Also, CAC numbers are suppossed to go up with age, and these went down. I think a 15% change is more than an error.
1 Like
You may be right, but… In my case I’ve had a series of CAC scans.
5/97 CAC zero
10/20 CAC 157
8/22 CAC 287
6/24 CAC 242,
Current age is 75, Levine bio age 64
So, looking at my last 2 scans, did I successfully reverse the CAC or is it just an overlap due to the error bars not being reported ?
To be fair, I did increase my Rosuvastatin to the max and added Ezetimibe after 8/22
However, my question is still… what are the error bars on the reported CAC numbers?
( I do plan to do another CAC or CTAngio in August to decide on whether or not to add inclisiran.)
2 Likes
From Gemini. It could be statistical error. However…
Even though the 15% decrease could be a technical illusion, this test result is a massive clinical win for a 79-year-old male.
Zero Progression: In an untreated individual, coronary calcium scores typically increase by 20% to 25% every single year as a natural part of aging and progressive vascular disease. Over two years, a score of 323 would normally be expected to climb well over 450.
Disease Stoppage: The fact that his score dropped slightly means his plaque buildup has completely halted and stabilized. The disease is sleeping, not growing.
Either way, it’s a win. We will rescan in 2 years.
7 Likes
The OpenEvidence AI comments:
" Coronary artery calcium (CAC) Agatston scores carry interscan variability of approximately 10–20% , with a standard deviation of roughly 10% on contemporary scanners. "
So for a CAC of 250 the error bars are +/- 25 for a contemporary scanner or as much as +/- 50 for an older scanner.
So, I don’t think we have any proof, in this thread, that CAC numbers are reversible.
3 Likes
I think being able to reduce your CAC score beyond 20% may be difficult. It’s similar to saying I’ll beleive in longevity if someone hits 150 (20% above Jean Calment’s record).
I guess you can either choose to beleive CAC regression or not. Even if you don’t beleive it decreased, it did not gain the 20-25% it should have in a typical man of his age. That is an achievement in and of itself.
