Any reason for picking pitvastatin as opposed to say rosuvastatin?
1 Like
Beth - did you mean to list testosterone since progesterone was listed twice? And if not, why not some T?
@DavidCary it was just a mistake… I did a cut and paste and didn’t see progesterone, so i typed it in… I now see it was on the other line :). I’ll go fix it.
And good question… I don’t have a good answer other than I feel fine and no doc has suggested I add it. I know from the olden days I would have worried about increased cancer or heart attack risk. I have not looked into the current thinking on the subject so I realize those concerns might not be legitimate.
Edit:
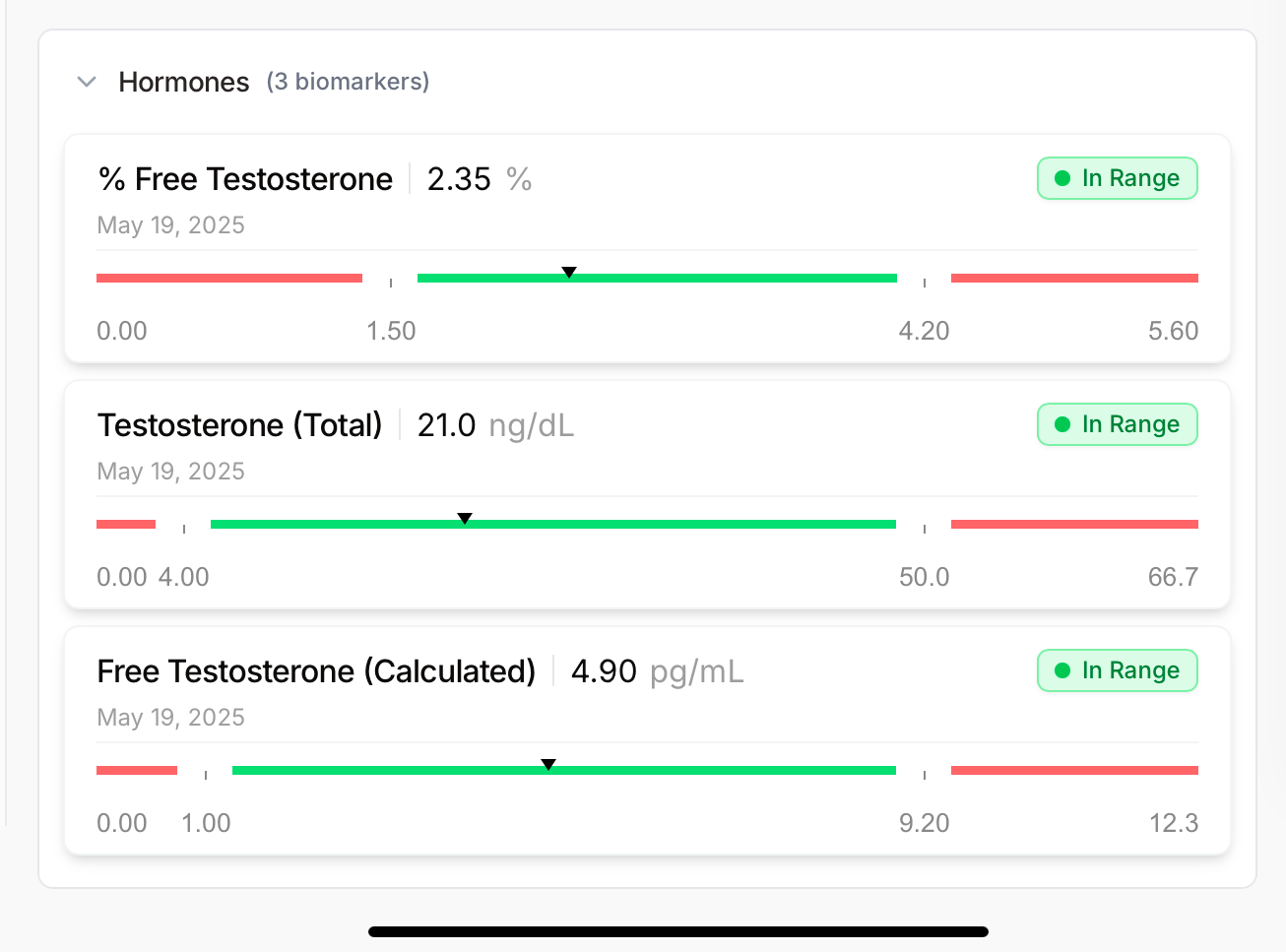
Also, I just realized I did labs in May, here are my results… maybe this is why my doc didn’t suggest it?
2 Likes
Thanks for everyone who chimed in.
What are your stacks then and what do you use for ApoB?
Stain is seeing a lot of back and forth.
