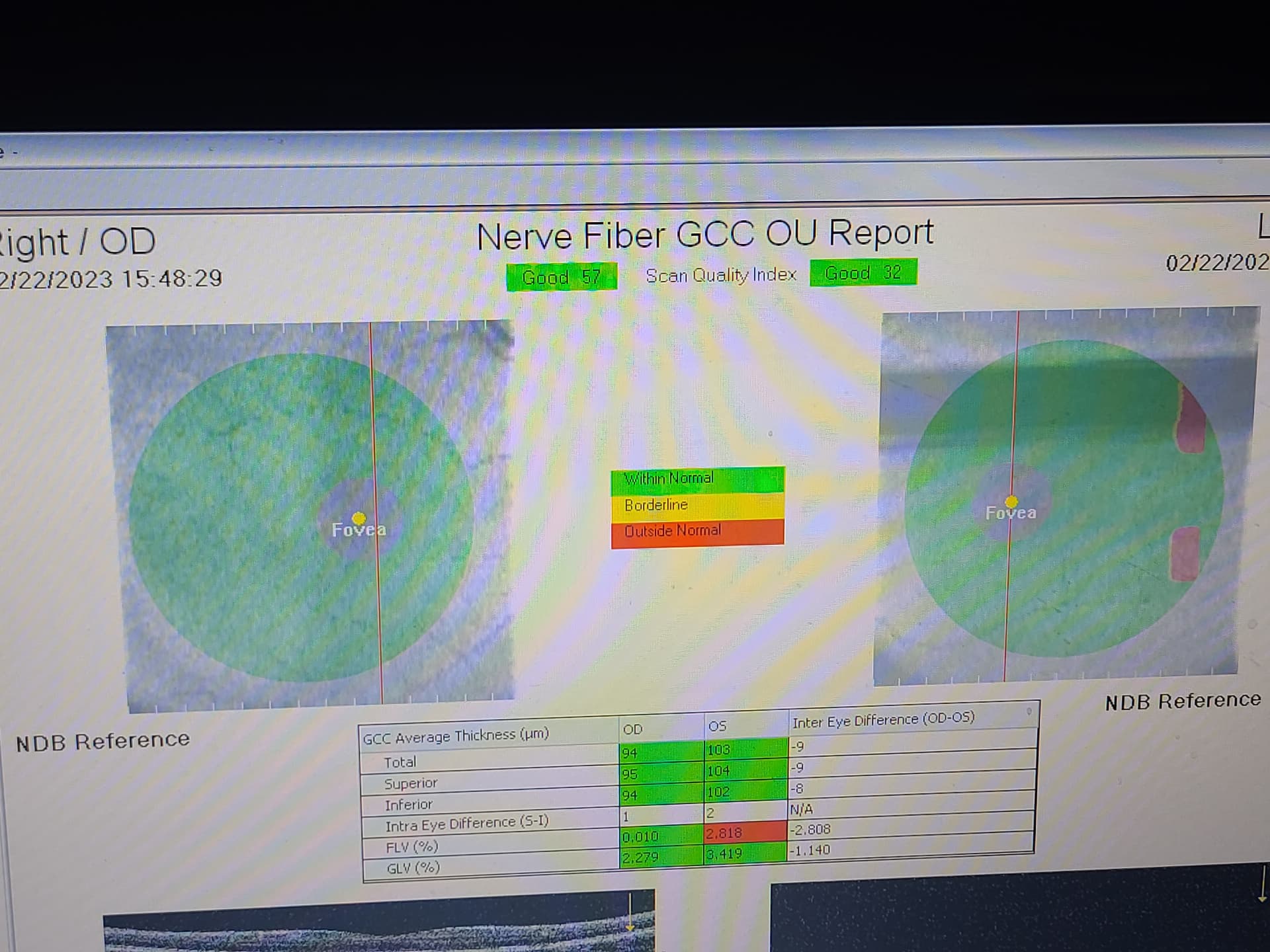
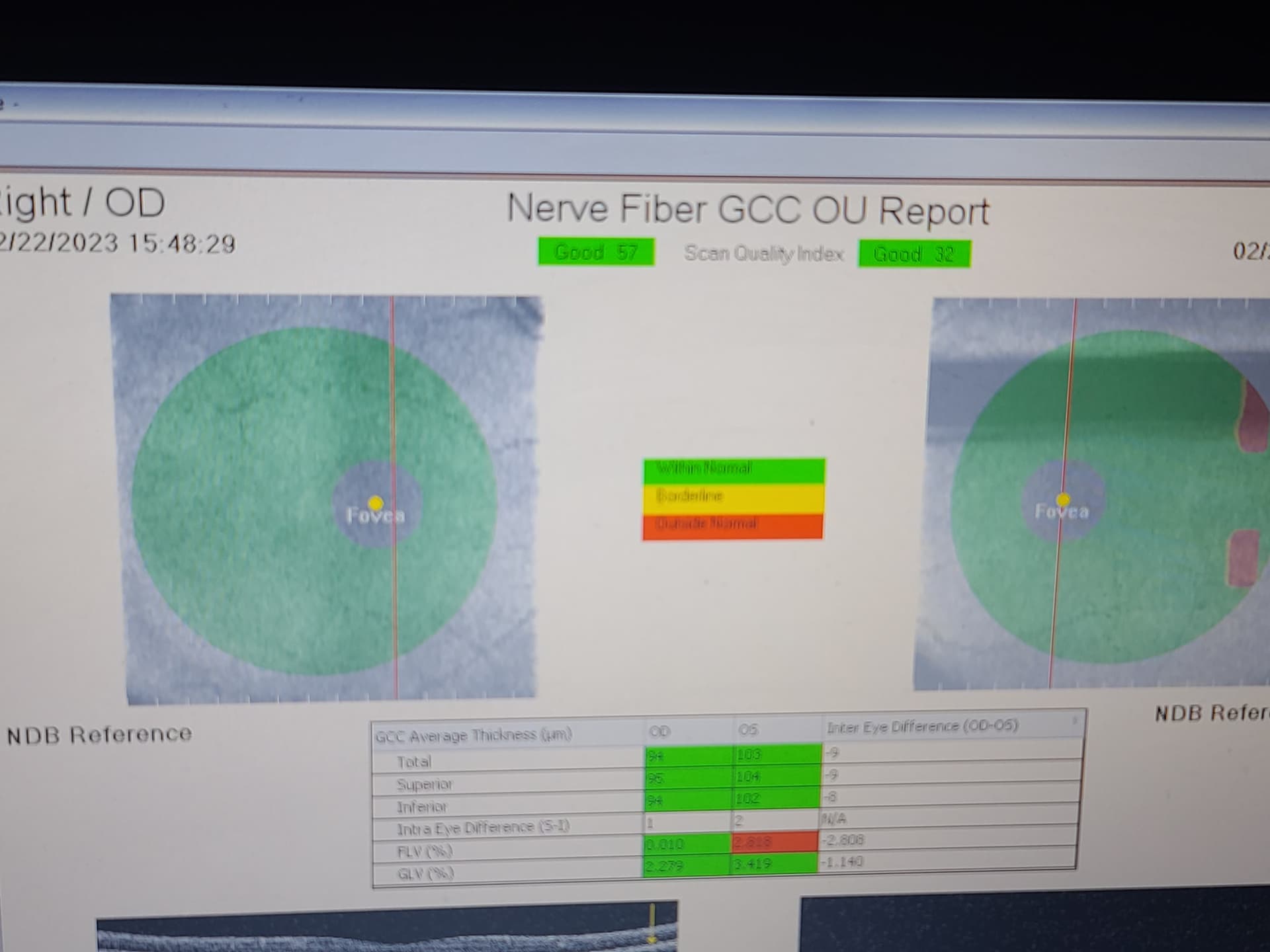
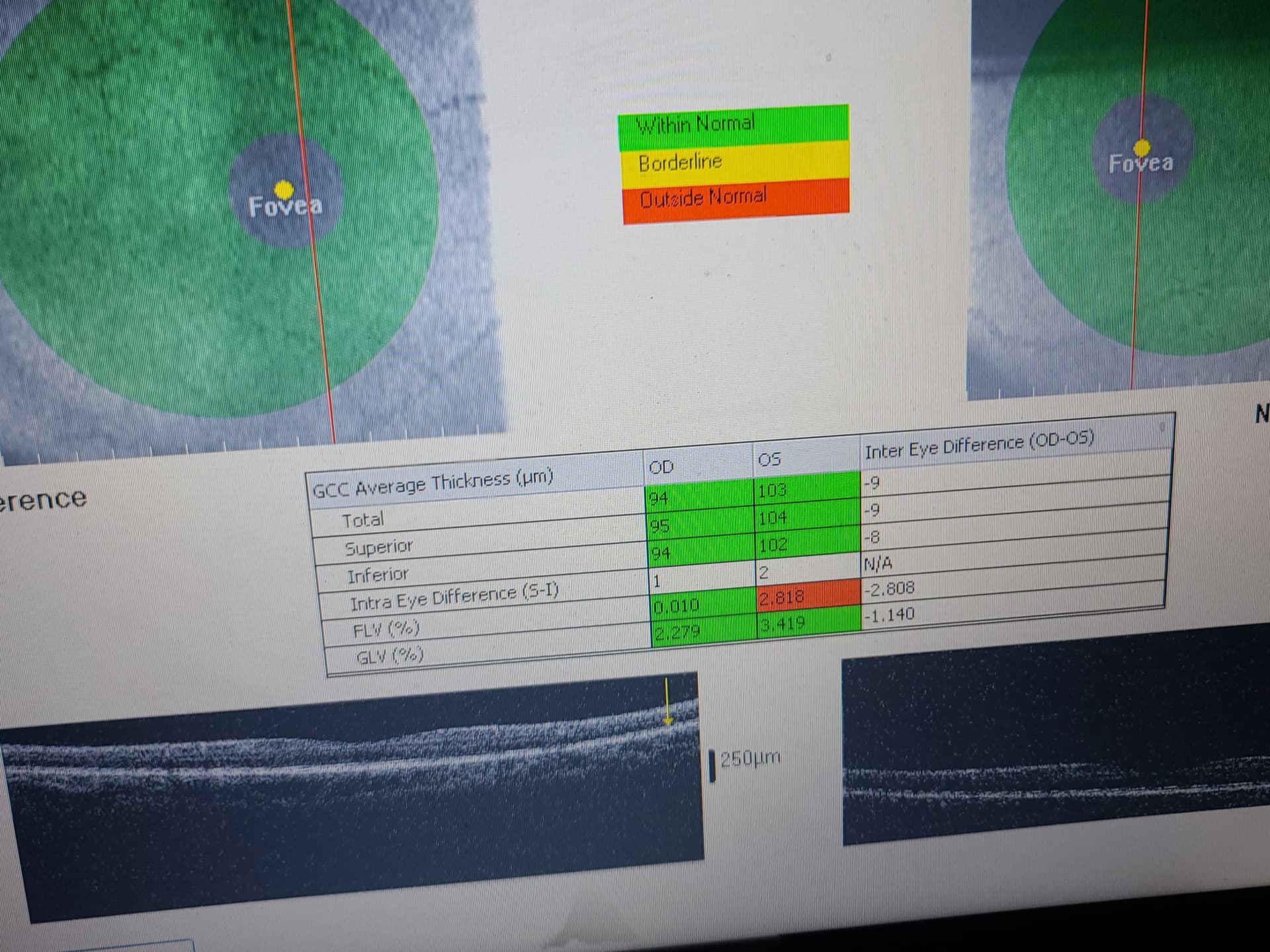
Hm focal loss volume (FLV %) in OS is a bit too high (slightly worrisome?)
PPG = pre-perimetric glaucoma has FLV% averages in that range (but not GLV%)
Could you comment on this video with The Godfather of Melatonin research? He suggests that people late in life might take 50-150mg depending on their issues.

