What are they? Are they meaningful?
I heard that drug companies typically choose a easy brand name, but indentation lean towards “brutal” names for the “medical” name to make it less easy for generics once the patent life is over
It will likely have a better brand name
1 Like
If things are not sterile and you are injecting it at home you run the risk of infections and in the worst case death. Some people have no problems with injections at home though. Personally, I would not want to do my own injections at home.
@DeStrider But are you talking about the auto injectors that brand GLP1a comes with or something else?
Auto injectors are safer. Many people turn one injector into several injections on their own. This has safety issues.
I thought the Indian ones were powder and you had to reconstitute them. This is also problematic.
I prefer the pill.
1 Like
Practically very few manufacturers of tirzepatide and semaglutide for injecting are from India . The majority come from China.
1 Like
My side effects from even low dose Rybelsus were intolerable. Profound fatigue was the worst part, although I did lose maybe 10 pounds. The published trials for Rybelsus aren’t impressive for weight loss, but if you tolerate it well and you don’t need to lose much, it’s certainly a viable option.
1 Like
BTW I was wrong about the above. Orforglipron is GLP-1 agonist only, so same mechanism as semaglutide not tirzepatide. I’m much less excited about it now, unless upcoming data show it to be more tolerable than Rybelsus for whatever reason.
2 Likes
Dr, Greger chimes in on ozempic and glp-1RA, and gives some historic context:
Does Ozempic Work?

1 Like
I think it’s pretty cool. Reminds me of the rapamycin origin story.
I thought it was exendin-4, and from this they made exenatide.
I wouldn’t call them no hassle. You need to fast for 30 minutes after consuming the pill in the morning, every morning. Or once a week you can do an easy, relatively painless peptide injection.
2 Likes
Yes, exenatide is the synthetic form of the naturally occurring exendin-4.
1 Like
