Ongoing… This is the issue with taking a lot of substances at the same time… I was taking a lot of grams of glycine during my experiment with higher acarbose rates which I believe, along with the acarbose and jardiance lowers glucose… I stopped taking glycine while still taking jardiance 25 and 600 mg of acarbose (300, twice daily with or without food), and wasnt near hypoglycemia. The one on the line hypoglycemic reading I got was jardiance 25, acarbose 700 a day (twice 350 with to without food) and a lot of grams of glycine with my coffee… I’m in limbo with whether or not I want to continue with glycine. If I stop taking it I will probably go even higher than the 600 daily (300 twice daily with or without food) acarbose, maybe towards 1000. If I continue with the glycine, I will probably stop at 600 (twice daily with or without food) acarbose with jardiance 25.
Maybe you’ve found some data on dose range for acarbose? I’ll admit I haven’t looked but there definitely will be an upper limit where you will not get any more serum glucose reduction as you increase the Acarbose dose. If I had to guess I’d think it would be down around 100-200 mg / meal.
Do you see a clear difference in glucose spikes between an acarbose dose of 100 /meal and a dose of 300 / meal? I guess if the meal is high in carbohydrates one might see an affect but then IMO a better approach would be to cut down on the carbs rather than take more acarbose.
Starting Aug 2024(the conversation), I think thats what was in the itp(?) tests equivalent human dosage. Around 800? I’m a big man a 200 pounds so I would take a bit more
I’m quoting this again despite being two months old but this is so helpful to see. It shows that 50mg per meal could be enough and that we don’t need veery big doses like the ITP used.
A good writeup summary on Acarbose:
Regarding Acarbose Dosing in Males
Most experts hold that acarbose’s glucose-modulating and longevity effects plateau around 100 mg per meal (≈ 300 mg per day).
However, a closer look at the Interventions Testing Program (ITP) data suggests that this “plateau” may simply reflect the limits of statistical sensitivity rather than true biological saturation.
Across all tested doses, the p-values for lifespan benefit in males were already at the extreme lower limit of significance (< 0.0001), meaning the study design could not resolve finer gradations in benefit. Greater precision in variables such as food intake, acarbose concentration, or body-weight normalization might reveal additional separation at the sixth or seventh decimal place.
| Dose (ppm) | Female p | Male p |
|---|---|---|
| 400 | 0.033 | < 0.0001 |
| 1000 | 0.0027 | < 0.0001 |
| 2500 | 0.0061 | < 0.0001 |
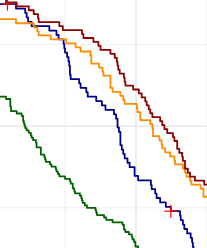
Looking directly at the survival curves, the male cohorts between roughly day 350 and 1075 show a clear outward “bulge,” indicating longer survival with increasing dose—the low-dose (blue) line having the smallest bulge and the 1000 ppm and 2500 ppm groups visibly higher.
Comparable “bulges” in other ITP lifespan plots, when quantified, have been statistically significant; for example, in female 1000 ppm ACA, overall survival improvement reached p = 0.0048 .
Thus, although formal statistics report no additional p-value improvement beyond < 0.0001, visual and comparative evidence strongly implies a dose-response relationship that continues beyond the nominal 300 mg/day human equivalent.
In other words, imho, the higher-dose effect is real—it simply exceeds the sensitivity of the ITP’s original analytic framework.
Acarbose 1000 mg dosing (males & females)
Just eyeballing it, the orange and the red higher doses, clearly beat the blue and the green.
I’m still pondering the shape of the survival curves. Bouncing it off AI I get:
The ITP’s official stats (log-rank tests) look at the entire survival curve, so a drug like acarbose can score very strong p-values by shifting the bulk of the population out to older ages. But if you look instead at a simple tail metric — e.g., ‘how many treated mice are still alive at the age when the last control dies’ — acarbose alone doesn’t look nearly as dramatic: only a few percent of ACA-treated males are still alive at that point. In contrast, rapamycin (and especially rapamycin + acarbose) leaves a much larger fraction of animals alive when all the controls are gone — often in the 10–20% range. In other words: acarbose is great for median lifespan; rapa (and rapa+ACA) hit the far right tail much harder.
