I will provide some summaries of the presentations with a few slide captures, over the coming week. My focus is on rapamycin and other high-impact and actionable approaches to longevity.
Targeting availability to consumers in the next few years…
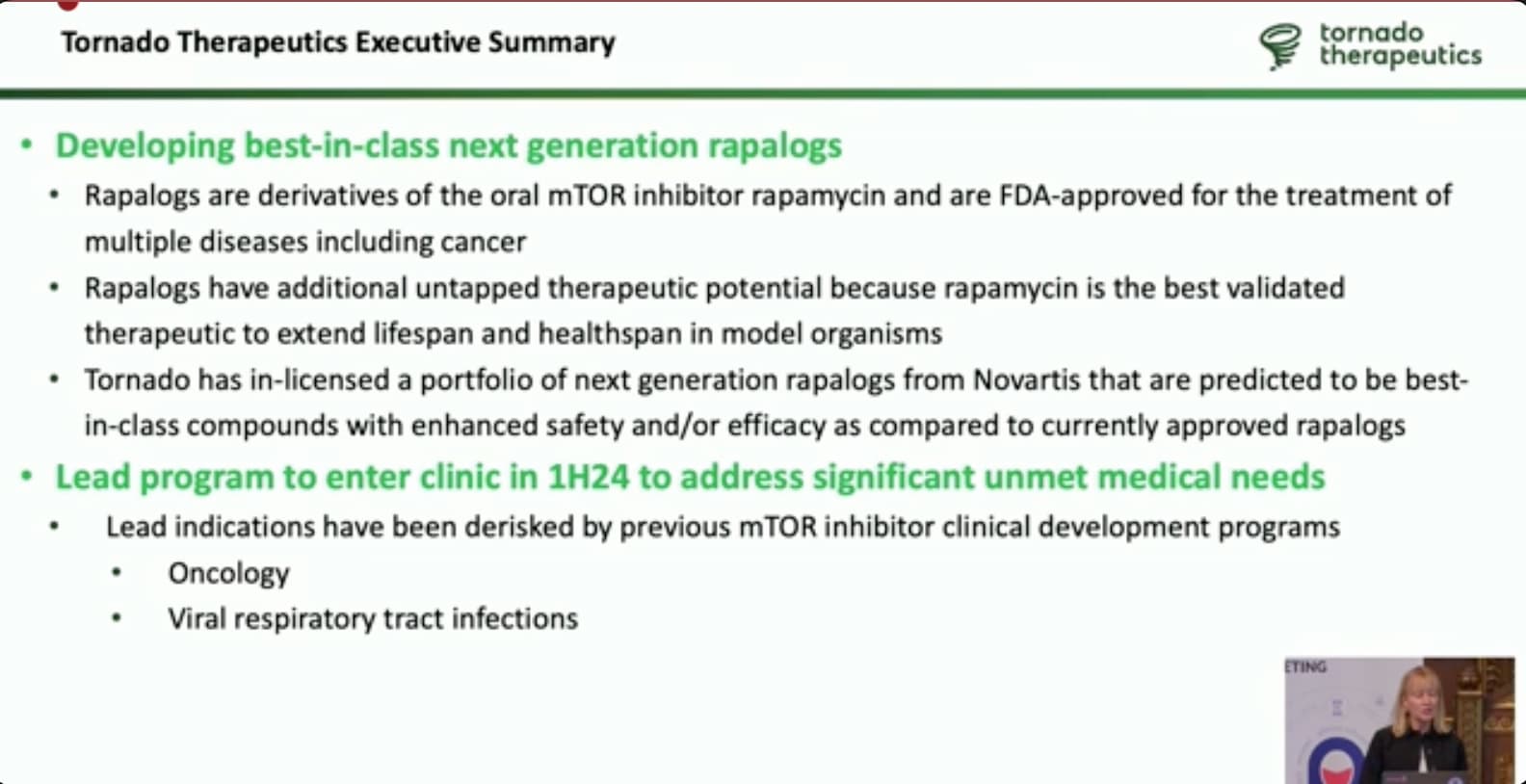
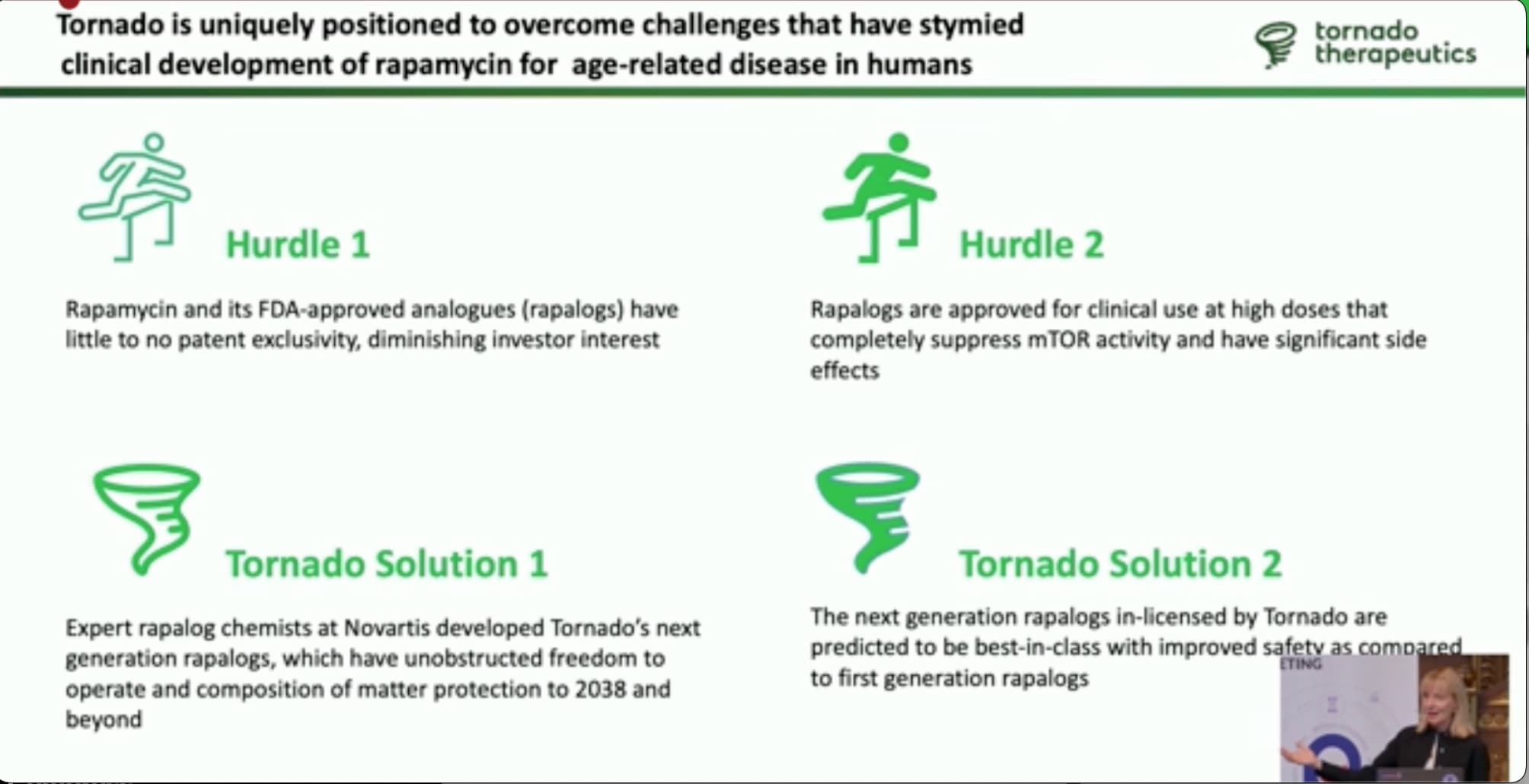