I’ll post his updated score after his next scan in 2 years. Maybe it will go down further? Honestly, these results were better than I expected in any case so I am pleased.
Also, they are developing therapeutics which do actually regress calcified plaque. Maybe this will all be a moot point when those drugs are approved.
2 Likes
I asked Claude Opus 4.8 to summarize the clinical and scientific evidence of Low LDL lowering CAC scores. Here is what it said:
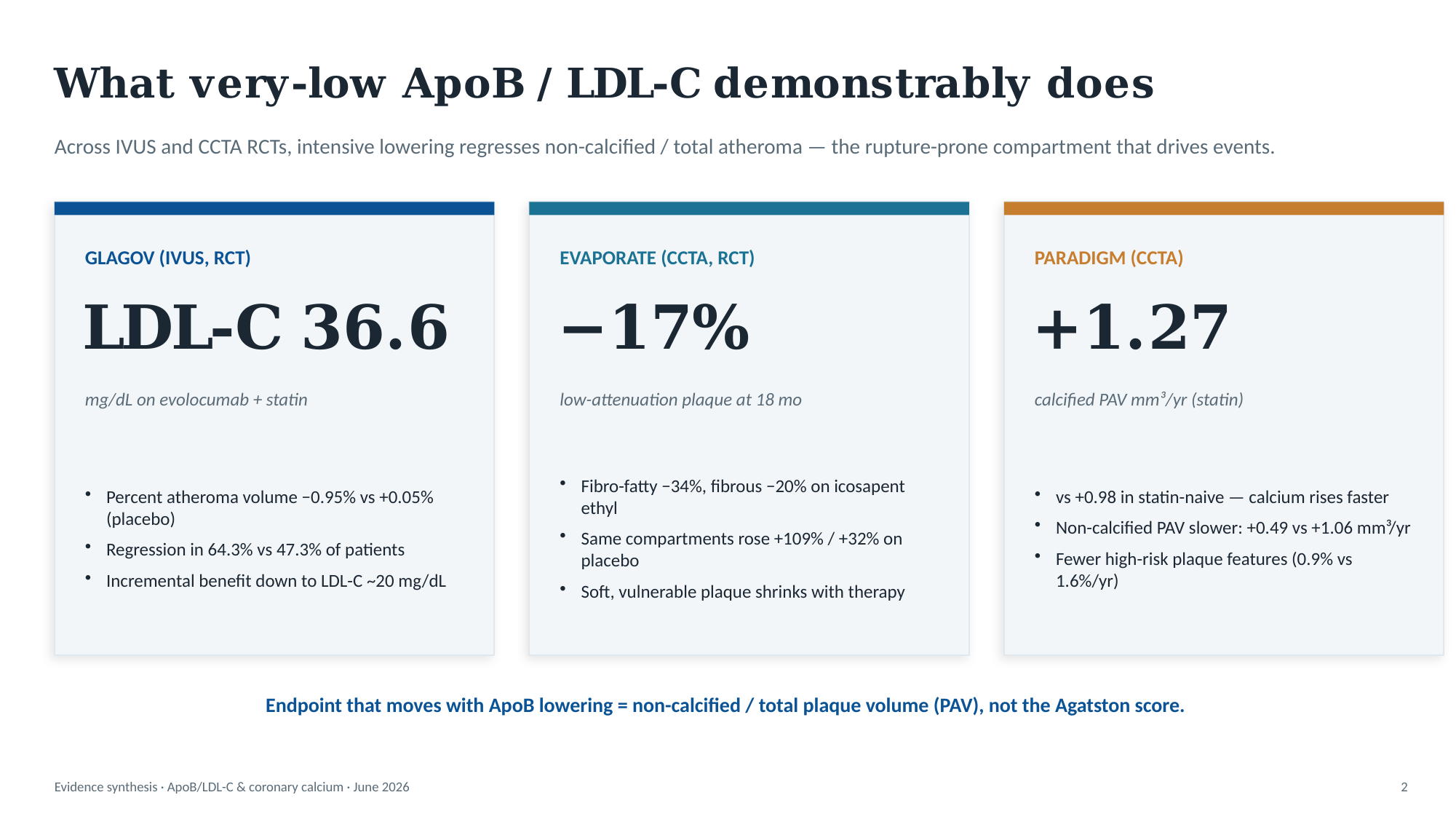
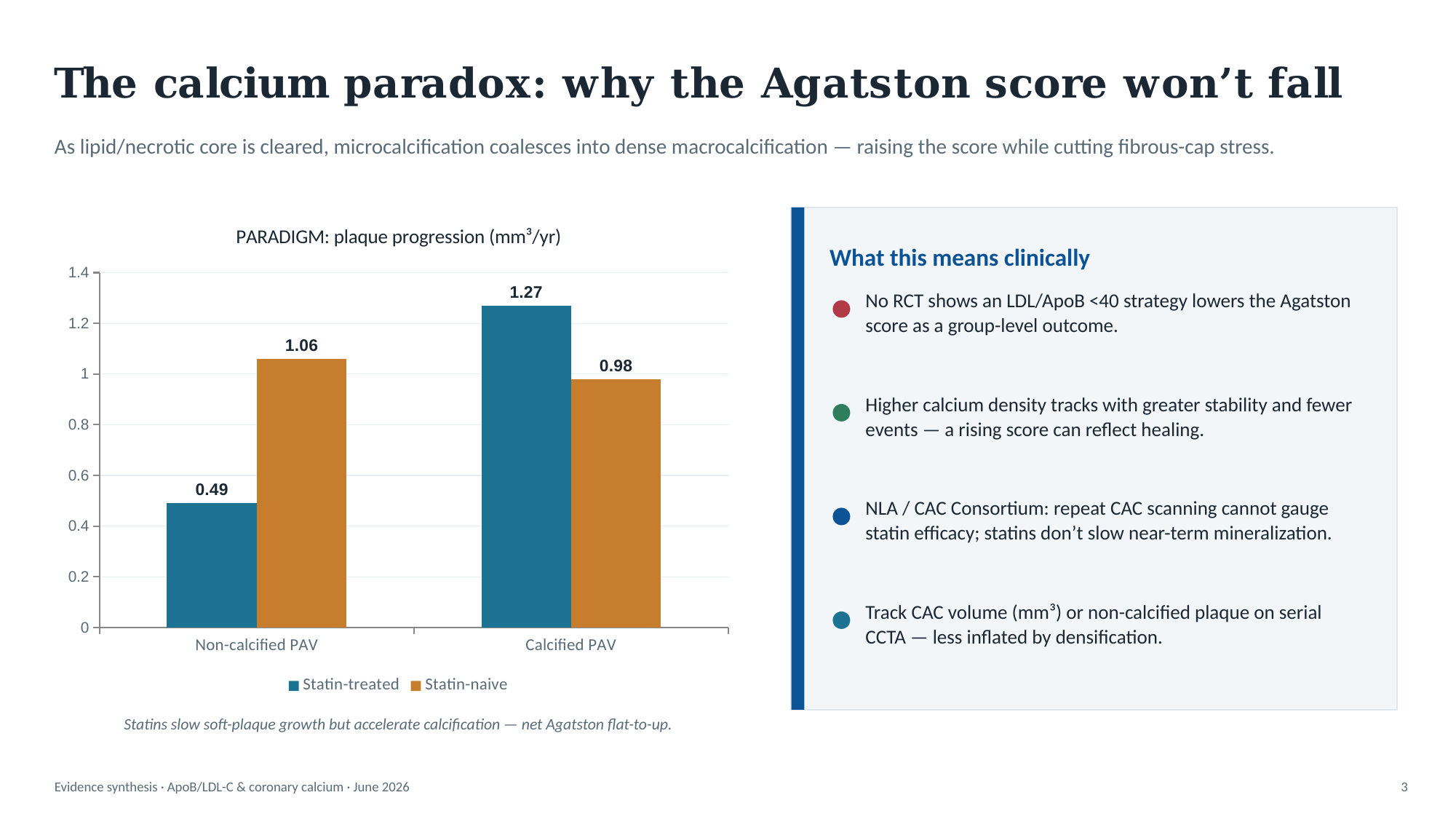
There is good, multi-trial evidence that lowering ApoB/LDL-C to very low levels (<40) regresses non-calcified plaque volume and reduces events. There is no high-quality evidence that it produces a statistically significant decrease in the Agatston CAC score; the densification effect generally pushes the Agatston number flat-to-up even as the plaque becomes more stable. If the goal is to demonstrate benefit on imaging, the defensible endpoints are non-calcified/low-attenuation plaque volume or PAV on serial CCTA/IVUS — and CAC volume rather than Agatston — not the calcium score itself.
5 Likes
This is odd then. If statins and cholesterol treatments are suppossed to increase the CAC, it’s doubly odd that the CAC score declined.
The Average Annual Increase [1]
- Statin Monotherapy: Clinical trials published in journals like Nature and Atherosclerosis show that standard statin therapy typically causes an annual CAC score progression of roughly 25% to 30% per year. [1, 2]
- The Non-Statin Baseline: For comparison, individuals not taking a statin but who already have plaque buildup naturally progress at a rate of about 15% to 18% per year. [1, 2]
- The “Statin Premium”: This means the medication itself is responsible for an additional 7% to 12% absolute increase in the score each year beyond the natural progression of the disease
So, my father, taking a statin decreased by 15% when it was expected he should increase by 25-30% per year. Or 15-18% per year with no therapy. A 15% reduction over two years, is amazing. Even if you assume a statistical error, there’s some valuable results here.
