I have eczema so my needs is low dose keep mTorc1 less active.
It just worked for me better over time. Doxy is based on research like this and it is a bit of insurance policy: https://www.sciencedirect.com/science/article/pii/S2666354624001728
Beth – Those are very good metrics. Given the complexity and your personal goals, you are obviously doing a great job. I think we may share a challenge. I am trying to simplify my protocols in a systematic evidence-based way. If you do all of the research, it can be a daunting task. Recently, I found that I was making more progress by organizing the supplements I take (including self-prescribed pharma) by health target. For example, I have the relatively common BHMT-08 homozygous polymorphism which is easily addressed via a supplement stack of Phosphatidylcholine, TMG (very low dose, contra common belief), 5-MTHF, Methyl-B12, B6, Creatine, and Mg Glycinate. You can see that some of these supplements can be valuable in relation to other health targets. Thus begins the matrix. Creating a comprehensive supplement matrix across targets in a way that accommodates not only shared purposes but addresses time of day, frequency, with or without food, and contraindications – all while seeking simplification – is where the fun comes into play. I’m enjoying the process and accept that it may take awhile.
3 Likes
General health:
- MicroVitamin by Dr Stanfield
- Plant-based protein powder 30g
- Creatine HCL 5g
- L-Ergothioneine 25mg
Cardiovascular health:
- Pitavastatin 1mg
- Omega 3 EPA-only 1g
- Retatrutide 6mg
Kidney health:
- Empagliflozin 6.25mg
Better Sleep:
- Sleep by Dr Stanfield
- Amitriptyline 25mg
Stomach health:
- Boulardii
- Psyllium husk 6g
Penile health:
- 2.5mg tadalafil
- 6g L-Citrulline
Eye health:
- Astaxanthin 12-24mg
- Lutein 10mg + Zeaxanthin 4mg
Skin health:
- Sunscreen UV50
- Tretinoin 0.05%
- Collagen peptides 12g