I had reliability issues with several consumer grade BP meters including ones from Balance Health and Omron. They usually err on the side of higher reading than actual, but I have seen the reverse as well when I was experimenting with various meters in the same sitting. In one occasion I took my meter with me to my doctor visit to compare with their higher grade triage BP meter. The result: some 6 or 7 higher on my device. A year ago my doctor at Kaiser sent me home with one from their medical devices stock which also uploads the data to the app/medical record. I am very satisfied with the device made by Omron (model HEM-8210T0), more expensive than the usual consumer grade BP meters. Turns out I have no high BP issues. For what it is worth, I google the model and I was able to find it for sale at around $280 from what looks like a medical devices seller. The link:
2 Likes
Starting again, but will post on My continuous glucose monitor (CGM) logging - Chitchat - CR Society Forum [threads here get unwieldy with size]
I don’t take rapa, so I’ve never considered this question.
My two cents:
- Sotagliflozin and dapagliflozin were approved in Europe for Type 1 diabetes. They’re not approved anymore but “the removal of the type 1 diabetes indication is not because of any new safety concerns” (details of this complex case)
- In T1D, “the analysis of the regression plot (Fig 3) indicates that the DKA risk starts to increase with BMI ≥27.00 kg/m2, which coincides with the cut-off of approval for SGLT2i in Europe.” as “they are more prone to unrestricted FFA lipolysis from their increased triglyceride stores during the negative glucose balance and insulin dose down-titration induced by SGLT2i” (Assessing the risk of ketoacidosis due to sodium-glucose cotransporter (SGLT)-2 inhibitors in patients with type 1 diabetes: A meta-analysis and meta-regression)
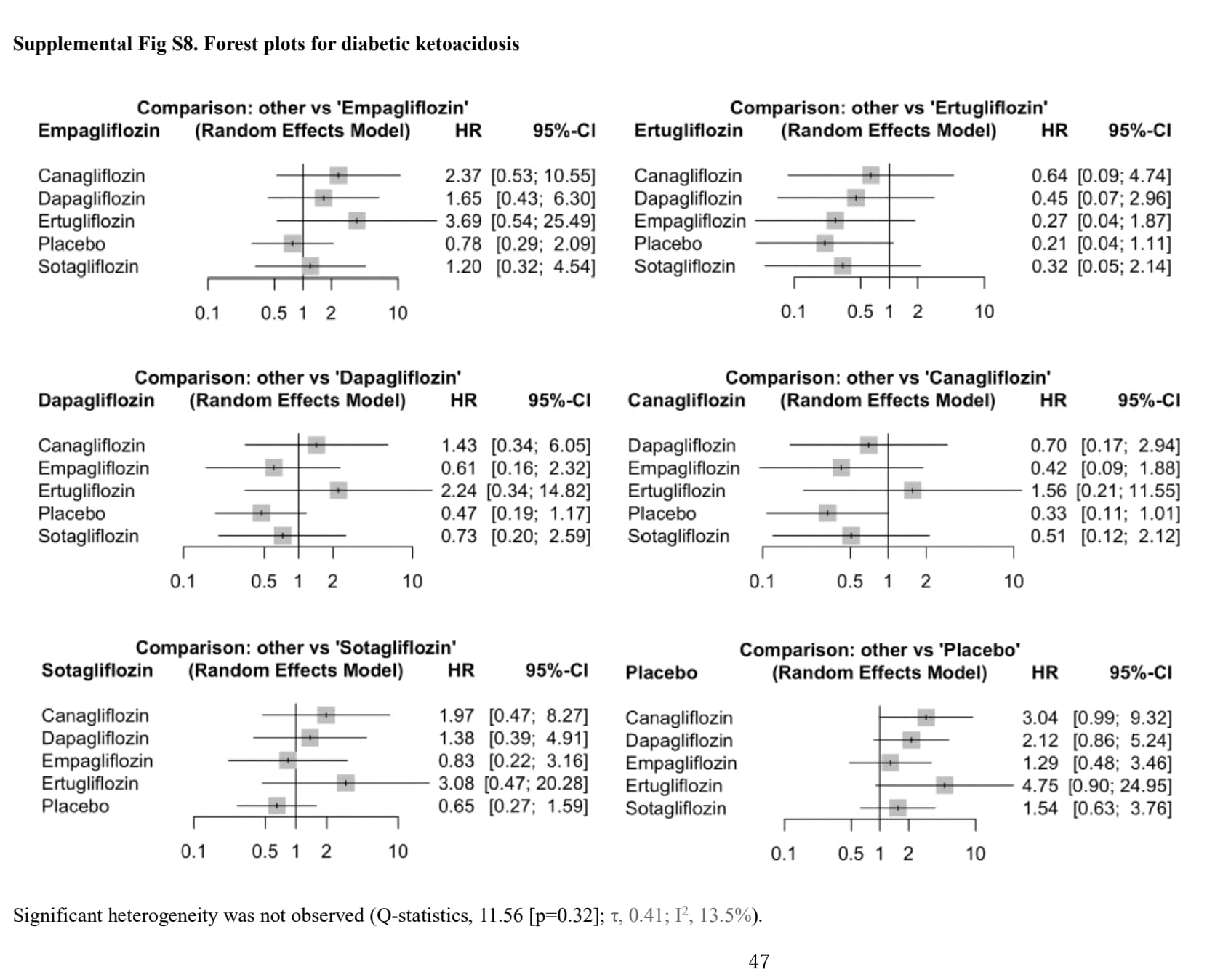
- The DKA risk is dose-dependent (see Fig 2. Forest plot of comparison: SGLT2 inhibitors, outcome: incident diabetic ketoacidosis (DKA). in the above paper).
- SGLTi are approved in non-diabetic people for CKD and HF.
- For empagliflozin, the risk of DKA on SGLT2 is not higher than placebo: Comparison of Effectiveness Among Different Sodium‐Glucose Cotransoporter‐2 Inhibitors According to Underlying Conditions: A Network Meta‐Analysis of Randomized Controlled Trials 2024