Metformin and Berberies? I do use Barberries which you can get from Amazon when eat heavy meals.
1 Like
From Indian Vendors. There is a guy named Paul something who did really well with it. I am a fan of his approach.
I have eczema so my needs is low dose keep mTorc1 less active.
It just worked for me better over time. Doxy is based on research like this and it is a bit of insurance policy: https://www.sciencedirect.com/science/article/pii/S2666354624001728
Beth – Those are very good metrics. Given the complexity and your personal goals, you are obviously doing a great job. I think we may share a challenge. I am trying to simplify my protocols in a systematic evidence-based way. If you do all of the research, it can be a daunting task. Recently, I found that I was making more progress by organizing the supplements I take (including self-prescribed pharma) by health target. For example, I have the relatively common BHMT-08 homozygous polymorphism which is easily addressed via a supplement stack of Phosphatidylcholine, TMG (very low dose, contra common belief), 5-MTHF, Methyl-B12, B6, Creatine, and Mg Glycinate. You can see that some of these supplements can be valuable in relation to other health targets. Thus begins the matrix. Creating a comprehensive supplement matrix across targets in a way that accommodates not only shared purposes but addresses time of day, frequency, with or without food, and contraindications – all while seeking simplification – is where the fun comes into play. I’m enjoying the process and accept that it may take awhile.
