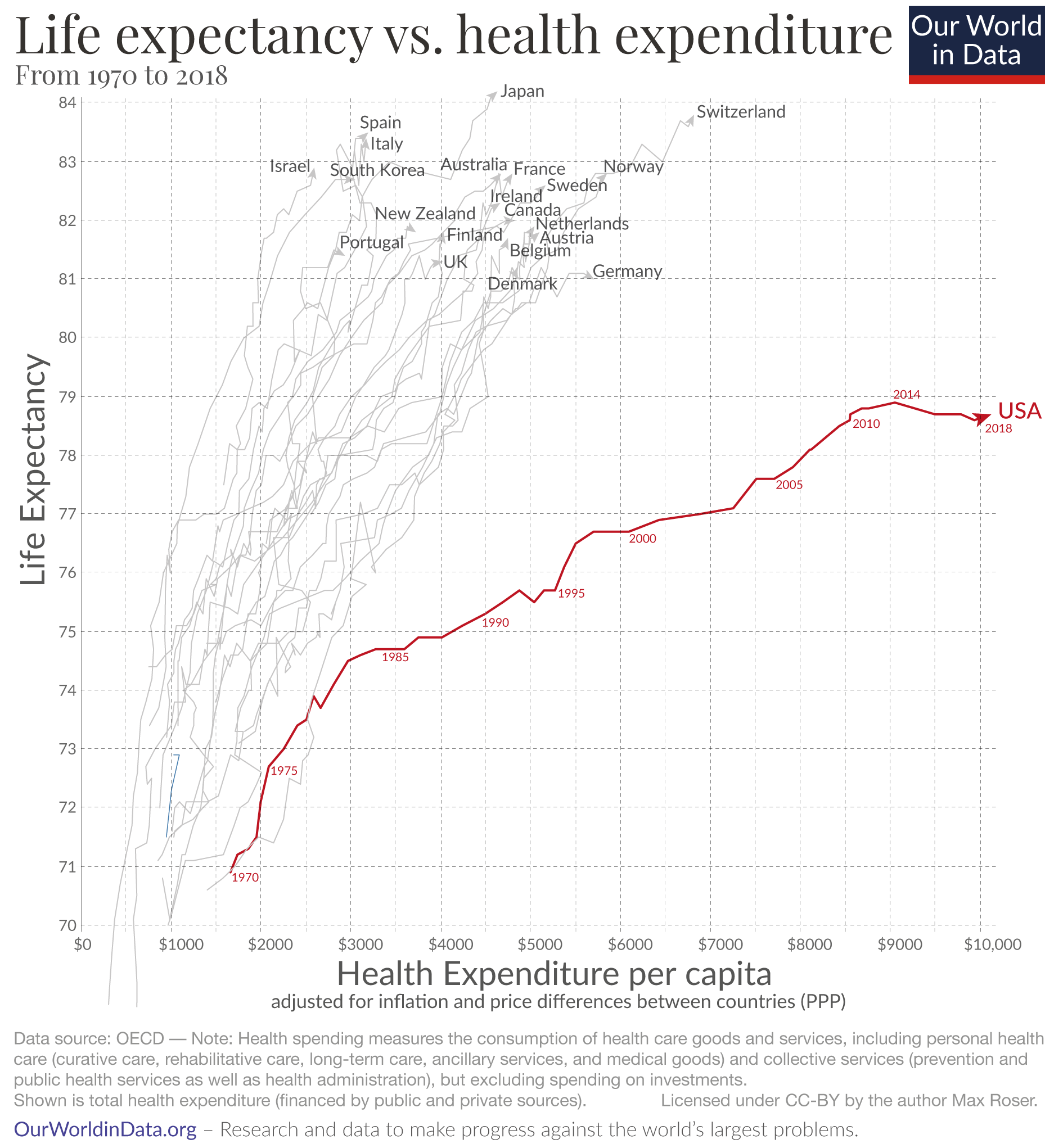
Globally, the medical systems in all developed countries (and even more so in undeveloped countries) focus on “sick care” - waiting until people get sick before they really treat them. Though I guess with universal healthcare as in all other developed country but the USA - you at least get regular checkups and early treatment for health problems (for people with poor or non-existent health coverage), before the problems get really bad and lifespan limiting. But generally, yes, I agree the healthcare system needs to move from what might be called a “defensive posture” to an “offensive posture” - i.e. truly targeting disease risk minimization as early as possible, and not just waiting for it to happen before doing anything.