- For fasting, several papers looked at this such as Recommendations for management of diabetes during Ramadan: update 2020, applying the principles of the ADA/EASD consensus 2020: “Since the last Ramadan update in 2015, several studies have shown the safety of the SGLT2i class during Ramadan including lower risk of hypoglycemia and renal safety. However, careful pre-Ramadan assessment and education is important including advice on hydration and potential risk of volume contraction and postural hypotension, especially in warm climates with long fasting hours and risk of diabetic ketoacidosis (DKA). Testing for ketones when unwell is required for all patients who chose to fast and are using SGLT2i.”
So if SGLTi (and especially empagliflozin) are safe in nondiabetic people fasting (and also in T1D?), then I feel like we would need rapamycin to be an extremely potent inhibitor of insulin secretion to have any concern.
In doubt, check ketones + prefer empagliflozin 10 mg?
(On the other hand, we know that SGLTi increase the risk of genital infections by 4, and taking an immunosuppressant might not be great with GIs.)
3 Likes
It might be a choice either of rapamycin or SGLT2i when it comes down to it.
1 Like
Could be. Who are those in the longevity space taking rapa + SGLT? (Attia? Anyone else?)
1 Like
Very helpful - as usual @adssx
@Davin8r you might find the above helpful in context of your post that I quoted just above it.
2 Likes
I’ve been thinking of perhaps cycling between them
Rapa (and acarbose) in spring and summer, when I also focus more of resistance training than cardio and when risks of covid, colds, flu, pneumonia are generally smaller / and I’m more outside doing things
Come off of Rapa and onto SGLTi in the fall and winter, when my mTOR is less up given less resistance training and more focus on cardio and when extra good to have an optimized immune function
Any thoughts?
1 Like
That seems like the superior approach if you are going to use rapamycin. You do miss out on using a SGLT2i during spring and summer though.
1 Like
fingersticks aren’t the most accurate for calibration
i have two CGMs on right now and they do differ somewhat (will have more info in 5 days)
5 Likes
Wow two CGM’s at the same time…respect ![]()
1 Like
Canagliflozin (mixed SGLT1/2 inhibitor) did NOT prevent 18oz blueberries from spiking my BG briefly to 182… (this is the highest I’ve ever seen it)…
3 Likes