And talking about curves — looking at the Rapa + Acarbose survival curve (MPD: ITP survival analysis: rapamycin and acarbose)
— they’re truly a thing of beauty, put Marilyn Monroe to shame:)
Yes, I view Acarbose as a Rapamycin enhancer and not so much as a standalone treatment. I also feel like you could swap Acarbose with either an SGLT2I or Metformin and get similar results.
Based on what I’ve read, I’m guessing the optimal combination would be Rapamycin, an SGLT2I and Acarbose.
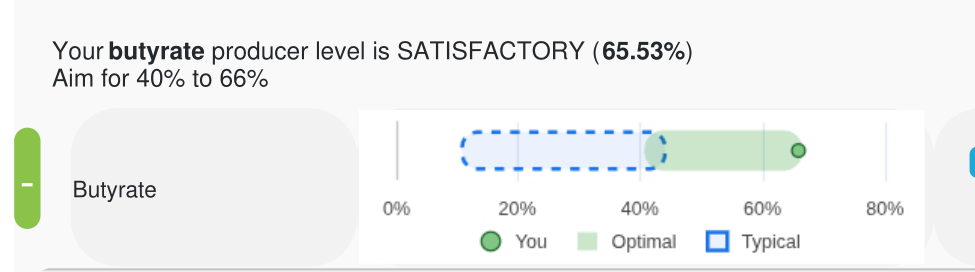
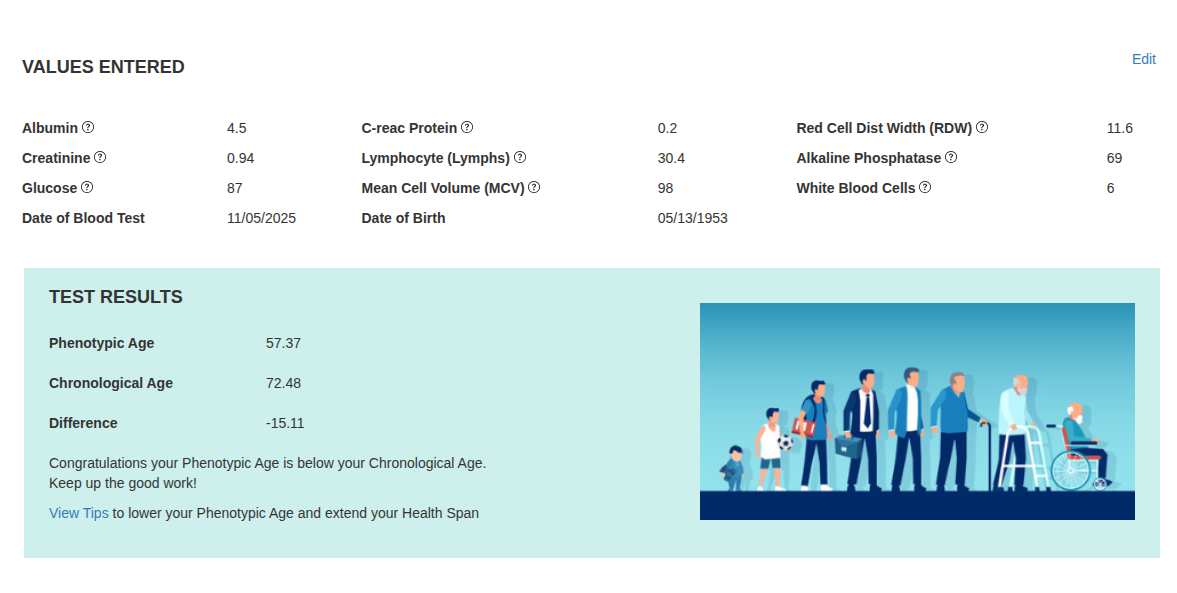
My biome results came back after high dose acarbose and high intake of potato starch (150 grams a day) for a couple of months. At first glance it looks like a “win” on the two main “fronts”. I wanted to increase SCFA production and as a secondary measure check my Levine Age Score. SCFA came back as a clear win, essentially maxxed out, total victory.
My Levine Score didn’t come back too shabby either. About a year ago I was running negative 12-14 years, latest is closer to negative 15. There are alot of confounding variables, so its good news, but not probative.