Hair (and prostate) health:
- Finasteride 1mg
- Minoxidil 5%
- Ketoconazole shampoo once weekly
5 Likes
@RobTuck
Thanks. Learning your approach is helpful and gives me something to try to wrap my head around to help me further fine tune my ‘mess’. Today was the first day I attempted to list what I take by my goals and I see it does help clarify things. I’ll pm you to ask you more about how you manage the list in regards to the same thing helping various goals.
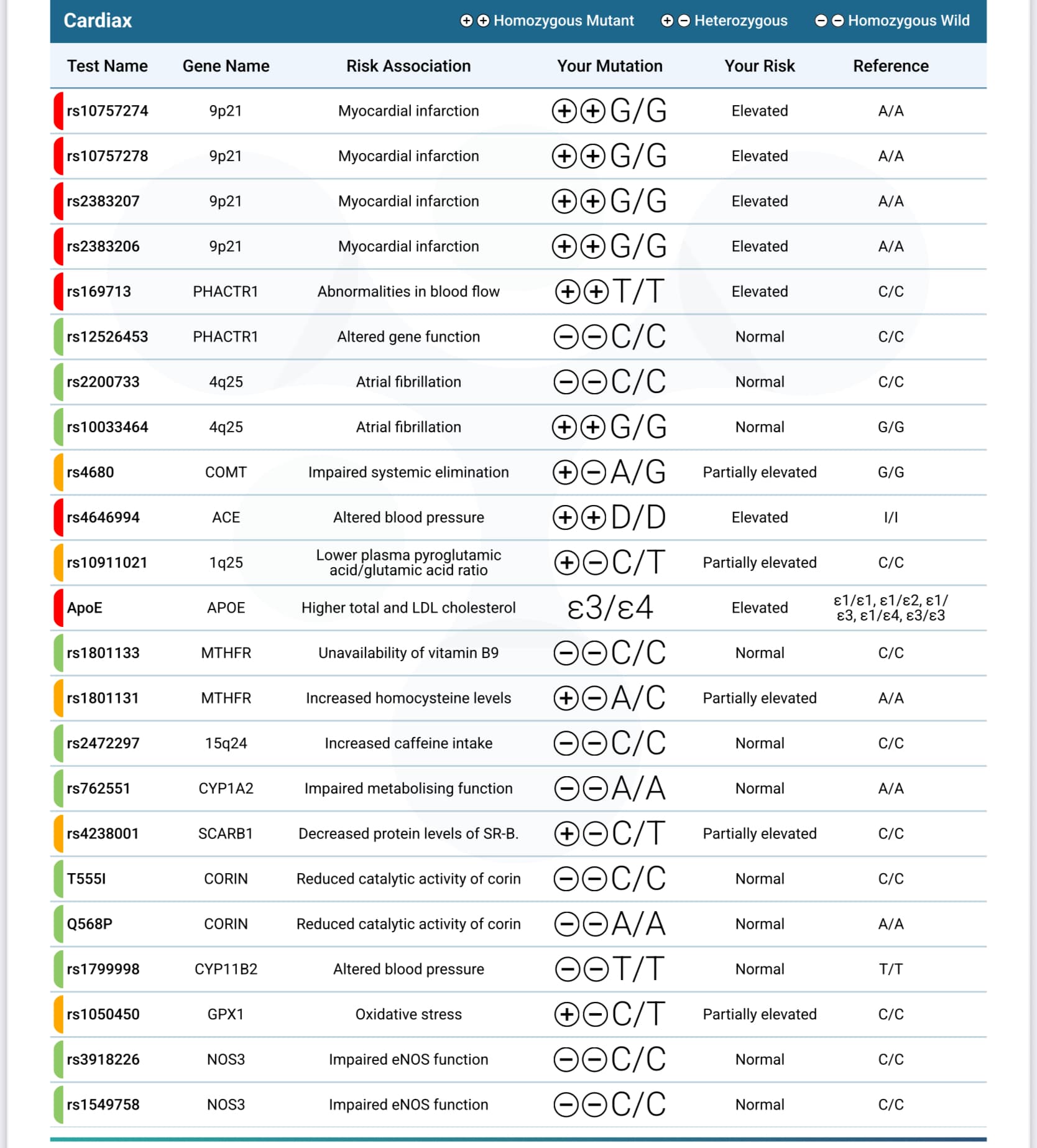
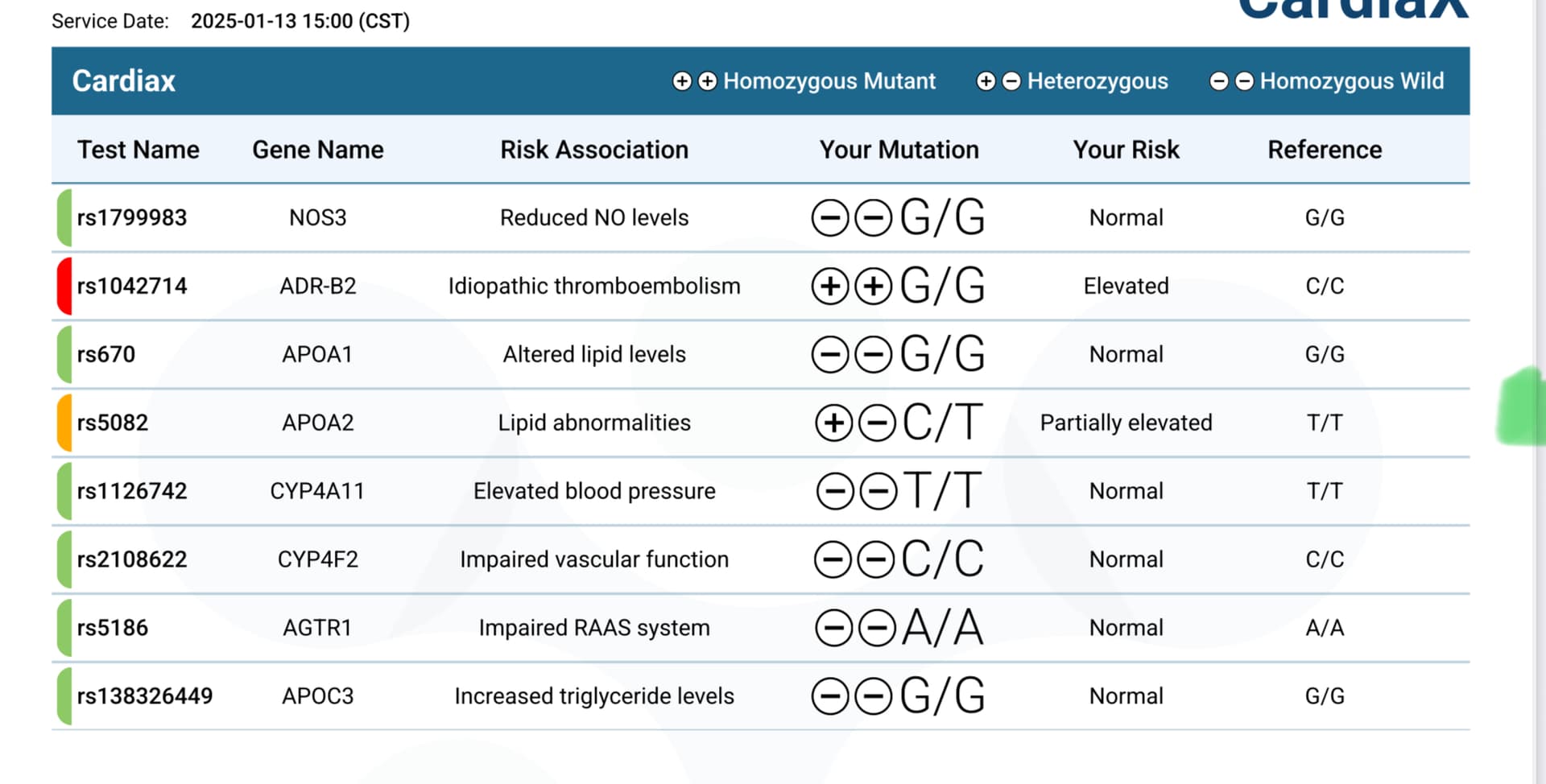
This is the sort of thing that is way over my head. Ages ago I learned I had the MTHR gene, and I see a lot of you talk about methylation, but it’s just something I have not understood or learned about yet.
Last year I did take the cardiax test that talks about some of this, but it’s all Greek to me. Just to be OTT, I”ll include those results here.
1 Like
Do you use this for joint pain? If you look it up, long term use isn’t recommended because of its effect on the stomach and kidneys
1 Like
Tons. I’m on my phone atm, bit I’ve written about that many times, citing studies.
Well those are Grok’s words but there are A LOT of studies showing NR boosts NAD levels. Are you specifically saying it doesn’t boost NAD+ at the tissue level?
This is why I take it. The effect on joint pain is a nice bonus though. It was shown to have the greatest reduction in all cause mortality at double the dose I am taking. I don’t think it is harming my kidneys because my Cystatin C was recently 0.64
https://onlinelibrary.wiley.com/doi/10.1111/acel.14334
Abstract
Although most drugs currently approved are meant to treat specific diseases or symptoms, it has been hypothesized that some might bear a beneficial effect on lifespan in healthy older individuals, outside of their specific disease indication. Such drugs include, among others, metformin, SGLT2 inhibitors and