@JazzMann, thank you! I really appreciate your thoughtful comments. I’ll be very thorough in my reply because you took your time to offer me some great advice and you asked good questions. The bonus is arranging everything like this also helps me in this puzzle.
You mentioned the potential risk of unexpected or undesirable interactions. I actually don’t know what those are, so I’d love to hear what you think I should look out for. And thanks, while I do try to learn by being active on here, I admittedly only know enough to be dangerous.
On minimizing my stack and living a healthy lifestyle… this is where it becomes a bit of a quandary for me. Until I started down the longevity path almost two years ago, I did all the right things, including having a freakishly healthy diet and even doing Prolon once a quarter for several years, but I still felt MEH pretty much all of the time. I was constantly going to doctors and having a million tests done to figure out why I never felt well, but there were never any answers. I just figured that was my lot in life. Then I started rapa (and all this other stuff) and I feel better than I have in over 20 years, so I’ve been rewarded for turning my body into a pharmacy  … and I realize what has made me feel great could ultimately be my downfall… rewarded for continually adding things…
… and I realize what has made me feel great could ultimately be my downfall… rewarded for continually adding things…
I’m sure some of what I take is not helping, but my issue is I don’t know which of these things have less value. I also have some crappy genes I’m trying to outrun. I’m not trying to defend my too long stack because I do believe it’s too long, but I’m only explaining why just a great lifestyle has been shown not to work for me. I remain very open to any advice or critiques
I had horrible insomnia for decades, and as I’ve shared elsewhere, rapa flipped a switch for me. I personally don’t understand it all, but I remember @John_Hemming commented it