1 Like
Well, I think it entirely depends on what sort of plaque he had.
If a person has lots of soft plaque, and starts aggressive lipid-lowering, you might see a sharp rise in CAC. That’s because the environment inside the artery wall is now not building plaque, so it has time to repair. Remember, calcium is the evidence of repaired damage.
And to be honest, I think measurement variation is incredibly likely.
This study found “The interscan mean variabilities were 21.6% (median, 11.7%) and 17.8% (median, 10.8%) with the Agatston and volumetric score, respectively (P < .01).”
Another study: Inter-scan reproducibility of coronary calcium measurement using Multi Detector-Row Computed Tomography (MDCT) - PMC found inter-scanner variability of 15%
So in your father’s case, 323 to 282 is a 13% decrease (not 15%), and that’s easily within the margin of error. So he could have had a test on Monday, and another on Tuesday, and walked away with 323 and 282.
However, what we can say is that he hasn’t significantly worsened within a year, which is fantastic news all by itself. There’s no way in the world that the statin, ezetimibe and BA isn’t benefiting him, but I also don’t think you can claim you’ve got rid of calcified plaque.
What you hope to see in the coming years is that the number doesn’t meaningfully change. Any current soft plaque will hopefully calcify and stabilise, and he should have stopped building any new soft plaque. However, what you might see, and should prepare for, is the possibility that it jumps next year. If, for example, 323 was the “real” value and 282 is the underestimate, you could also have a 370 next year, which would be a 15% over-estimate. I would say the same thing there too - don’t over-state it, and just stick with the lipid-lowering plan, which is great no matter what!
5 Likes
You could try a CONNEQT which measures arterial stiffness with a blood pressure like device to see if there is a change in its metrics over time. Device costs under $300 I think. I don’t know how adequately that would capture any changes in risk but might be worth a look. Does anyone else have an opinion on this?