Tornado in-licensed a bunch of compounds from Novartis (because Novartis has decided not to pursue aging as a target at this time).
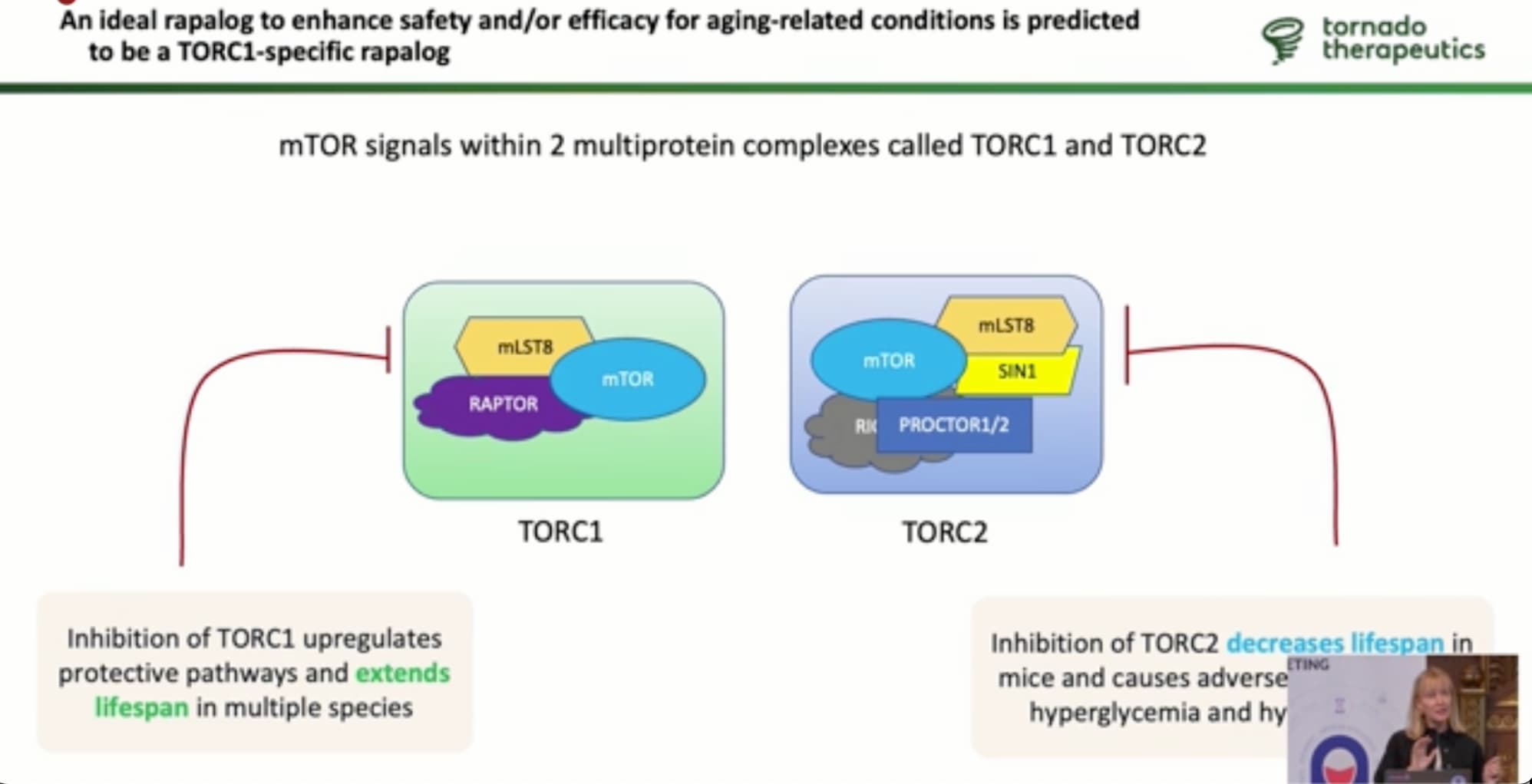
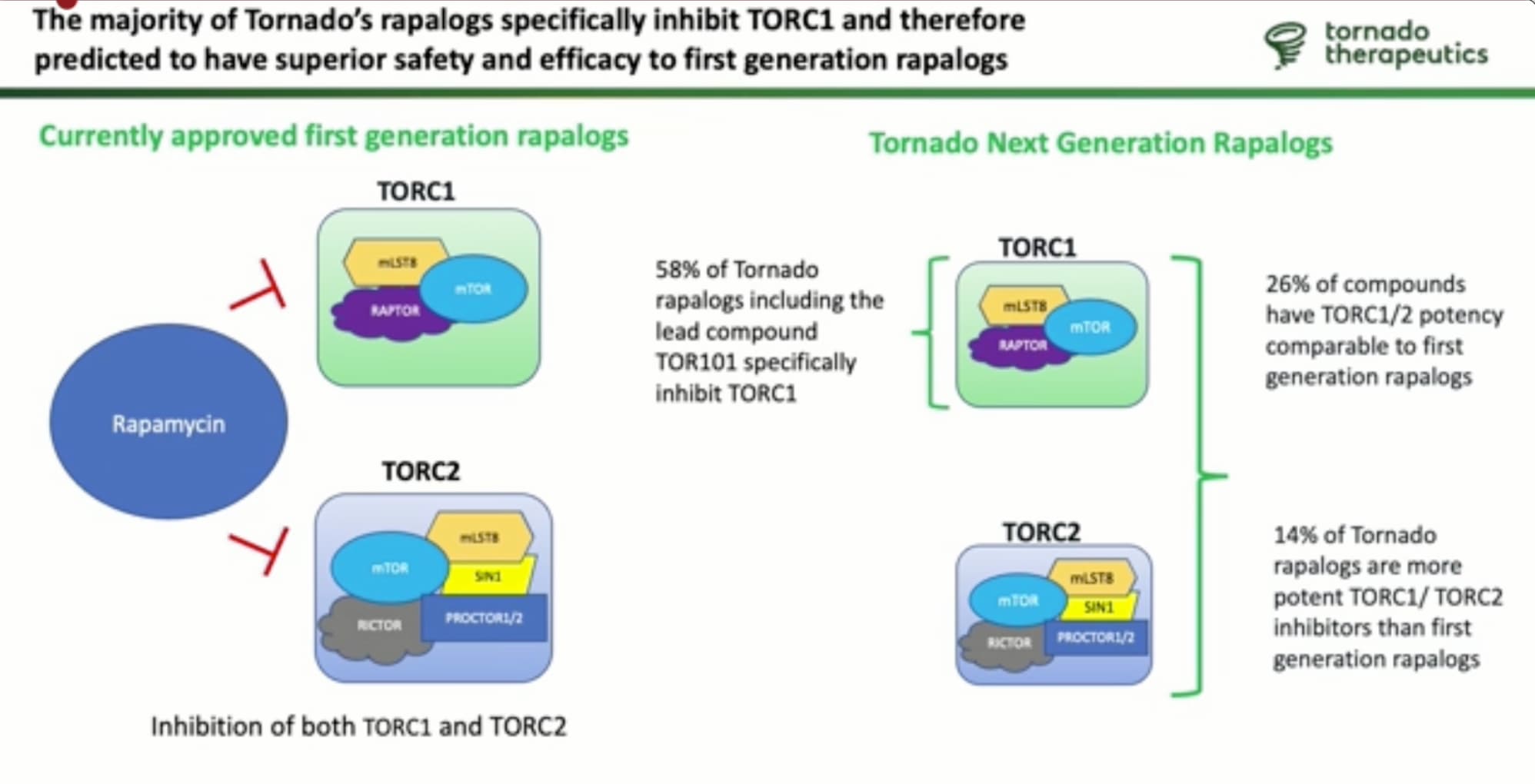
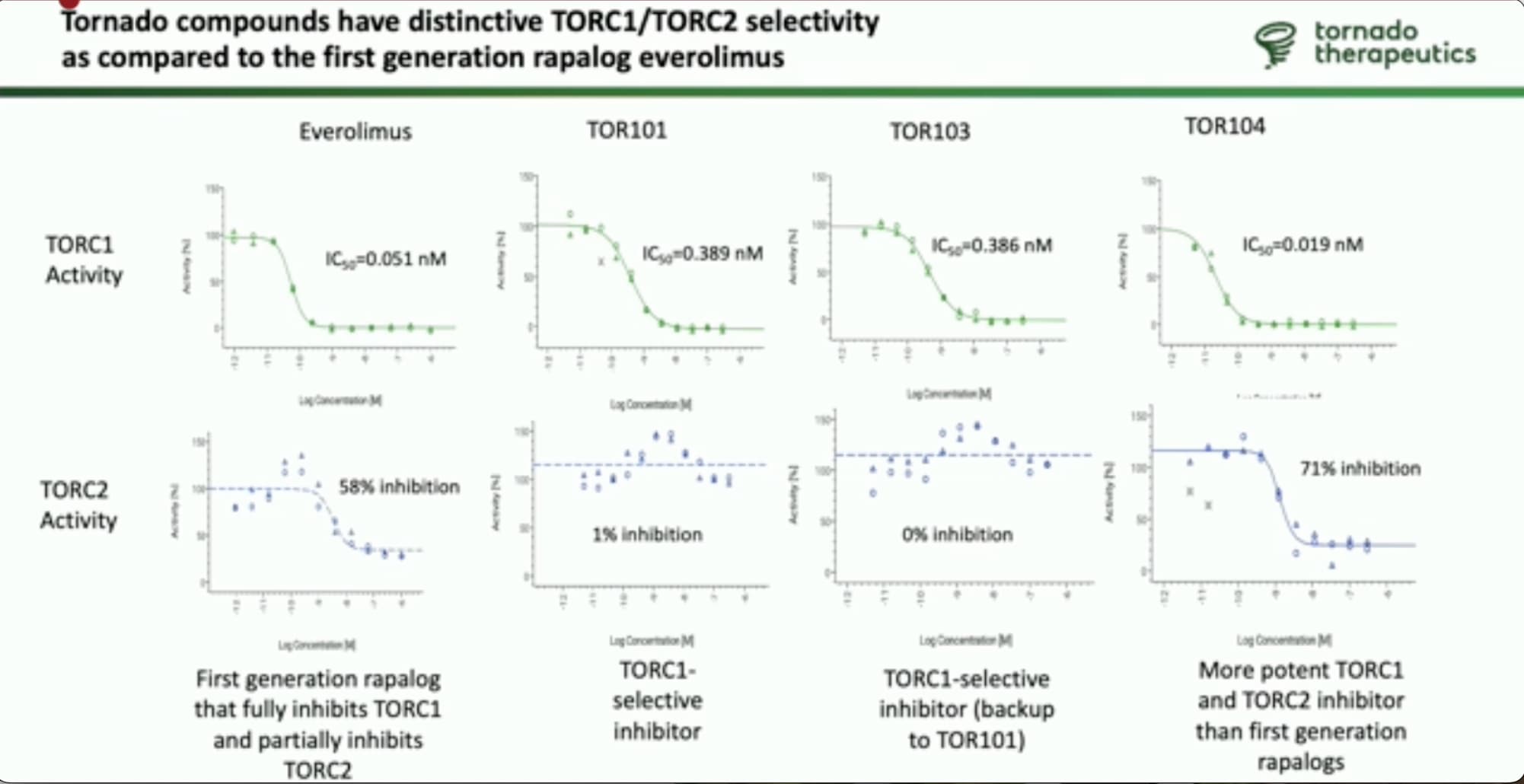
Lead compound is to enter the clinical trials next year… the endpoints being targeted; oncology/cancer and aging immune system. Their goal is to come out with an mTOR inhibitor that inhibits mTORC1 better, and mTORC2 at a much lower level than can happen with rapamycin (or a negligible level).
From the consumer perspective (i.e. longevity enthusiasts), the key issue will be the cost/benefit comparison of any new drugs from Tornado to rapamycin and everolimus. What is the marginal benefit compared to the marginal cost over existing generic mTOR inhbitors? Everolimus recently went off patent (in the past two years) and the price prior to going generic was in the $15,000 to $20,000 per month range. I believe prescription generic rapamycin (sirolimus) is in the $200 to $400 per month range, for a month’s supply.