could be from rapa helping my mitochondria. I took that idea and ran with it, and now any time I hear something is good for my mitochondria, I say gimme some.
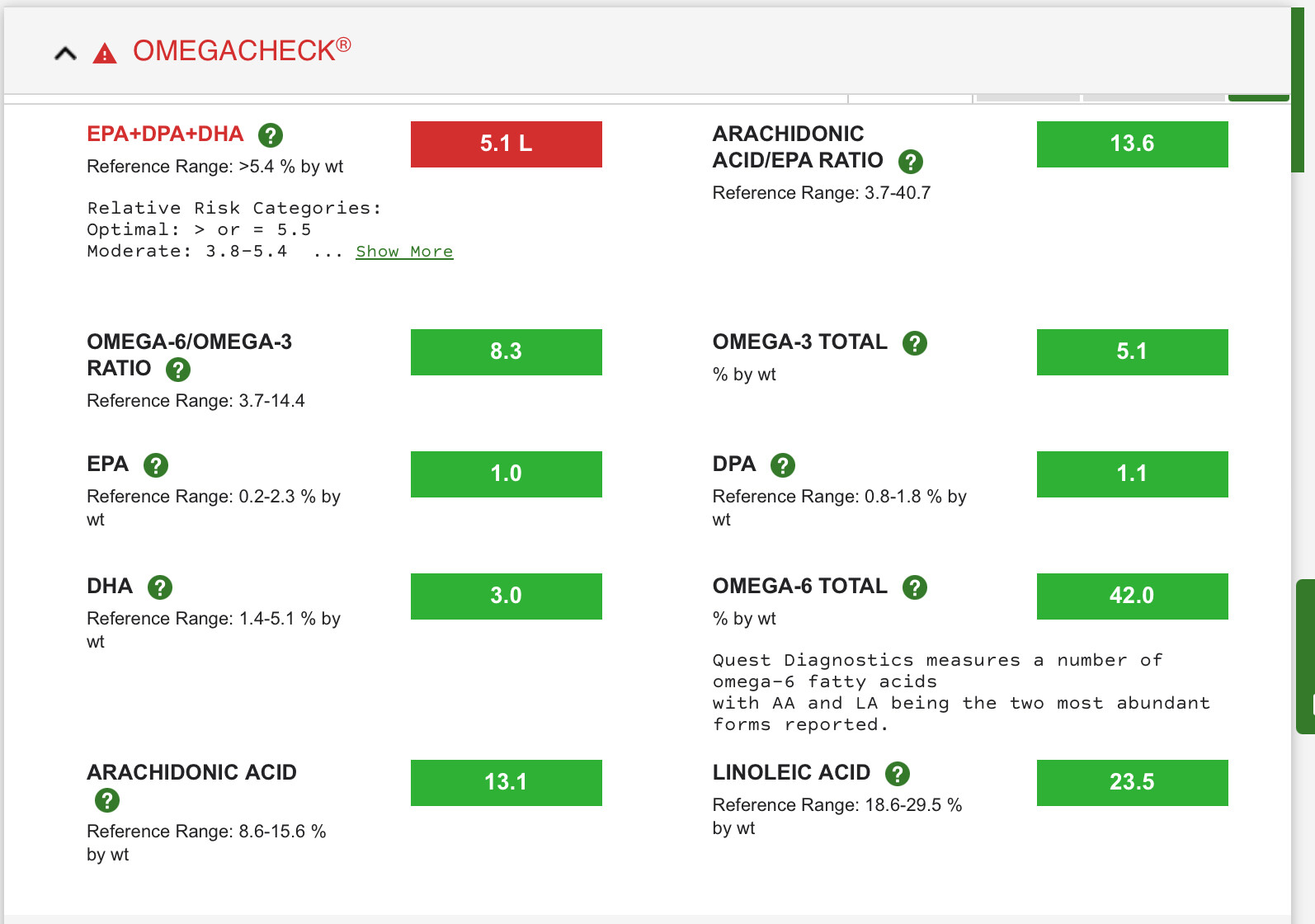
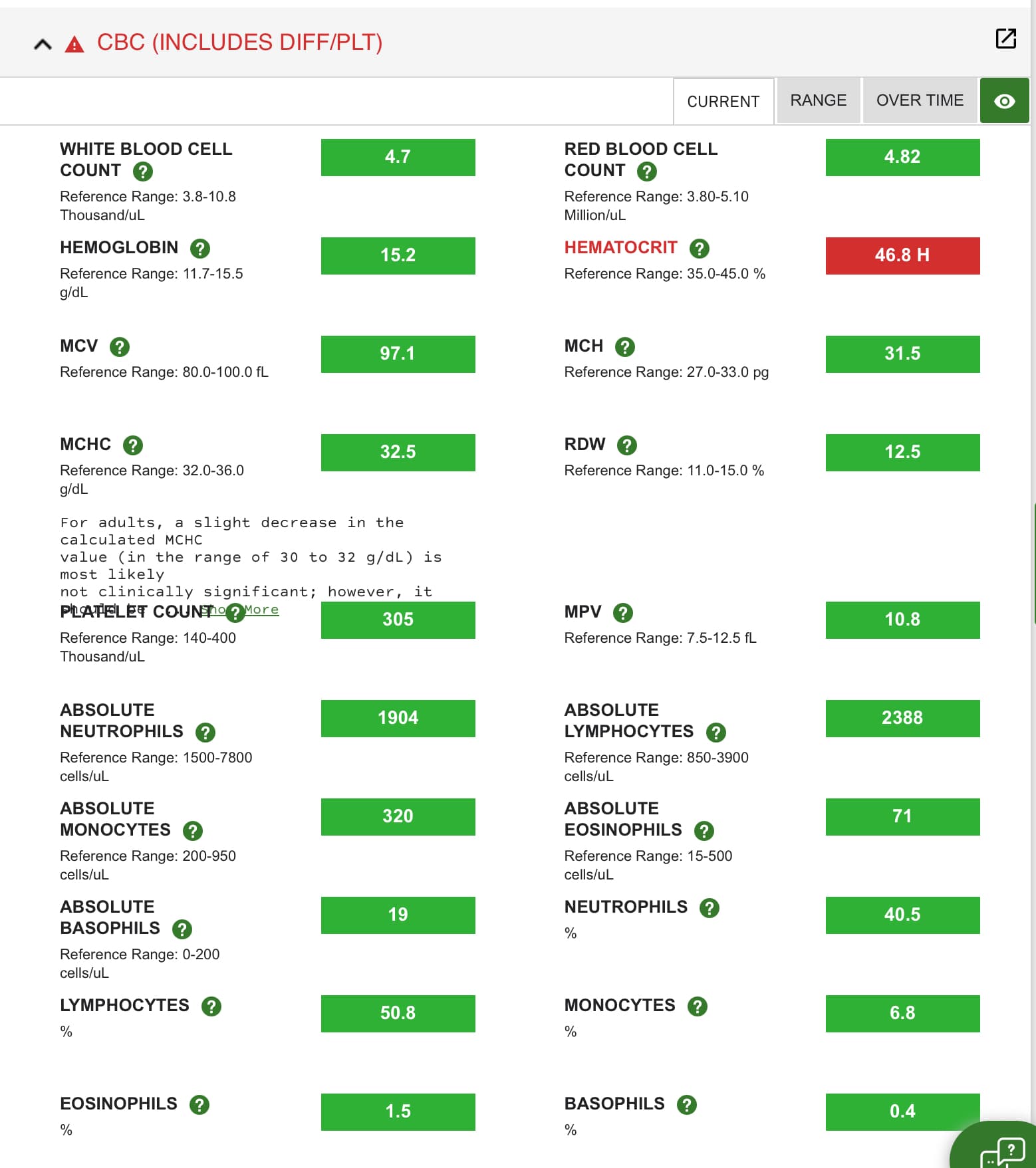
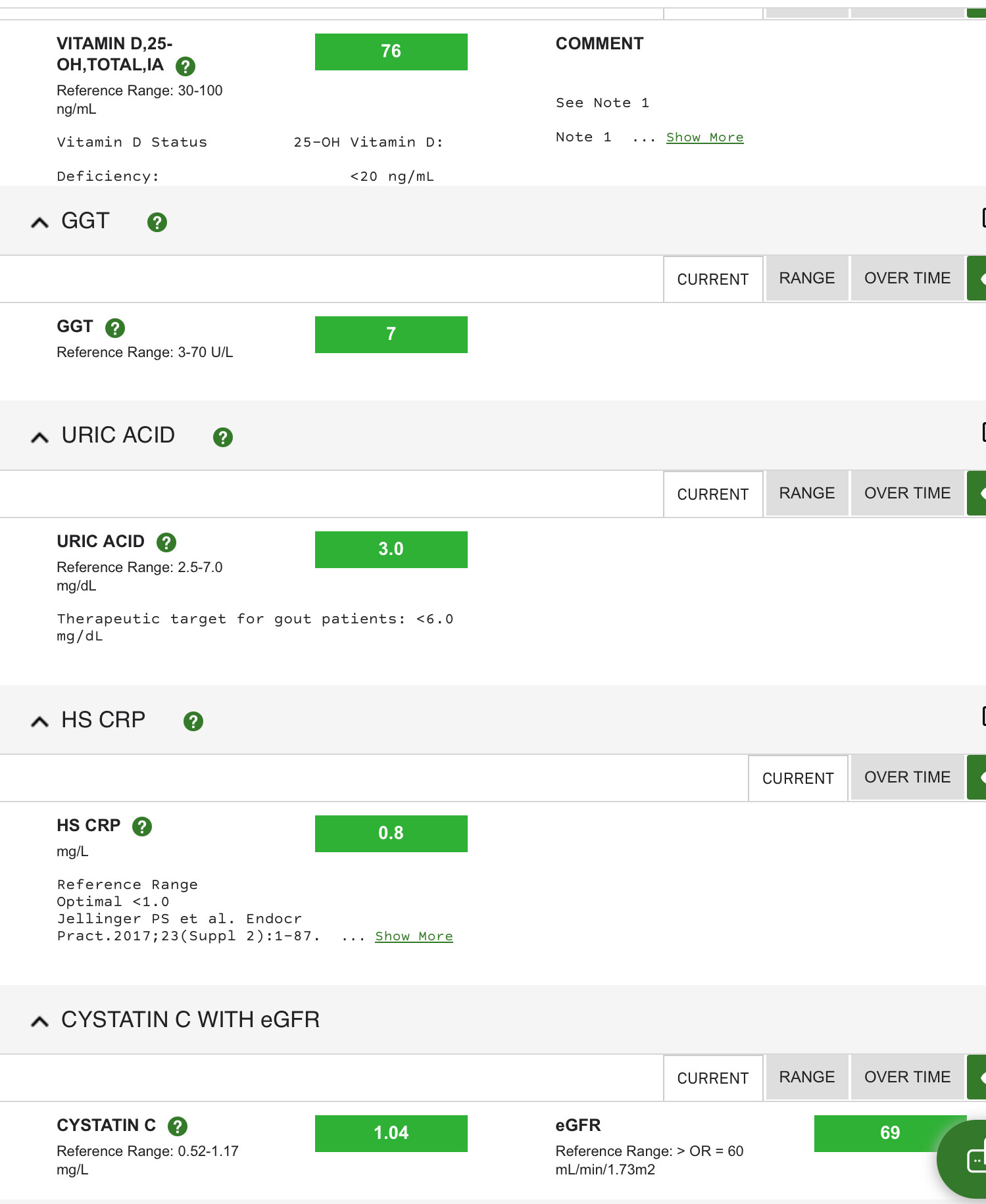
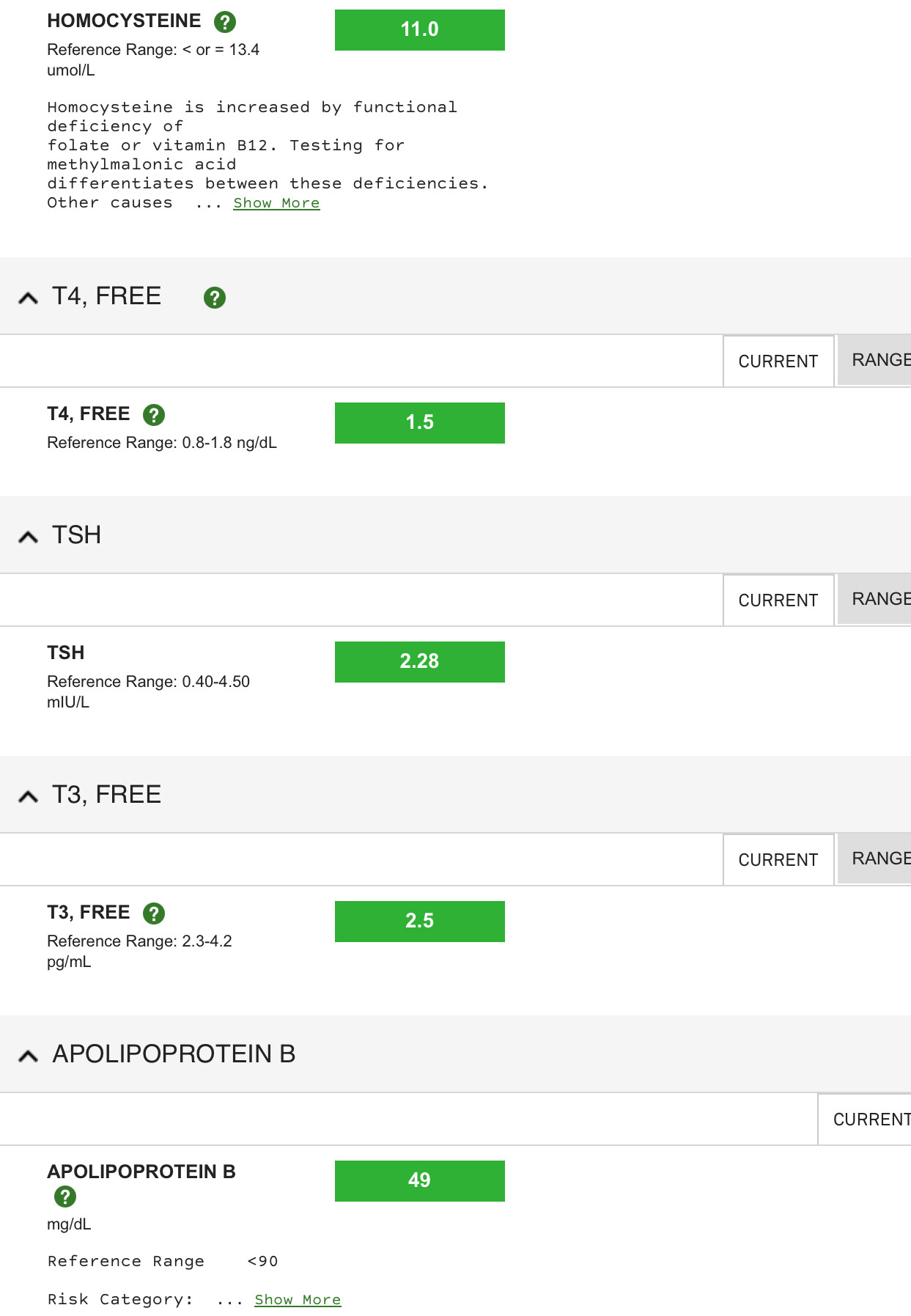
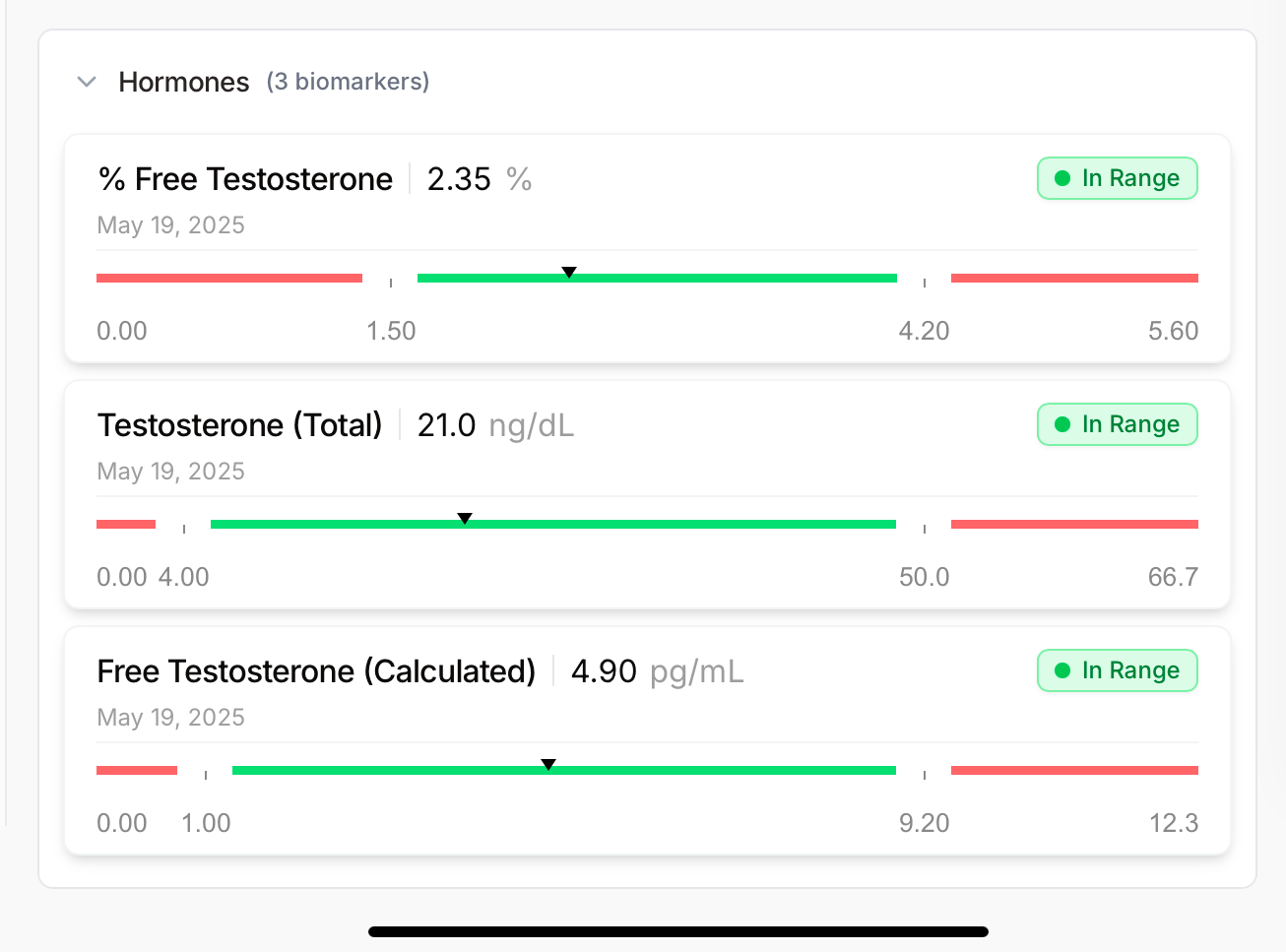
I get labs done 3-4 times per year. If there are recommended labs, by all means, please share. I’ll include my most recent labs from 10/25.