That is so true. For me I used to have the mindset “when I get rich I could use tirzepatide and possibly alleviate sleep apnea”, then I find out you can get it really affordably. Now I’m just using it, and quite honestly the results have been great and I’m excited to continue.
We shouldn’t have to think like “when I get rich I can be healthy”, it’s so sad that so many people must think like this when there are options.
3 Likes
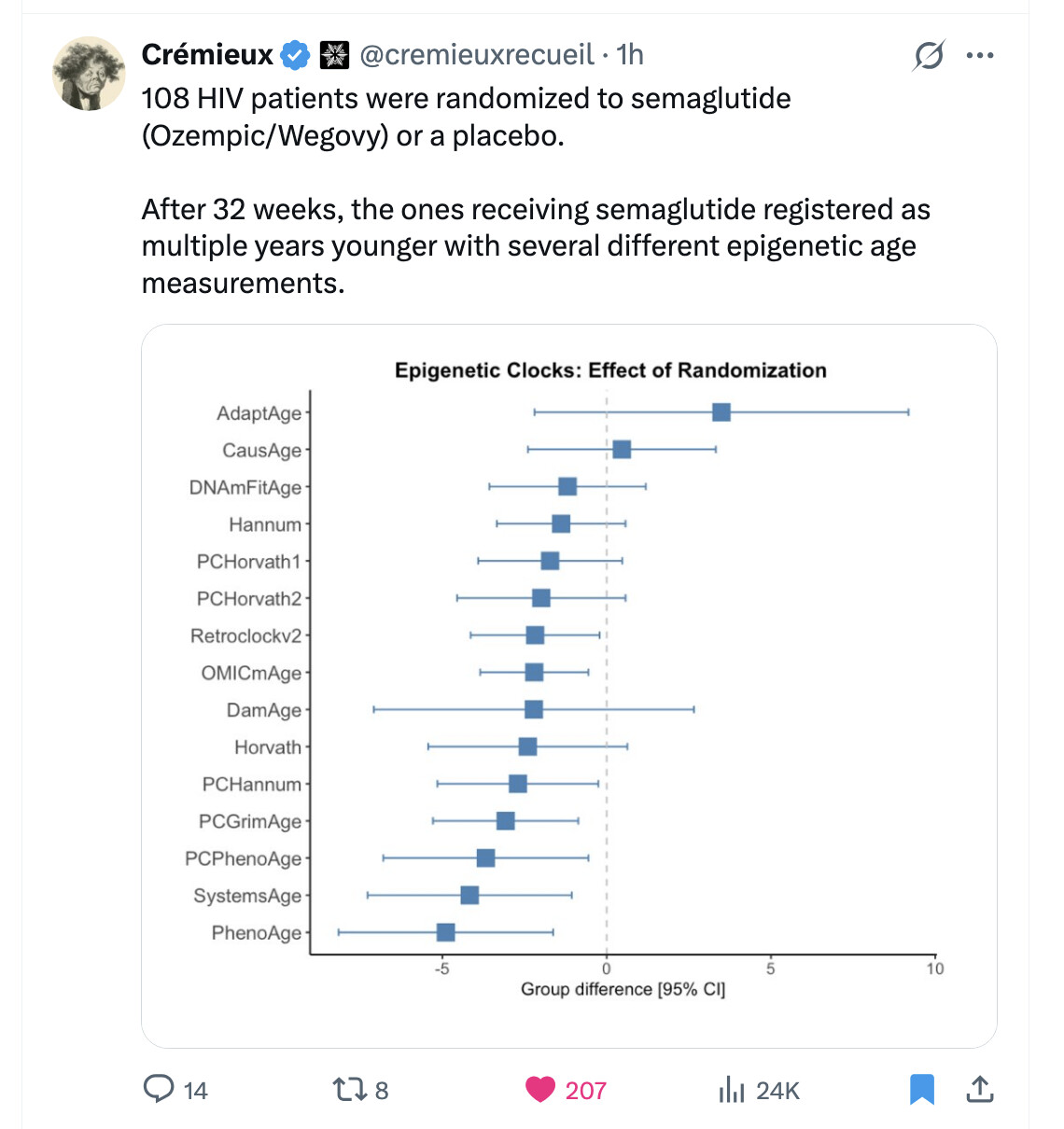
New study on GLP-1 = younger
Anyone think of giving it a go? Or something that is not an injection.
5 Likes
Yep. In my opinion tirzepatide is up there with rapamycin as one of the best currently available and approved for human use longevity intervention drugs.
4 Likes
Mitochondrial biogenesis and protection
Studies have explored the ability of GLP-1 to stimulate mitochondrial biogenesis in pancreatic β-cells, where mitochondrial function is critical for optimal insulin secretion. GLP-1 increases mitochondrial ATP production by driving greater utilisation of glucose and fatty acids and promotes the growth and fission of mitochondria, yielding more of these energy-generating organelles inside cells. It also protects mitochondria by reducing reactive oxygen species (ROS), stimulating mitochondrial dynamics, and shielding against mitochondrial damage.
Marco et al. examined the effect of a GLP-1 receptor agonist on mitochondrial function in patients with type 2 diabetes. Participants were divided into two groups, with or without GLP-1 treatment. Therapy with the agonist benefited polymorphonuclear neutrophils (PMNs) by lowering oxidative stress, boosting cellular energy production, and reducing inflammation and inter-cellular adhesion—findings that suggest therapeutic potential in disorders linked to inflammation and immune dysfunction.
Antiproliferative effects in hepatocellular carcinoma
Krause et al. investigated the antiproliferative actions of liraglutide (a GLP-1 analogue) in HepG2 hepatocellular carcinoma cells at concentrations of 10–20 µM for 24–48 h. Liraglutide induced cellular senescence and autophagy through increased TGF-β1 expression, indicating possible utility as a liver-cancer therapy [20].