rapamycin. Since 2006, the UK biobank has recorded prescription medication and mortality data for over 500′000 participants, aged between 40 and 70 years old. In this work, we examined the impact of the top 406 prescribed medications on overall mortality rates within the general population of the UK. As expected, most drugs were linked to a shorter lifespan, likely due to the life-limiting nature of the diseases they are prescribed to treat. Importantly, a few drugs were associated with increased lifespans, including notably Sildenafil, Atorvastatin, Naproxen and Estradiol. These retrospective results warrant further investigation in randomized controlled trials.
2 Likes
Is Naproxen same as Aleve?
Yea Aleve is just the brand name
1 Like
Testosterone for women (and men) is particularly good for muscle mass and bone strength. The main downsides are potential androgenic effects - hair growth, acne, deeper voice. At female dosing, there isn’t much serious downside. If anything, it would be CV risk but probably minimal.
Other positives are energy level, positive outlook, libido, etc.
Having looked at this for my wife for awhile, I think most post-menopausal women should be on what I term triple therapy - estrogen patch, progesterone pill at night and testosterone cream. Dosing mostly by symptoms but check testosterone levels to avoid going too high. I had a female patient with a 500 testosterone level from pellets. She had no downside but that is nuts. She reported anger issues only when she was low on T strangely enough. No voice changes either. She was 65 with a 50 year old husband …
Overall T is probably more health span than lifespan but fraility and broken hips kill so I think lifespan is likely improved also.
Now, there isn’t going to be any data particularly with starting later. With Estrogen, the thinking by many is that you shouldn’t start over 60 years old I believe.