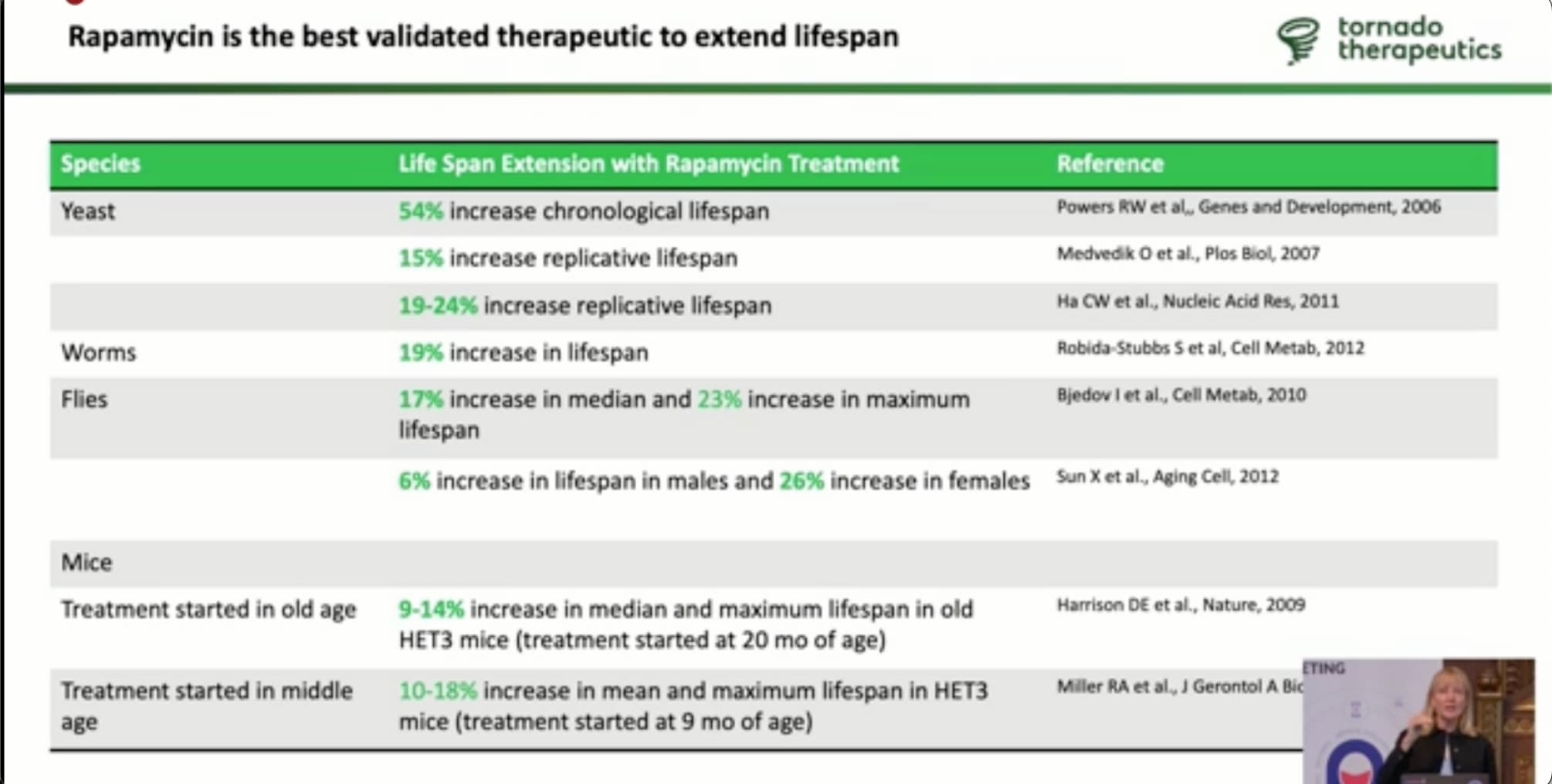
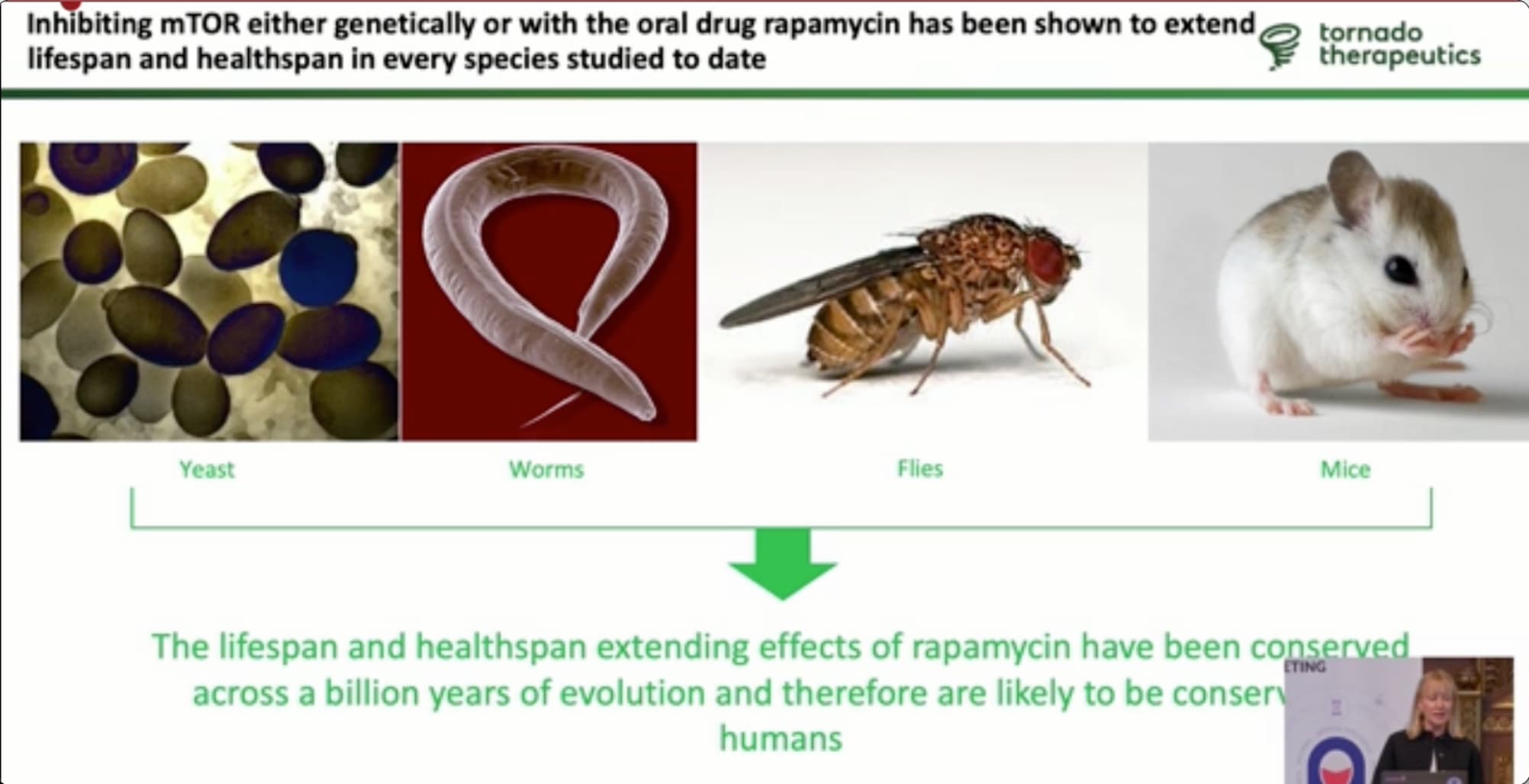
Most of the information below in the slide presentation is well known to fans of rapamycin:
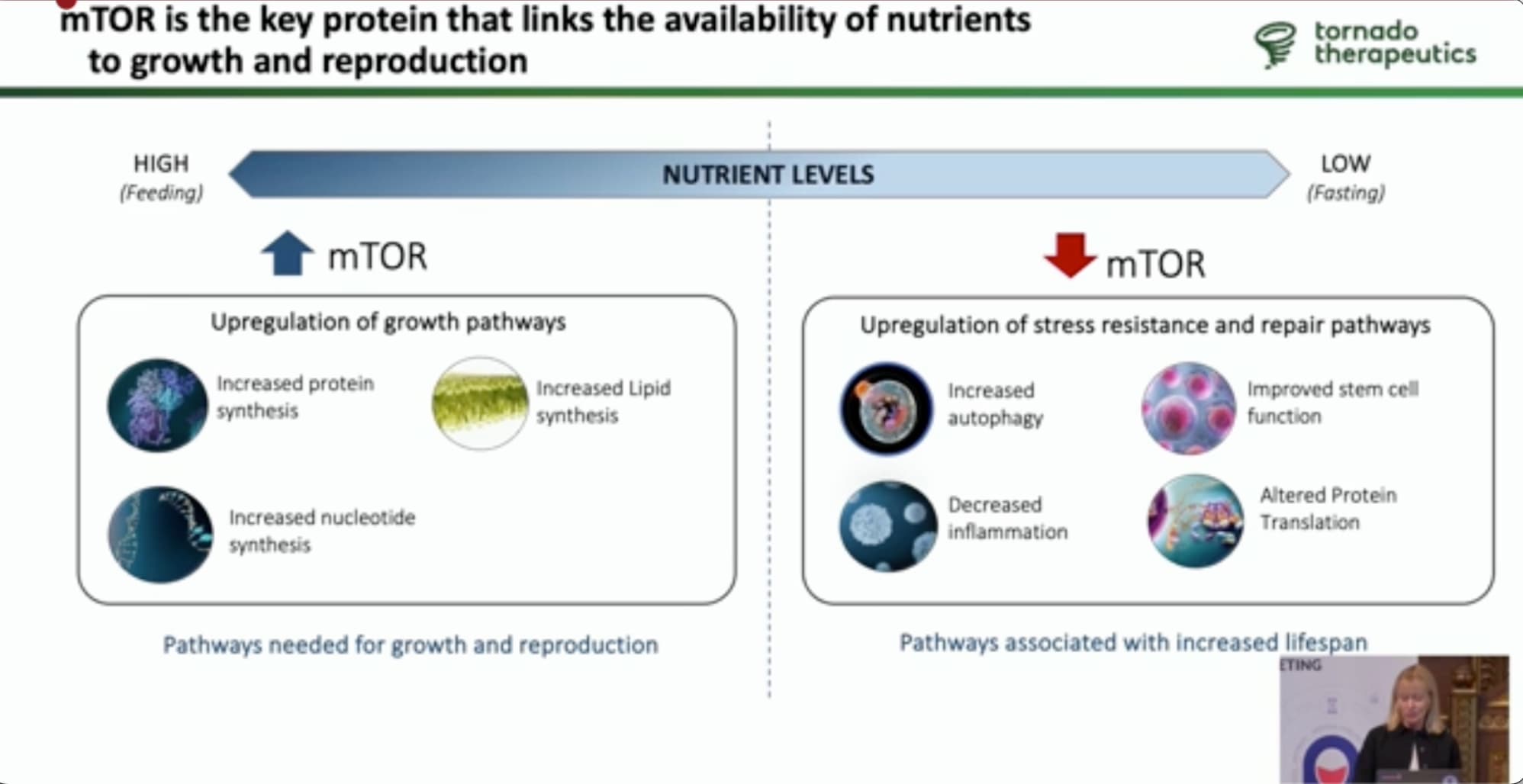
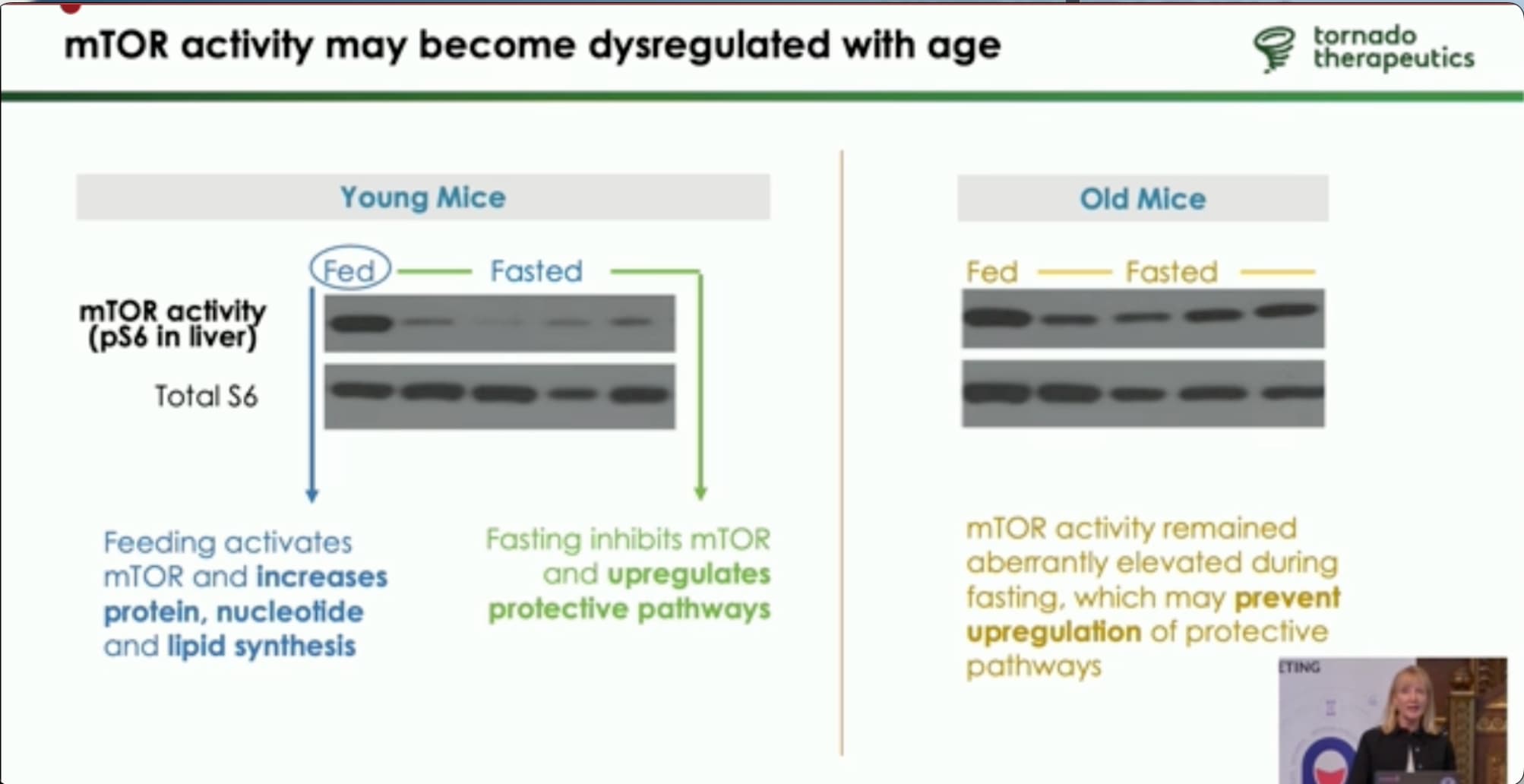
The key issue (that rapamycin, etc.) is addressing is that with increased age, mTOR gets activated most of the time in cells (i.e. becomes disregulated), which (in other sources I’ve read) people have compared to having the gas peddle on the car pressed down all the time, even when you don’t need to go fast. In young mice, mTOR is only activated when there is a good nutrient supply. in older mice mTOR becomes activated all the time, even when older mice are on a fast / nutrient deprived. Rapamycin acts as an mTOR inhibitor.