Cost of medicine in the US is a huge issue, the US pays the highest for its drugs of any country.
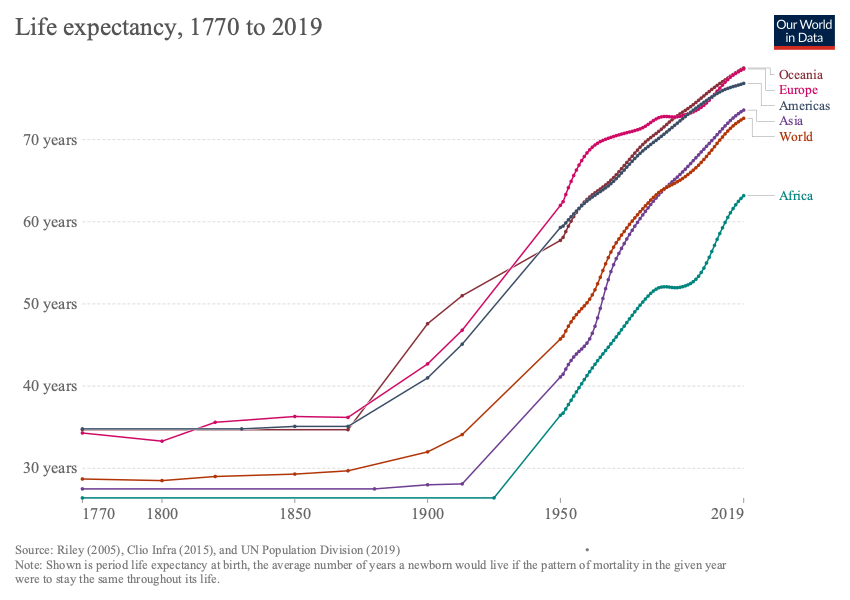
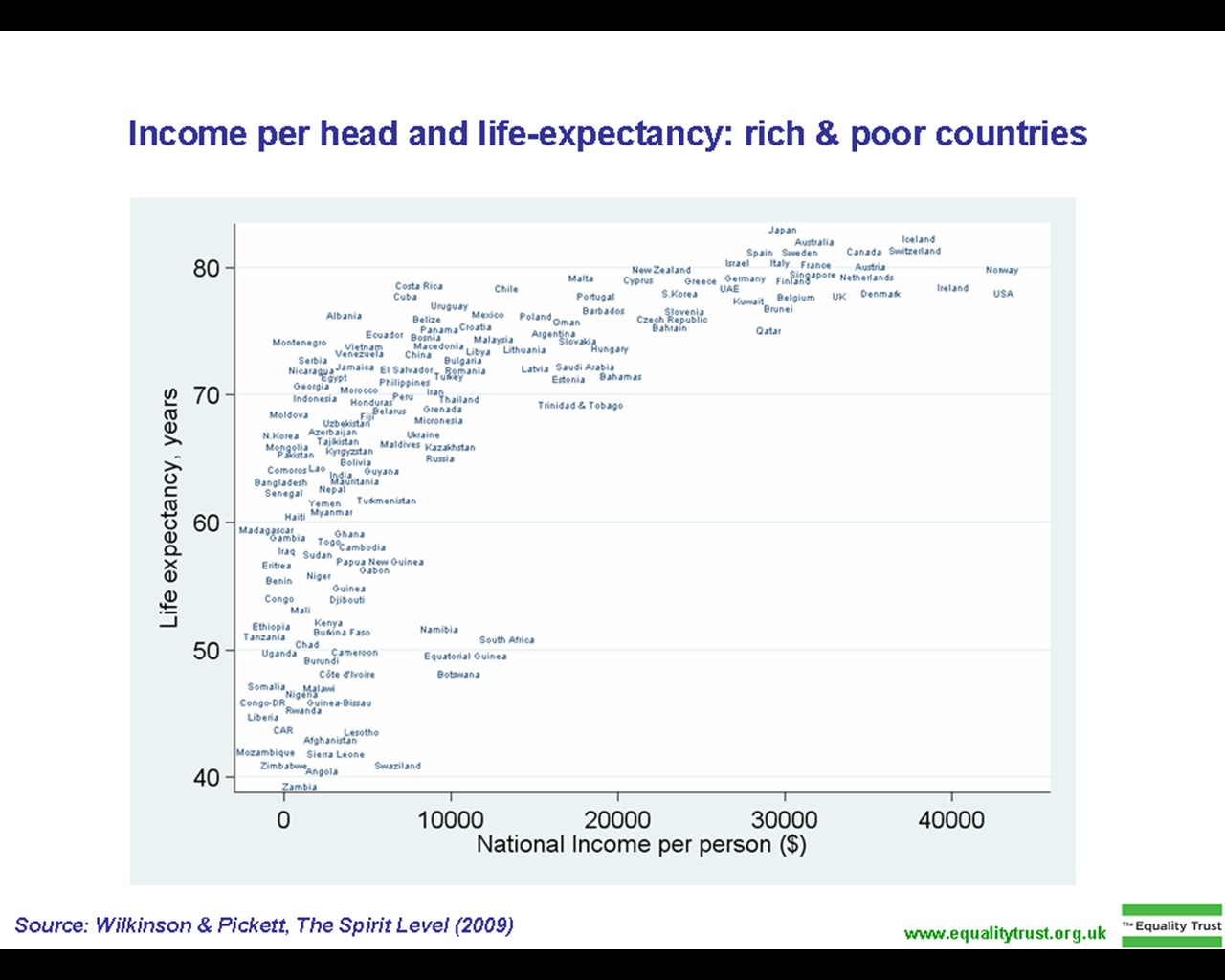
Its going to be really interesting how this issue of lifespan / life expectancy in different countries plays out in the next 50 years as longevity drugs and therapies become more prevalent.
Obviously - most of the people on this forum are much, much more aware of their health and lifespan options and choices and will likely be in the top 1% of lifespan improvements compared to the regular population.
But as I was reviewing the data and writing up the article on the MBS/Saudi $ Billion / year Hevolution Foundation plans, I began thinking about how this acceleration of the field might play out at a population level. Its a little bit like how the Internet impact all aspects of business during the first two decades after adoption took off in the late 1990s. It quickly became obvious in the business world that “network effects” were a dominant force in driving success in Internet