Lastly, most studies demonstrate neuroprotective action particularly in cell cultures (of questionable relevance). But also in mouse models and some human disease states.
6 Likes
Jonas So, the doxycycline with the rapamycin has nothing to do with the combination of the two. It’s purpose is specifically for Alzheimer’s prevention. Or, did I misunderstand?
1 Like
How is this going? I’ve got some and I’ve been tempted to start trying it out.
In my case I moved over to pitvastatin for its lower impact on insulin resistance. My LDL-C is down in the 40 range now, and so my priority is my slightly raised blood sugar levels: What's the best statin to take? - #51 by vishnu
4 Likes
These supplements may increase blood levels, and perhaps extracellular matrix levels, but the real question is do they increase intracellular NAD+ levels which is where an increased concentration of NAD+ could benefit us.
I haven’t seen any studies that suggest an increase in intracellular NAD+ levels. If you can reference, I’d be happy to take a look, but failing that, I regard these expensive supplements as a waste of money.
I would try Niacin instead of NMN or NR to raise NAD+ levels: NAD+ Reality Check: Can We Bottle Youth? - #2 by RapAdmin
Related:
3 Likes
I don’t take them either. I was just pointing out that they probably don’t deplete methyl groups.
1 Like
Your stack is whatever you want to take, but it’s not based on the latest science.
1 Like
What kind of Magnesium?
I use Magnesium L-threonate at night, Glycine in the morning, Malate if I am playing sports.
@KarlT I would love it if you could share your stack?
Any of my stack is non-sense that you want to tear up? I would welcome that. I am purposely stay “lean” for the time being and then add back some perhaps over time.
One thing I am adding this year is to use some of DORA sleeping medications to aid my maintenance sleep (Dayvigo 5mg) and better clearance of brain sewage at night. This is very recently discussed by Matt Walker (the sleep doc) and used by Tim Ferris etc.
On Doxy, it’s just I also have rosacea now and then so it’s part of insurance for a variety thing with me personally. I believe Peter Diamandis proposed Rapamycin with Doxy at one point.
I use it 100x twice a week as it is a dose that is not likely alter my gut bacteria.
Some of Gemini cited research on Doxy:
Key Researchers, Studies & Protocols
- Dr. Johan Auwerx (2013/2022) | The Worm Longevity Model: Auwerx’s lab at EPFL established the foundational theory of “Mito-hormesis” by showing that doxycycline extends C. elegans lifespan by up to 70%. By mildly inhibiting mitochondrial ribosomes, the drug triggers a survival response called the Mitochondrial Unfolded Protein Response ($UPR^{mt}$), which effectively “tunes up” cellular repair mechanisms and reduces the accumulation of aging pigments like lipofuscin.
- Dr. Baohua Liu (2024) | The Mammalian Breakthrough: Published in PubMed in 2024, Liu’s research moved the needle from worms to mammals by proving that doxycycline treatment extends the lifespan and rescues the physical decline in Progeria (accelerated aging) mice. The study highlighted that the drug works by suppressing IL-6 (a master cytokine of “inflammaging”) and preventing the breakdown of the nuclear envelope, a hallmark of cellular aging in humans.
- Dr. Michael Lisanti (2019/2023) | The DAV Protocol: A pioneer in cancer metabolism, Lisanti developed the DAV Protocol (Doxycycline + Azithromycin + Vitamin C) specifically to target Cancer Stem Cells (CSCs). His research demonstrates that this triple combination “starves” the mitochondria of senescent and cancerous cells, preventing them from replicating and driving the metabolic decline that often accompanies advanced age.
- Dr. David Sinclair / Life Biosciences (2025-2026) | The Epigenetic Remote Control: In a shift from using the drug as a supplement, Sinclair uses doxycycline as a molecular “on-switch” for gene therapy. In his current “rejuvenation” trials, patients receive a viral delivery of Yamanaka factors (OSK) that remain dormant until the patient takes a course of oral doxycycline, which activates the “cellular reset” to turn old, injured cells back into a younger state.
- Jane McLelland & The Metabolic Community: As the author of How to Starve Cancer, McLelland has popularized the use of doxycycline as a Matrix Metalloproteinase (MMP) inhibitor. Biohackers in this niche use low-dose doxycycline to block the enzymes that degrade the extracellular matrix, aiming to preserve skin elasticity and prevent the systemic “leakiness” of tissues that occurs with age.