3 Likes
It seems to be a good product…
See Product "Connect Pulse" for Blood Pressure, Arterial Health Monitoring
1 Like
My recent CAC score was 0 (0th percentile). Before starting self-directed health interventions around the age 35, I was obese, inactive, smoked, and ate a plaque diet. Does this result show that the body is highly resilient and capable of forgiving past damage? I keep thinking about why Dr Blagosklonny interventions were too late. RIP.
2 Likes
CAC is only looking at calcified plaque, you could still have a ton of dangerous soft plaque. Don’t assume it’s all good news.
2 Likes
Absolutely, but given my age, I am still somewhat surprised at my score given my past. Although nothing can really surprise me anymore. As we age, the likelihood of having calcified plaque increases dramatically. I understand a 0 is common for young adults, but it is increasingly rare as time goes on.
4 Likes
Three tests… at age 64, 66 and 68 years. Still zero. No signs that its not accurate
4 Likes
Luckily, 35 is still very young really, from a cardiovascular point of view. You have to have REALLY horrible genetics and lifestyle to have measurable CVD by 35. (Like familial hypercholesterolemia, full-blown diabetes etc).
And yes, there’s a lot of individual variation. Some people do have LDL-C of like 200mg/dl for decades and never build plaque, while others build plaque super fast at 100mg/dl. You might be a fortunate one who got away with a period of poor lifestyle.
But, as others have said, CAC is a pretty delayed measurement. You get calcium when plaque has formed, gone through cycles of inflammation and repair, and has finally hit a stable repair end-point. So you could have soft plaque right now, which will take a few years to stabilise, and then your CAC goes up. And FWIW, there’s no good evidence that you can actually reverse calcification, but you can reverse soft plaque to some extent. Obviously the best time to start was yesterday, and today is the second best!
4 Likes
My 84 year old dad’s CAC score was 1700. He did 26 weeks of chelation therapy and dropped it to under 100. He never had to see a cardiologist or a neurologist and will probably live to 100 knowing my luck.
4 Likes
What was his chelation therapy protocol ?
Thanks
1 Like
In general lots of good comments already. I think the Claude AI summary RapAdmin provided was particularly informative.
I looked into this myself in the past and the general consensus is against serial measurement of CAC scores once you’ve decided to treat with a statin, or a statin plus Zetia, or statin plus Zetia plus …
I violated this rule myself so I understand why others might as well. But the CAC score’s best use (as of today) seems to be risk stratification. If you were on the fence about whether to take a statin and you got a zero score, you might decide to not take the statin and repeat the test in a few years. That is defendable.
Once you decide to go on the statin, the question is what are we going to do with the new test information? Would you decide to stop the statin if you like the results? What changes in treatment depending on the next test? If the answer is nothing, then probably the next test is not warranted.
But of course if you are paying for the test yourself, and you want it, I see no reason why you can’t get it. It is your body and your money and should be up to you.
Anyway, despite saying all of this, I may get another one in a few years, although I doubt it. Both of my tests yielded horrific numbers, the 2nd worse than the 1st.
At some point one accepts that they have to almost consider themselves as belonging in the secondary prevention group of patients (rather than the primary prevention group), despite never having had an MI yet. I don’t think my cardiologist particularly cares what my future CAC scores are; I am on maximal recommended medical treatment already, my LDL is ~ 40 mg/dL and there is not much else to be done in the absence of symptoms.
Good luck to your father!
3 Likes
I think the main purpose for my father was if his score went up, we needed to think about the possibility of adding stents. And if it went down, which it did, he can feel exuberant about this progress. I think the placebo effect could be beneficial in many cases. You feel like you are getting in better shape and that changes your game mentally. Especially since he was shocked the first time by his relatively high numbers.
3 Likes
My understanding is that stenting stable CVD is not appropriate. For years we all assumed that a stent could be helpful for people with “clogged” arteries but it turns out that, in the absence of symptoms, stenting has shown no benefit. So it is basically no longer recommended.
It is a weird thing because if you are having a heart attack, stenting is crucial and can absolutely save your life. And it seems so physically obvious that it should help in other situations also. But we’ve basically learned it doesn’t. At least this is my current understanding. Obviously I am not a cardiologist.
This having been said, I completely agree with you that the benefit of seeing a lower number is huge, even if it is measurement error. It motivates us normal humans. There was a problem, he has taken action, now the problem was inspected again and shown to be diminished. He is making progress. It makes it easier to keep doing whatever we have been doing. It is great.
3 Likes