business; the more users / vendors a marketplace (e.g. Craigslist, eBay, Amazon, Facebook) had, the more people wanted to visit it, the more people wanted to visit it, the more vendors wanted to use it, etc… so a very rapid transition to monopoly for many segments of the market.
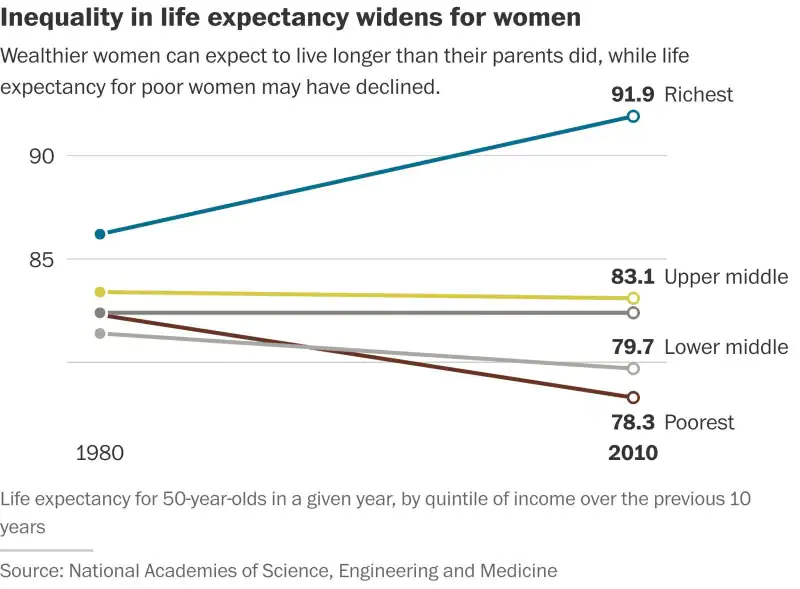
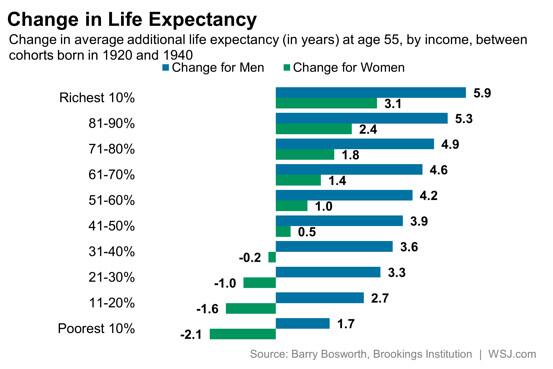
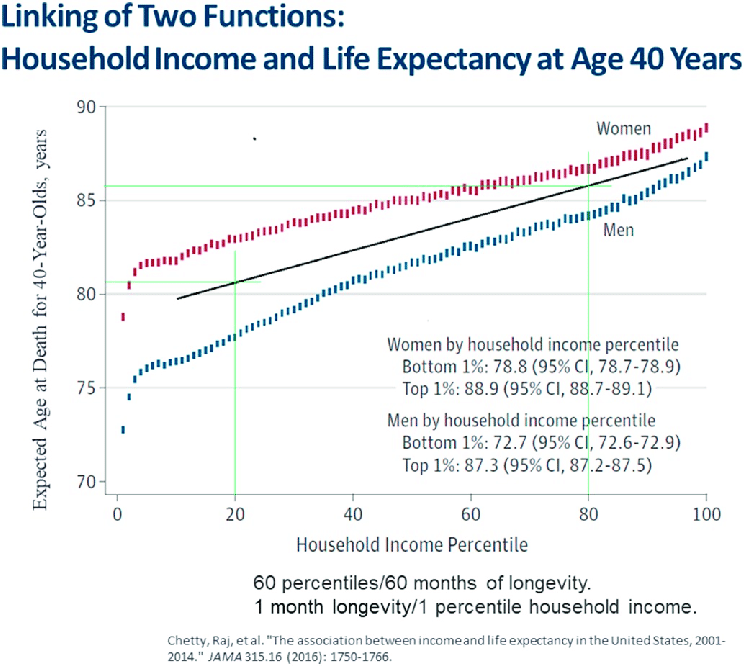
It doesn’t take a huge leap of faith to see that a similar positive feedback loop / market dynamic could take place in the Longevity Therapeutics / Life Expectancy “market” and society more broadly. It seems likely that wealth inequality and lifespan inequality will be mutually reinforcing; the more money you have, the more you will spend on health / longevity therapeutics and therefore the longer you live, the longer you live the more money you can make, the more wealth you can accumulate…
We can already see hints of this trend already in the US … Peter Attia is a great popularizer of longevity science, and I’ve also heard that he business model for his medical clinic is functioning as a high-end concierge medical clinic type service where he charges clients $160,000 per year for his lifespan / healthspan maximization service. Peter Diamandis and Craig Venter have started the company Human Longevity Inc focused on a similar area: The company maps clients’ genomes and subjects them to regular full-body MRI scans and various blood tests to fight diseases associated with aging. The service starts at $7,500 and rises to $19,000 for a “platinum” package. As the geroscience / longevity biotech progresses over the next decade, I suspect we’ll see a lot more of this types of businesses. The key issue that people are trying to overcome is that the cycle time for biotech / medical innovation (clinical trial cycles that take years, patent protection that is 20 years, etc.) is all relatively slow compared to the human lifespan, so it will be worth a lot to people to be relatively early adopters (but not too early) for the latest longevity technologies that are a good match for their personal biology / genotype.
