Well, I think it entirely depends on what sort of plaque he had.
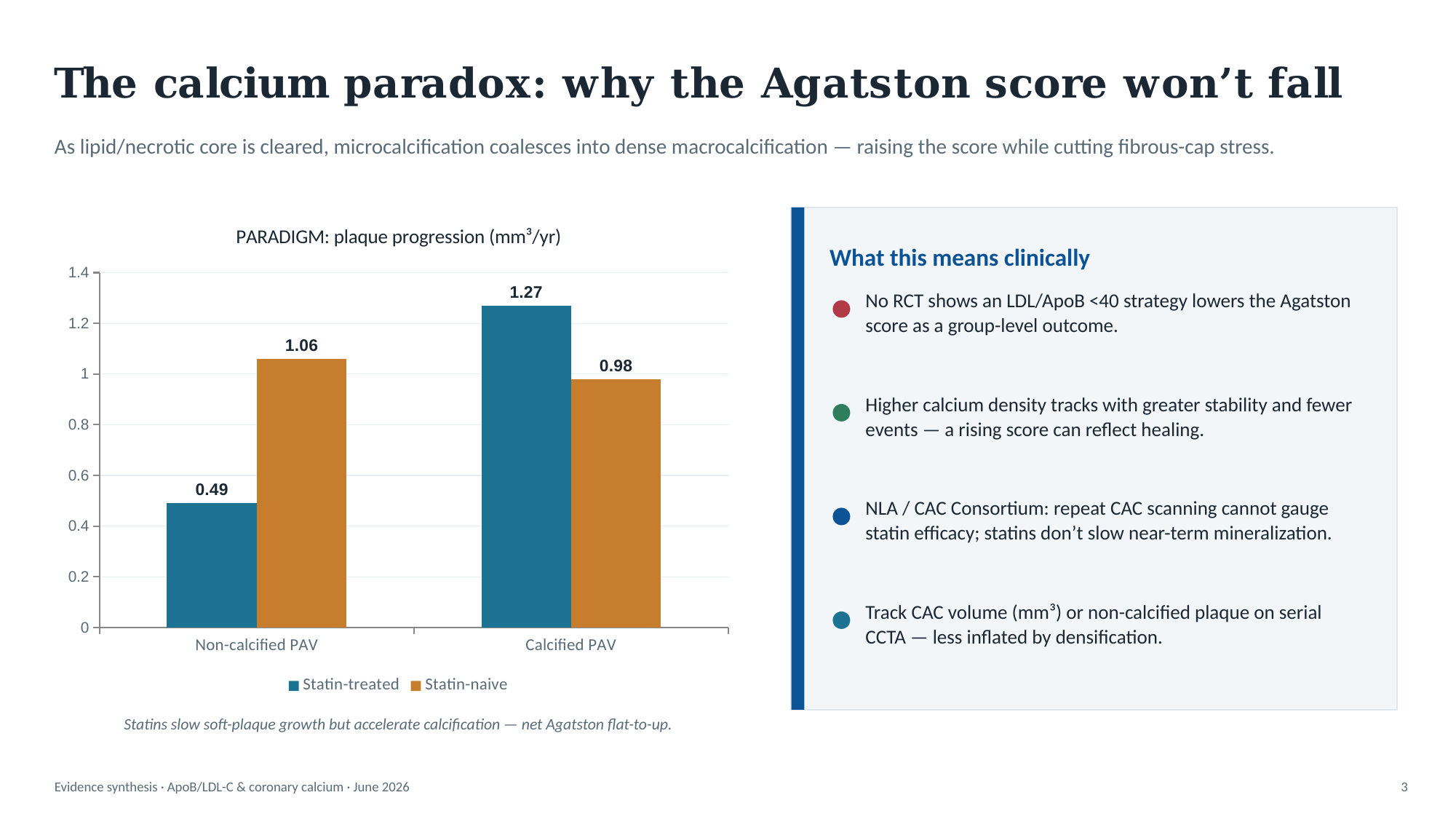
If a person has lots of soft plaque, and starts aggressive lipid-lowering, you might see a sharp rise in CAC. That’s because the environment inside the artery wall is now not building plaque, so it has time to repair. Remember, calcium is the evidence of repaired damage.
And to be honest, I think measurement variation is incredibly likely.
This study found “The interscan mean variabilities were 21.6% (median, 11.7%) and 17.8% (median, 10.8%) with the Agatston and volumetric score, respectively (P < .01).”
Another study: Inter-scan reproducibility of coronary calcium measurement using Multi Detector-Row Computed Tomography (MDCT) - PMC found inter-scanner variability of 15%
So in your father’s case, 323 to 282 is a 13% decrease (not 15%), and that’s easily within the margin of error. So he could have had a test on Monday, and another on Tuesday, and walked away with 323 and 282.
However, what we can say is that he hasn’t significantly worsened within a year, which is fantastic news all by itself. There’s no way in the world that the statin, ezetimibe and BA isn’t benefiting him, but I also don’t think you can claim you’ve got rid of calcified plaque.
What you hope to see in the coming years is that the number doesn’t meaningfully change. Any current soft plaque will hopefully calcify and stabilise, and he should have stopped building any new soft plaque. However, what you might see, and should prepare for, is the possibility that it jumps next year. If, for example, 323 was the “real” value and 282 is the underestimate, you could also have a 370 next year, which would be a 15% over-estimate. I would say the same thing there too - don’t over-state it, and just stick with the lipid-lowering plan, which is great no matter what!