You advice on making sure my doctor is aware of what I do is sound, and I do share everything I take with him because he is fortunately very open minded… albeit not a fan of grey market peptides
I’ve put these into categories and added some doses
General health/longevity:
Blueprint Essential (contains a few things I take individually w/ bonus ingredients) Glycine 1 g taken on occasion
Taurine (aprox 5-6g… I am small so I think I could take less, but the high dose seemed to make sense because I’m vegan?)
Creatine 5g
Sun Fiber 1 scoop (I’m a lemming and recently added because you all say fiber is great)
L-citrulline 1.5g (just recently added after seeing the raves on here and that it might help heart health, see lemming above)
CA-AKG (incase the hype is real)
NACET (100mg NAC/600mg glycine)
Mag malate 100mg (only taking for my mag intake and malate seems to be a good source)
Rapa 8mg
R-Alpha Lipoic Acid 100mg (no idea why I take this other than it was suggested)
Lysine 650mg very randomly
Vanity:
Hyaluronic acid 100-200mg
Tremella
Labs indicate need:
Citocoline/ cdp choline (I was deficient) 500mg
Calciferol (4000 iu total- including blueprint)
TMG 750mg (added when most recent labs showed a jump in homocysteine, but I had labs taken a week post concussion and was recently informed my labs might have been temporarily altered, so I plan to repeat shortly)
Sleep:
Melatonin/glycine mix (10mg melatonin/1g glycine)
Mag glycinate 100-200mg (I don’t need but mag seems like a win)
Brain-one copy of APOE4 and strong family history (grandmother had ALS, mom had PD, and her only sibling has something similar):
LDN (makes me sleep like a baby, so I’d keep this even if useless for brain)
RT or TZ
SS-31 (I just started this and feel it)
Lithium
Methylene blue (not taking often and thinking of deleting)
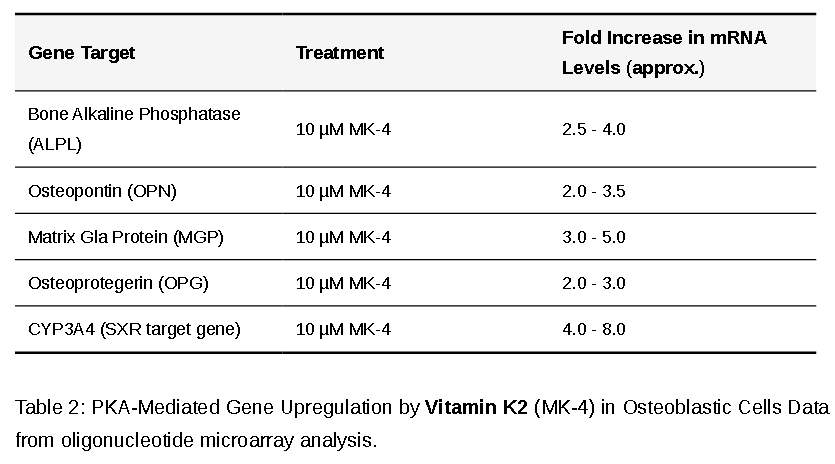
EPA / DHA
Citrate protocol a la John Hemming -possibly helping with bones, too
Urolithin A (incase the hype is real)
Things I need to take:
Established CVD: (CAC of almost 500 a decade ago, elevated Lp(a), coupled w father and grandfather having heart attacks in their 40s.)