Context-dependent effects on autophagy
GLP-1 can both activate and inhibit autophagy, depending on cell type and context. It triggers autophagy via AMPK/mTOR signalling, ROS reduction, and endoplasmic-reticulum stress mitigation, but it can also suppress autophagy through glucagon inhibition, mitochondrial protection, and other tissue-specific mechanisms.
Stem-cell modulation
The interaction between GLP-1 and stem-cell biology holds promise for regenerative medicine and age-related disease. GLP-1 enhances stem-cell proliferation, differentiation, migration, homing, mitochondrial function, and survival. In diabetic rats with nephropathy, Habib et al. showed that exenatide (a GLP-1 agonist) improved the renal-protective functions of adipose-derived mesenchymal stem cells after four weeks [23, 24].
Cardiovascular benefits
GLP-1 receptor agonists (GLP-1 RAs) were first adopted for glycaemic control but also improve classic cardiovascular-disease (CVD) risk factors such as dyslipidaemia, weight, and hypertension. Emerging evidence indicates that GLP-1 RAs may further enhance endothelial function, improve coronary perfusion under stress, and mitigate heart-failure progression.
Neurodegenerative disease mechanisms
Modulating GLP-1 activity can influence dopamine levels in Parkinson’s disease and amyloid-β aggregation in Alzheimer’s disease. GLP-1 RAs reduce oxidative stress, inflammation, and apoptosis, lessening cerebral infarct size and neurological deficits in stroke models. By enhancing synaptic plasticity, they may also improve diabetes- or obesity-related cognitive decline, bolstering memory and learning [29].
APP/PS1 mouse data
In 14-month-old APP/PS1 mice, liraglutide (25 nmol kg⁻¹ i.p. for two months) improved spatial memory, increased neuronal progenitor cells in the dentate gyrus, reduced inflammation and amyloid-plaque load, elevated cortical and hippocampal synapse counts, and markedly enhanced long-term potentiation.
Cancer-risk meta-analysis
Wang et al. compared cancer incidence in 619,340 metformin-treated patients versus 64,230 GLP-1 RA users over five years. GLP-1 RA exposure was associated with lower risks of prostate, lung, and colon cancers but a higher risk of thyroid cancer. Longer exposure further reduced prostate, colon, and lung cancer risk [37]. Because most data are observational, randomised trials are needed to confirm causality.
Muscle-atrophy studies
Using C2C12 myoblasts in vitro and rat models of freeze injury or denervation in vivo, liraglutide significantly protected against muscle atrophy, improving myogenic capacity and overall muscle function [39].
Osteoarthritis model
Meurot et al. found that intra-articular liraglutide (5–20 µg) reduced cartilage catabolism and pain in a mouse model of osteoarthritis. At 20 µg, its effects matched those of 20 µg dexamethasone and surpassed saline controls, also improving synovitis scores [40].
Age-related macular degeneration (AMD)
In preclinical AMD models, GLP-1 RAs reduce inflammation, provide neuroprotection, and enhance retinal blood flow. Seppa et al. reported that six months of liraglutide treatment lowered neuroinflammation, alleviated AMD-like symptoms, and protected retinal ganglion cells in aged rats [41].
CNS distribution and cognition
GLP-1 receptors are widely expressed in the brain and their agonists cross the blood-brain barrier [57, 58]. In a 12-week trial of 50 type 2-diabetes patients (NCT03707171), liraglutide improved scores across all cognitive domains—especially memory and attention—and increased activation of the dorsolateral prefrontal and orbitofrontal cortices, independently of changes in BMI, blood pressure, or glycaemic control [59].
Synaptic plasticity and signalling
Liraglutide prevented high-fat-diet-induced deficits in hippocampal synaptic plasticity in an Alzheimer’s mouse model [75]. GLP-1 receptor deletion reduced long-term potentiation (LTP) in CA1 neurons [76]. GLP-1 RAs up-regulated mTOR and Ntrk2 expression in the hippocampus, crucial for LTP and synaptic function.