3 Likes
General health:
- MicroVitamin by Dr Stanfield
- Plant-based protein powder 30g
- Creatine HCL 5g
- L-Ergothioneine 25mg
Cardiovascular health:
- Pitavastatin 1mg
- Omega 3 EPA-only 1g
- Retatrutide 6mg
Kidney health:
- Empagliflozin 6.25mg
Better Sleep:
- Sleep by Dr Stanfield
- Amitriptyline 25mg
Stomach health:
- Boulardii
- Psyllium husk 6g
Penile health:
- 2.5mg tadalafil
- 6g L-Citrulline
Eye health:
- Astaxanthin 12-24mg
- Lutein 10mg + Zeaxanthin 4mg
Skin health:
- Sunscreen UV50
- Tretinoin 0.05%
- Collagen peptides 12g
Hair (and prostate) health:
- Finasteride 1mg
- Minoxidil 5%
- Ketoconazole shampoo once weekly
5 Likes
@RobTuck
Thanks. Learning your approach is helpful and gives me something to try to wrap my head around to help me further fine tune my ‘mess’. Today was the first day I attempted to list what I take by my goals and I see it does help clarify things. I’ll pm you to ask you more about how you manage the list in regards to the same thing helping various goals.
This is the sort of thing that is way over my head. Ages ago I learned I had the MTHR gene, and I see a lot of you talk about methylation, but it’s just something I have not understood or learned about yet.
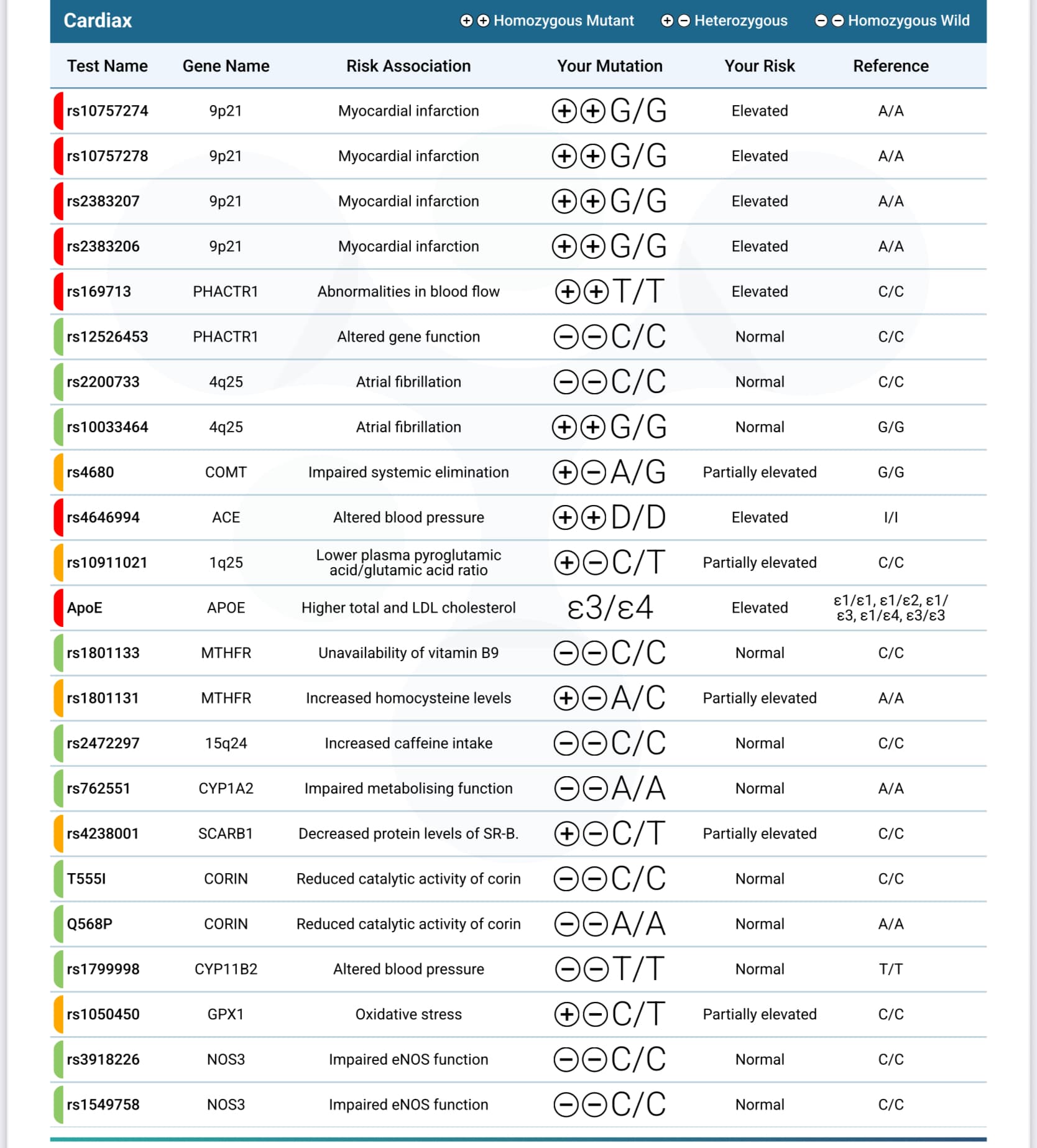
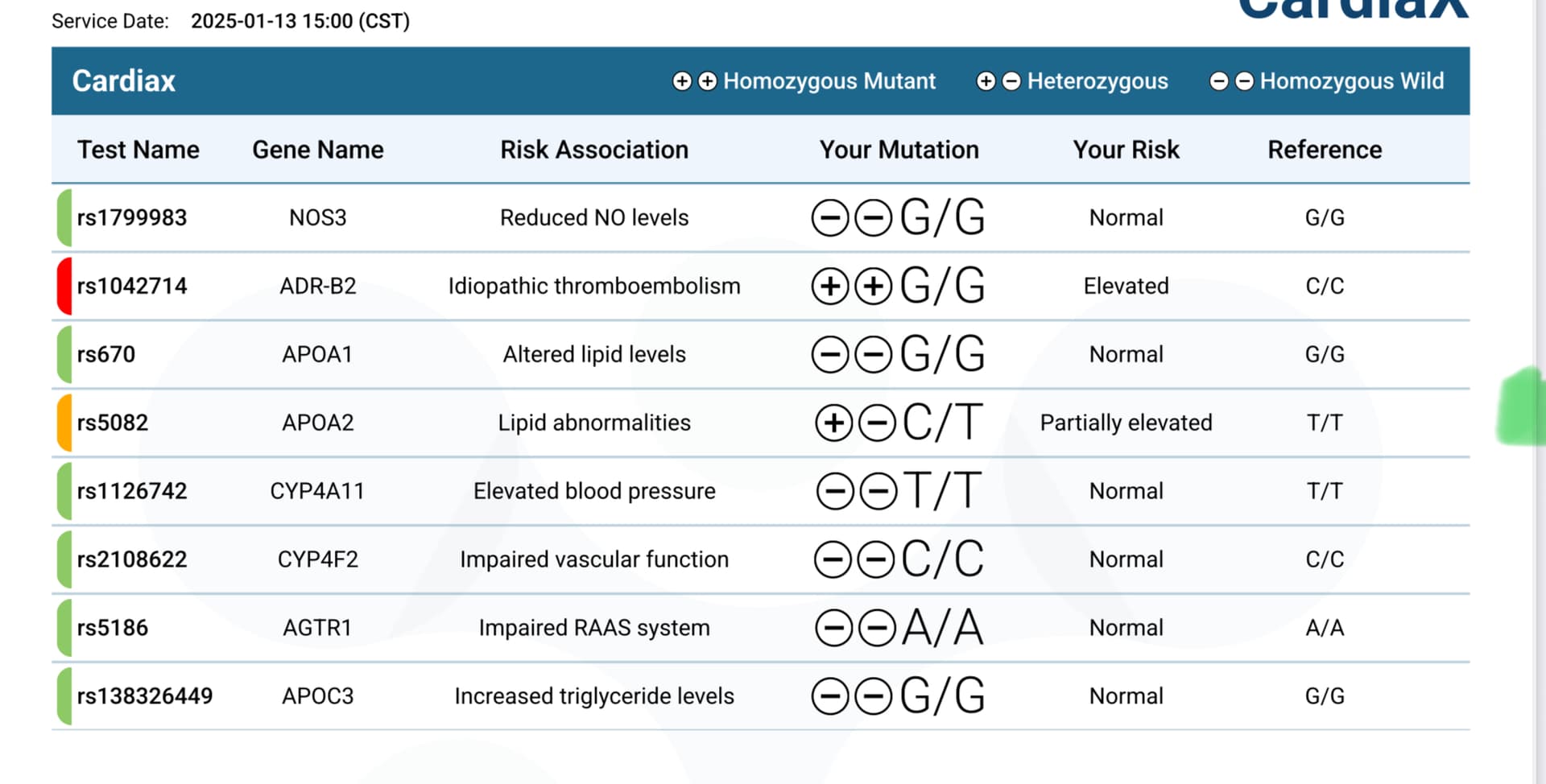
Last year I did take the cardiax test that talks about some of this, but it’s all Greek to me. Just to be OTT, I”ll include those results here.