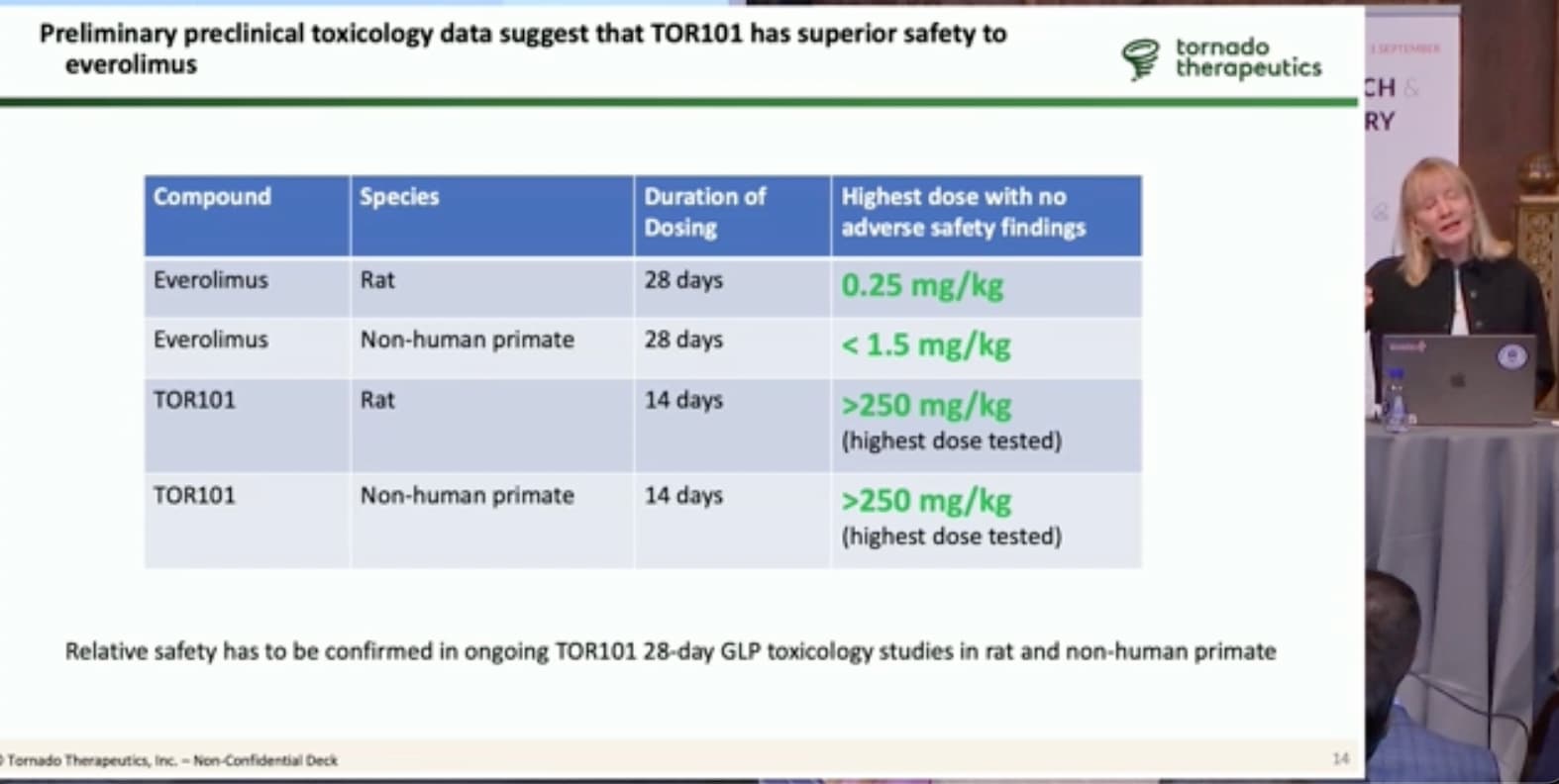
Joan says they are seeing very low toxicity with their new candidate molecule TOR101, as shown below with even very high dosing of 250mg/kg, so things are looking good.
I hope they are successful, as we need all the longevity drugs we can get. I’m just not optimistic that most people will be able to afford it, if and when it becomes available.