DNA repair and senescence
GLP-1 R signalling stimulates apurinic/apyrimidinic endonuclease-1 (APE1) to enhance DNA repair [79], reduces oxidative-stress-driven DNA damage, and counters H₂O₂-induced senescence while boosting antioxidant defences [80].
Cardiomyocyte and mitochondrial protection
Liraglutide shields cardiomyocytes from IL-1β-induced mitochondrial dysfunction, and GLP-1 R activation suppresses methylglyoxal-driven mitochondrial injury in H9c2 cardiomyoblasts [84].
Key survival pathways
GLP-1 acts through the PI3K/Akt/mTOR pathway to prevent cell death [86]; liraglutide protects β-cells from apoptosis via AMPK/mTOR [87]; and the DPP4–GLP-1 axis modulates cellular senescence through AMPK/SIRT1/FOXO3a [90].
Link to the full study without paywall here: Study behind paywall, can anyone find the full study? "Unlocking longevity with GLP-1: A key to turn back the clock?" - #2 by Bettywhitetest
5 Likes
GLP-1s Are a Lot Weirder Than Anyone Thought | The Ezra Klein Show

I. Executive Summary
The core thesis of this discussion is that GLP-1 receptor agonists (such as semaglutide and tirzepatide) have transcended their original purpose as diabetes and weight-loss medications. Originally designed to stimulate insulin release only when blood sugar is high, these drugs are now recognized as powerful regulators of the central nervous system and systemic inflammation. The prevailing scientific view is rapidly shifting to understand GLP-1s not merely as appetite suppressants, but as multi-system biological fine-tuners.
By mimicking gut hormones that travel to the brain, GLP-1s simulate a satiety response that quiets the “food noise” and persistent cravings characteristic of modern obesity. However, the most disruptive clinical finding is that the benefits of GLP-1s are largely weight-independent. Patients experience significant improvements in cardiovascular risk, liver health, kidney function, and systemic inflammation even without massive weight loss. This challenges the long-held medical assumption that fat reduction is the sole driver of metabolic recovery.
Furthermore, the drugs appear to cross into the brain’s reward centers, dampening compulsive behaviors and addictions ranging from alcohol abuse to online shopping. While the exact mechanisms remain under investigation, current data suggests GLP-1s modulate dopamine responses and chronic inflammatory pathways that fuel multiple age-related and behavioral diseases.
Despite their unprecedented efficacy, the drugs expose critical gaps in our understanding of human physiology. Side effects can include severe gastrointestinal distress, rare ocular nerve damage, and unexpected psychological shifts such as anhedonia (the inability to feel pleasure). Moreover, the normalization of these drugs has sparked a controversial wellness culture, where individuals use compounded, unregulated peptides for physical optimization rather than medical necessity. The consensus is that while GLP-1s offer a revolutionary tool against diet-caused metabolic diseases, deploying them as lifelong interventions—especially in pediatric populations—carries unknown long-term risks.
II. Insight Bullets
- The Brain-Gut Axis: GLP-1 medications target receptors in the brain to artificially signal that the body has consumed a toxin, safely triggering nausea and satiety to turn off hunger.
- The Weight-Independent Heart Benefit: Major cardiovascular event risk drops by roughly 20% for users, an improvement that occurs independently of how much total body weight is lost.
- Inflammation Tuning: These drugs act as systemic anti-inflammatories, calming the chronic immune responses that drive cardiovascular disease, diabetes, and obesity without shutting down the entire immune system.
- Resolution of Sleep Apnea: Clinical data indicates tirzepatide reduces sleep apnea severity by over 60%, resolving the disease entirely for nearly half of the patients in recent trials.
- Reward System Modulation: By altering dopamine pathways, GLP-1s inadvertently dial down cravings for alcohol, nicotine, and compulsive behaviors, though large-scale clinical trials are still ongoing.
- The Willpower Myth: The immediate success of these drugs strongly suggests that chronic overeating is driven by neurobiology and environmental design, not a lack of moral discipline.