Bempedoic acid
Ezetimibe
Colchicine
Repatha
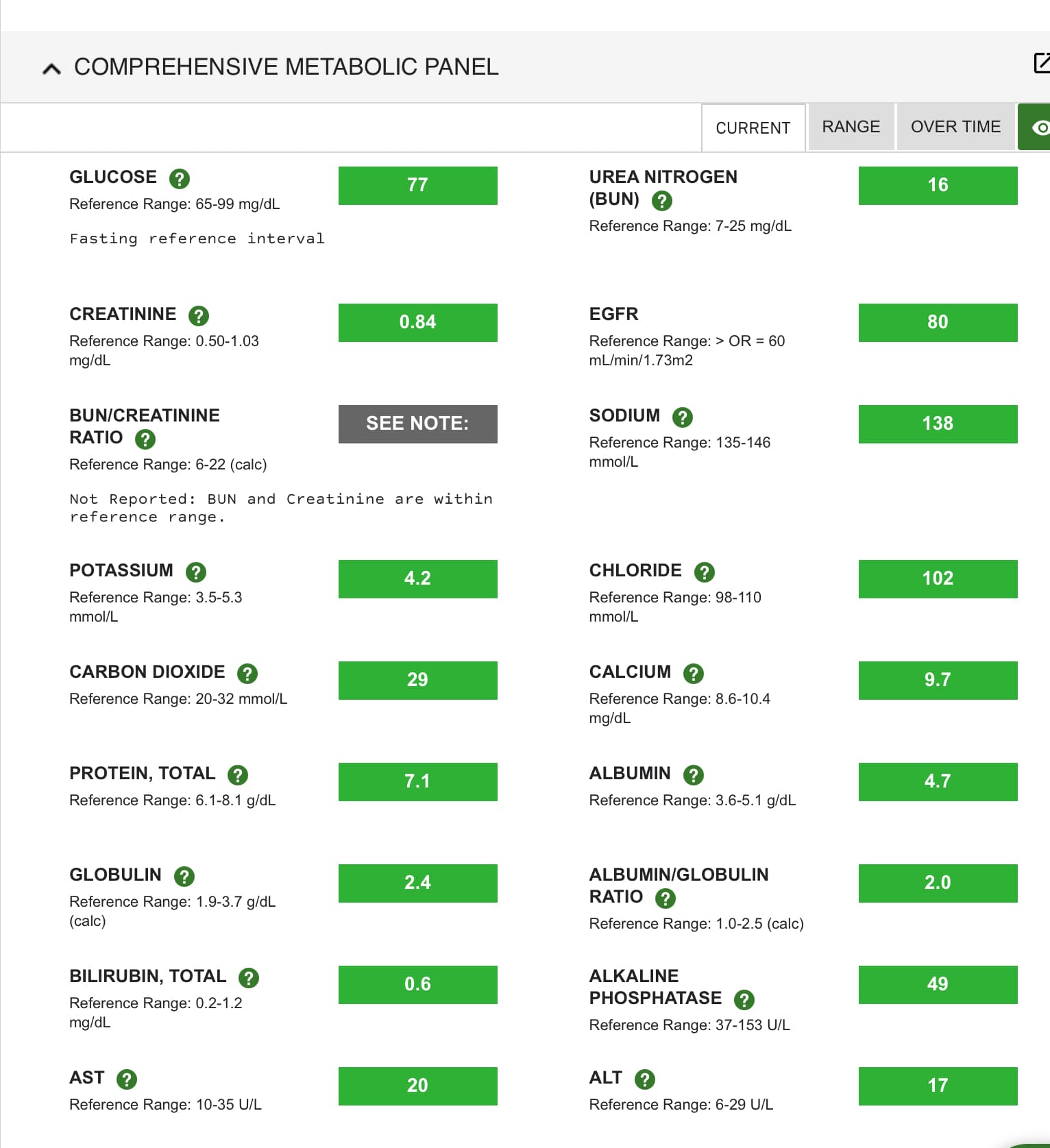
Blueprint Advanced Antioxidants (high vit k to help offset the heart risk of the calcium I’m taking… w bonus longevity/eye health ingredients)
Baby aspirin
Hashimotos/hypothyroid:
t3 ER compounded
synthroid
CGM indicates I’m not naturally metabolically healthy (pre rx, spikes over 200 daily)
Dapagliflozin 10mg
Acarbose 100-300 per day
Osteoporosis:
Calcium 250mg dicalcium malate
Estradiol Gel .5mg (also for building muscle)
Progesterone 100mg (also for building muscle)
@Rika_Qu I wish I had a better answer for you, but I chose that one because our trusted longevity doc here, Grant Fraser, advised me on taking this. I don’t know if this one is his preference for everyone or if it was ‘me’ specific. I’d tag him and he is welcome to share why he suggested it for me, but I don’t think he’ll answer here