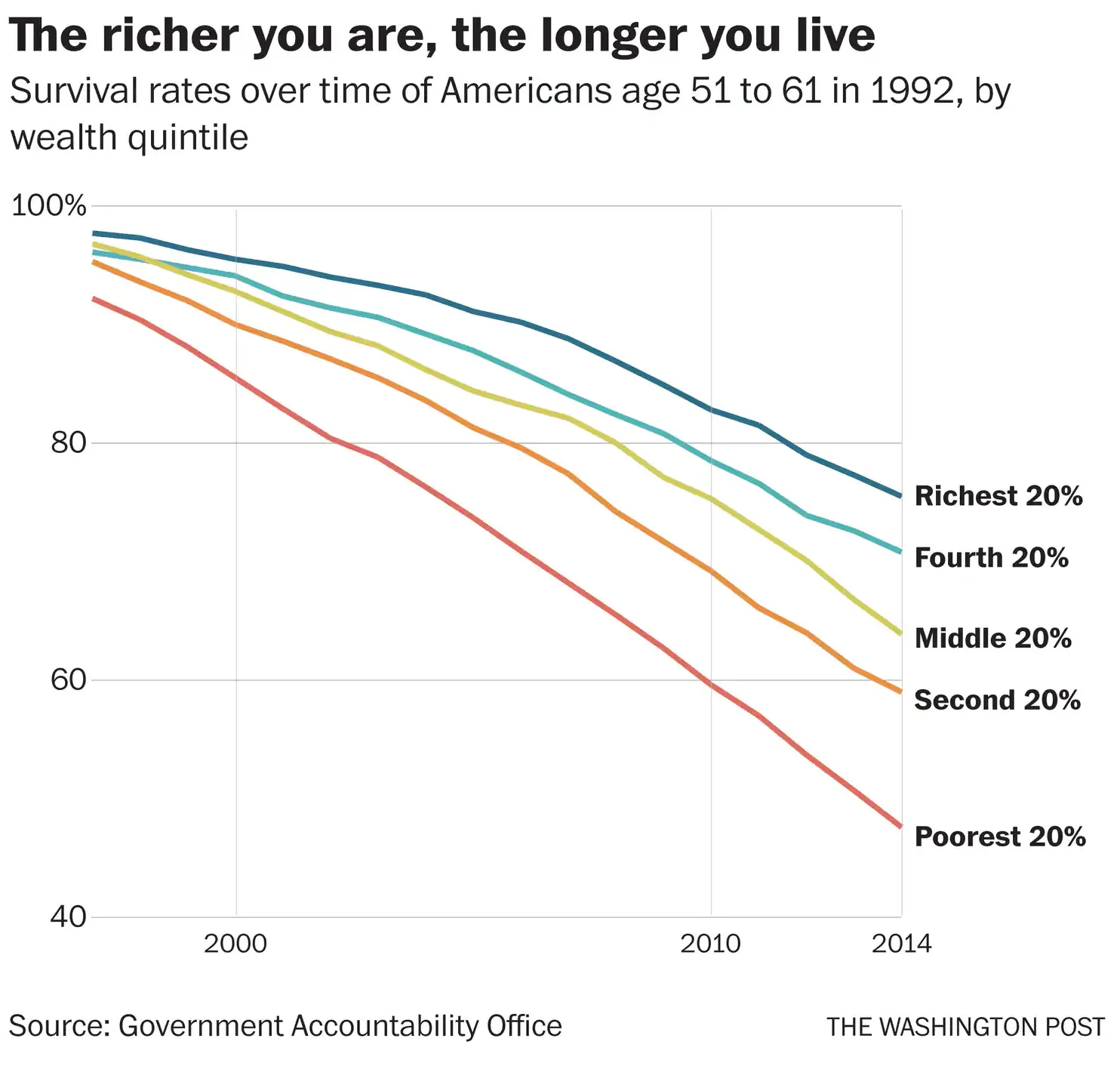
What does society look like if the top 1% of the wealthiest have life expectancies that increase 10%, 30% or 60% faster than the life expectancy increases of the bottom 95% of the population? Prices for longevity technologies may come down over time, but the wealthy will repeatedly and regularly get the most effective and expensive therapies as they become available, so the “lifespan inequality gap” will always grow. It would be interesting for some PHD students to model these different scenarios out over time and see what the results are.
How long will it be before human society starts looking like that of the bee colony, where the queen bee lives 5 to 10 times longer than the worker bees?
Then there are also second-order effects that could and should be looked at… Does the motivation of a much longer life (as the lifespans of the top %0.1 starts to diverge significantly from the mean) motivate more violence / social instability? What happens to capitalism and entrepreneurship where the difference between the winner and loser in a given market means not just much nicer houses and yachts, but potentially many dozens of years of healthy life? Does it result in an even more “no holds barred” deadly type of capitalism more like the historic Russia Oligarch model of the 1990s and 2000s, where people will do anything to become the oligarch?
I hope this isn’t what happens, but I suspect it will. When I read that the Saudi Royal family spends $1.5 million for a health checkup at the Mayo Clinic I realized that if the Saudi Royal family will spend $1.5 million on a simple health checkup, what are the limits they would spend to get an additional 30 to 100 years of healthy life? I suspect we have that answer now with MBS’s $Billion/year investment in Longevity Biotech / Geroscience. And this “willingness to spend” on longevity will increase dramatically, I suspect, as longevity science becomes more clinically validated. So you have a potential exponential growth in spending in this market over the next 20 years.
What do other people think about this? Maybe I’m being too alarmist on this issue.