- The “Anhedonia” Effect: A significant psychological side effect for some users is emotional flattening, mild depression, or loss of joy, resulting from suppressed reward pathways in the brain.
- Lifelong Dependency Reality: Once a patient stops taking the medication, the brain’s original appetite settings return, leading to rapid weight regain and recurring food cravings.
- Unregulated Peptide Markets: The success of GLP-1s has spawned a dangerous grey market where consumers purchase unverified, potent hormone stacks (like retatrutide) for cosmetic weight loss.
- Pediatric Unknowns: Prescribing severe appetite suppressants to children during critical phases of physical and neurological development introduces unquantifiable long-term risks.
- Rare Ocular Risks: Recent safety surveillance has flagged extremely rare but permanent vision loss—Non-arteritic Anterior Ischemic Optic Neuropathy (NAION)—linked to semaglutide.
- Gastrointestinal Paralysis: The mechanism that successfully slows stomach emptying can lead to severe side effects like chronic vomiting and, in extreme cases, gastroparesis.
- Dementia Prevention Ambiguity: While observational data showed lower dementia rates among users, recent randomized trials failed to prove that GLP-1s reliably reverse active Alzheimer’s disease.
- Organ-Specific Healing: Beyond systemic inflammation, the drugs send direct healing signals to specific organs, clearing fat from the liver and improving kidney filtration.
- The New “Worried Well”: The medical narrative is shifting from treating the chronically ill to optimizing the moderately healthy, pushing pharmaceutical resources toward lifestyle enhancement.
IV. Actionable Protocol (Prioritized)
High Confidence Tier
- Cardiovascular Protection: For patients with established cardiovascular disease and elevated BMI, use semaglutide to achieve a confirmed 20% reduction in major adverse cardiac events, regardless of total weight loss. Supported by clinical outcome data.
- Sleep Apnea Resolution: Adults with moderate-to-severe obstructive sleep apnea and obesity should consider tirzepatide, which has been shown to reduce breath-holding episodes by up to 63%. Supported by recent phase 3 trial endpoints.
Experimental Tier
- Addiction and Craving Management: Off-label use of GLP-1s for alcohol use disorder shows promise in suppressing cravings. However, clinical backing is currently limited to small-scale pilot studies, such as a recent 48-person randomized trial on alcohol consumption.
- Cognitive Decline Prophylaxis: Using GLP-1s strictly to prevent dementia or Alzheimer’s remains highly experimental. Current trials have not proven clinical efficacy in reversing or halting active disease progression.
Red Flag Zone
- Grey Market Peptides (Safety Data Absent): Do not inject unapproved, compounded research chemicals like retatrutide purchased from unregulated online vendors. These lack regulatory oversight and carry severe risks of contamination or incorrect dosing.
- Ignoring the Rebound Effect: It is a critical error to view GLP-1s as a temporary “jumpstart.” Discontinuation almost universally guarantees a return of extreme appetite and rapid fat accumulation.
- Vision Loss Ignorance: Any sudden blurring or loss of vision while taking semaglutide requires immediate discontinuation and emergency ophthalmological evaluation due to the risk of NAION.
3 Likes
So… if the GLP-1 peptides are a lot weirder than anyone thought, what about all those other peptides that haven’t even had human studies ![]() ?
?
4 Likes
Just a quick add here while we’re talking about GLP agonists. I have written about this elsewhere and have not encountered anyone with the same “adventure,” but the literature does raise a caution, so – FWIW
I used 3 grams Rybelsus, about once per two days, for a few weeks. Went from 105 to about 96 pounds. Developed severe pain, which it turned out (CAT scan) were gall stones.
I also lost significant muscle. Has taken months and months of work to get my butt back, and shoulders and arms not there yet.
I wish there were a way to majorly reduce the rybelsus dose to, about 1.5 – half the current non therapeutic starter dose. Here’s a business opportunity –
1 Like