1 Like
Do you use this for joint pain? If you look it up, long term use isn’t recommended because of its effect on the stomach and kidneys
1 Like
Tons. I’m on my phone atm, bit I’ve written about that many times, citing studies.
Well those are Grok’s words but there are A LOT of studies showing NR boosts NAD levels. Are you specifically saying it doesn’t boost NAD+ at the tissue level?
This is why I take it. The effect on joint pain is a nice bonus though. It was shown to have the greatest reduction in all cause mortality at double the dose I am taking. I don’t think it is harming my kidneys because my Cystatin C was recently 0.64
https://onlinelibrary.wiley.com/doi/10.1111/acel.14334
Abstract
Although most drugs currently approved are meant to treat specific diseases or symptoms, it has been hypothesized that some might bear a beneficial effect on lifespan in healthy older individuals, outside of their specific disease indication. Such drugs include, among others, metformin, SGLT2 inhibitors and rapamycin. Since 2006, the UK biobank has recorded prescription medication and mortality data for over 500′000 participants, aged between 40 and 70 years old. In this work, we examined the impact of the top 406 prescribed medications on overall mortality rates within the general population of the UK. As expected, most drugs were linked to a shorter lifespan, likely due to the life-limiting nature of the diseases they are prescribed to treat. Importantly, a few drugs were associated with increased lifespans, including notably Sildenafil, Atorvastatin, Naproxen and Estradiol. These retrospective results warrant further investigation in randomized controlled trials.
2 Likes
Is Naproxen same as Aleve?
Yea Aleve is just the brand name
1 Like
Testosterone for women (and men) is particularly good for muscle mass and bone strength. The main downsides are potential androgenic effects - hair growth, acne, deeper voice. At female dosing, there isn’t much serious downside. If anything, it would be CV risk but probably minimal.
Other positives are energy level, positive outlook, libido, etc.
Having looked at this for my wife for awhile, I think most post-menopausal women should be on what I term triple therapy - estrogen patch, progesterone pill at night and testosterone cream. Dosing mostly by symptoms but check testosterone levels to avoid going too high. I had a female patient with a 500 testosterone level from pellets. She had no downside but that is nuts. She reported anger issues only when she was low on T strangely enough. No voice changes either. She was 65 with a 50 year old husband …
Overall T is probably more health span than lifespan but fraility and broken hips kill so I think lifespan is likely improved also.
Now, there isn’t going to be any data particularly with starting later. With Estrogen, the thinking by many is that you shouldn’t start over 60 years old I believe.
Lastly, most studies demonstrate neuroprotective action particularly in cell cultures (of questionable relevance). But also in mouse models and some human disease states.
6 Likes
Jonas So, the doxycycline with the rapamycin has nothing to do with the combination of the two. It’s purpose is specifically for Alzheimer’s prevention. Or, did I misunderstand?
1 Like
How is this going? I’ve got some and I’ve been tempted to start trying it out.
In my case I moved over to pitvastatin for its lower impact on insulin resistance. My LDL-C is down in the 40 range now, and so my priority is my slightly raised blood sugar levels: What's the best statin to take? - #51 by vishnu
4 Likes
These supplements may increase blood levels, and perhaps extracellular matrix levels, but the real question is do they increase intracellular NAD+ levels which is where an increased concentration of NAD+ could benefit us.
I haven’t seen any studies that suggest an increase in intracellular NAD+ levels. If you can reference, I’d be happy to take a look, but failing that, I regard these expensive supplements as a waste of money.