NovBlood2025blacked2.pdf (2.8 MB)
With a little help from AI an observation: The most obvious change in my routine—even more than the acarbose—has been the sheer volume of potato starch I’m running: approximately 150 grams a day, split across my two meals (each paired with acarbose). Raw potato starch is mostly resistant starch (RS2), meaning it behaves like a ghost calorie: ~600 calories on paper, but the colon microbes actually get first dibs. Depending on the person, only ~0–60 calories make it to me; the rest ends up as butyrate/propionate/acetate (SCFAs). With the acarbose blocking a chunk of digestible starch, even more carbohydrate gets “caught” and delivered downstream, so you end up turbo-charging fermentation. Net effect: fewer human calories, more microbial calories, and yes—the gas is a feature, not a bug.
A further caveat: My gas production is notable, even epic. It would be totally unacceptable if I was working in an office setting. It is many times my previous level even when on a largely bean diet. I believe most people would find it unacceptable. When I get to the gym and I start any exercise involving the core/abdomen my gut senses it and I always have gas shortly before I start the move. I am just a rude grumpy old man and don’t really give a shyte, but its actually embasses even me and so I try to pass the gas while I’m walking quickly to the core/abdomen machine to “spread it out”. Gross I know, but its a real thing and people should be fore-warned.
I’d rather not. What about taking simethicone with it to reduce gas?
Also why is your hematocrit so low?
I have a large bottle. I think it mainly just works in the stomach. It does nothing for bowel gas, at least not for me.
I’ve never felt good on acarbose. Does it get easier with time?
Yes, I learned to avoid most wheat products, however pasta doesn’t seem to bother me that much.
Those heme blood markers have been low for several years. I tried B12, iron, all the normal supplements, no movement. PCP not worried about it, no external symptoms (fatigue) so no “treatment plan” just watch and wait.
As to Simethicone it “works as an antifoaming agent by reducing the surface tension of gas bubbles in the gastrointestinal (GI) tract, allowing smaller bubbles to coalesce into larger ones that are easier to expel through belching or flatulence.” My gut has adapted or learned how to handle the gas fairly well, so the “bubbles” of gas are coalescing well and those larger bubbles are slipping past the stool nicely without causing “leakage”. It took me a week or so to get past the leakage stage, also I bought some psycillium capsules and I take 3 with my one “oily” meal of the day, So it seems my stool consistency is good throughout both large and small intestine, and I think that is important for properly coalescing to avoid “explusion” problems. And gas is actually a minor problem in comparison to “expulsion”.
My God I feel like I’d need to live alone in a cabin in the woods to adjust to acarbose ![]() .
.
I’ve got like 100-200 tablets, I took it once or twice and said “nope”. Oh well maybe in the future I’ll try it out. Empagliflozin seems to be similar, you pee out sugar calories (compared to blocking starch digestion). Doesn’t have as annoying a side effect profile.
I get it. I’m old and alone, except for my wife, and isolated (except for the gym) and most people aren’t in that position. My wife is naturally more forgiving, but I tried her patience and olfactory tolerance a number of times. As long as I do my best to walk into the next room before I cut loose, she’s ok with it.
My potato starch came this morning. For those who don’t know grams, 150 gm is about a cup. That’s a lot. I did a Tbs this morning. And I don’t know what the acarbose will do for that at all. It’s nearly all resistant anyway. I just take it when I’m having a meal with family and we have root veg. or something. Maybe 50 3 times a week.
It seemed to me that before having the RS I should trim my gut buddies and get rid of the bad guys, that’s why the XOS for a week or so. Otherwise it’s like fertilizing the lawn when it’s full of weeds. The weeds appreciate it but going in the other order seems like it works a little better.
I’d never run across XOS before but it looks promising so I’ll try some. My butyrate produceers were great but lactate and acetate producers were in the middle range so hopefully it will give them a boost. Oh with the potato starch I put it in a water bottle and then I have to shake the bottle everytime before I take a drink. I think you’re right that it is mainly RS anyway but I’ve read different numbers for the percent digestable from 25% to 50%. I use the unmodified raw potato starch so that probably tends to have a lessor amount of digestable starch.
Take 10-20 mg (cut tablets whatever) at the start of a meal and limit rice, wheat, heavy carbs in the meal. Work up slowly. I felt seriously ill when I first started acarbose but now don’t notice any symptoms with taking 100mg prior to every meal. Even meals containing white rice etc. You need to start slowly, adjust your dose, and adjust your diet and give your gut a chance to reconfigure.