Source: https://x.com/VamsiMootha/status/2059688512765452488?s=20
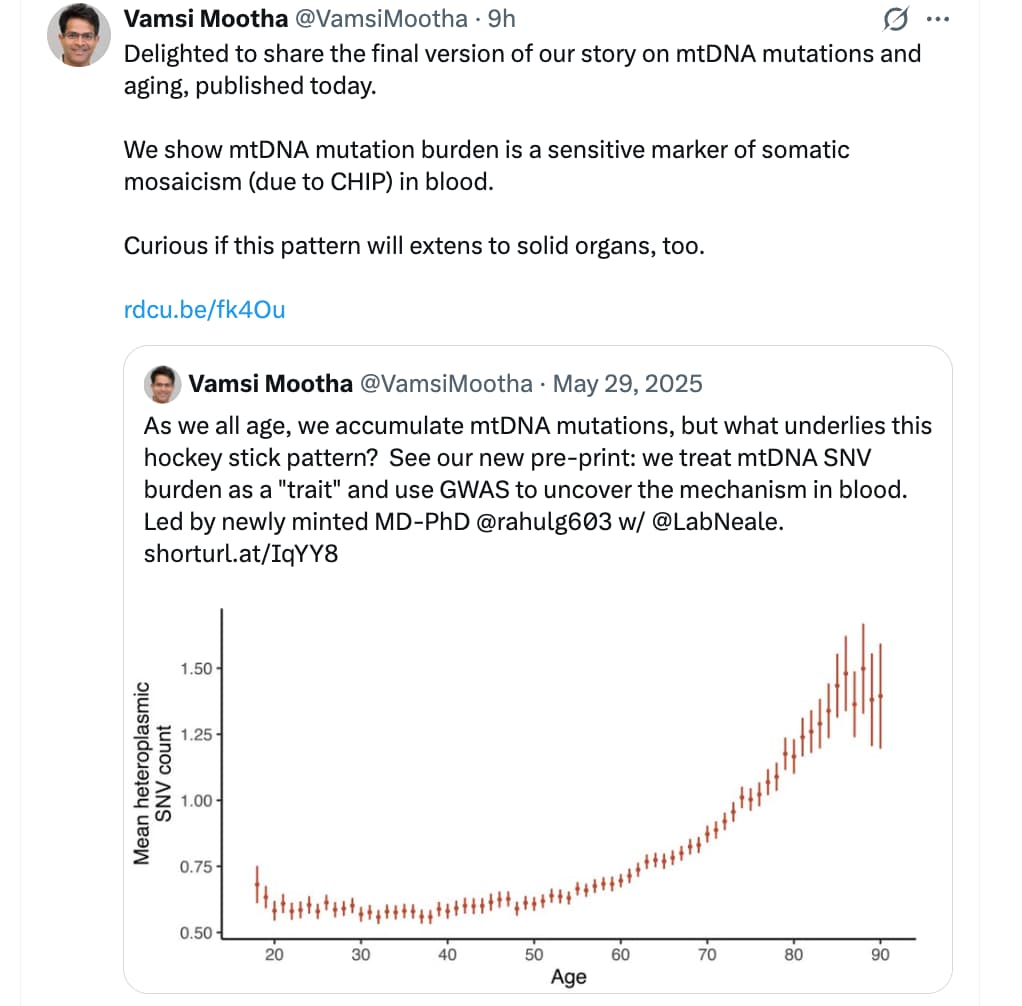
I wonder if it might be helpful to track the level of mtDNA mutations that a person has?
From Gemini:
Next-Generation Sequencing (NGS) architectures, including Whole Genome Sequencing (WGS) and targeted mitochondrial sequencing, can identify both the specific sequence variants in mitochondrial DNA (mtDNA) and quantify their heteroplasmy levels—the precise ratio of mutated mtDNA molecules to wild-type (normal) mtDNA molecules within a given sample.
Because cells contain hundreds to thousands of copies of the circular mitochondrial genome, quantifying this ratio is critical; the clinical or physiological impact of an mtDNA mutation is directly dependent on the percentage of shifted genomes.
Sequencing Methodologies and Detection Thresholds
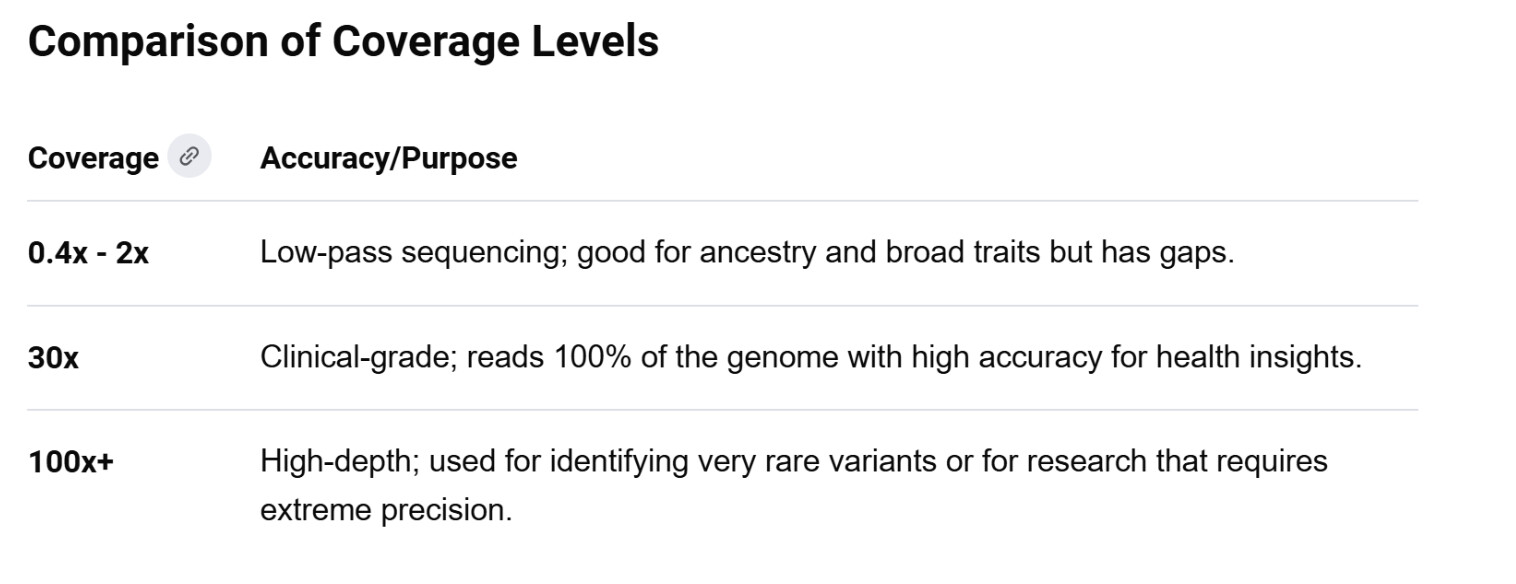
The capacity to accurately quantify mtDNA mutation levels depends heavily on the specific sequencing approach and the depth of coverage achieved.
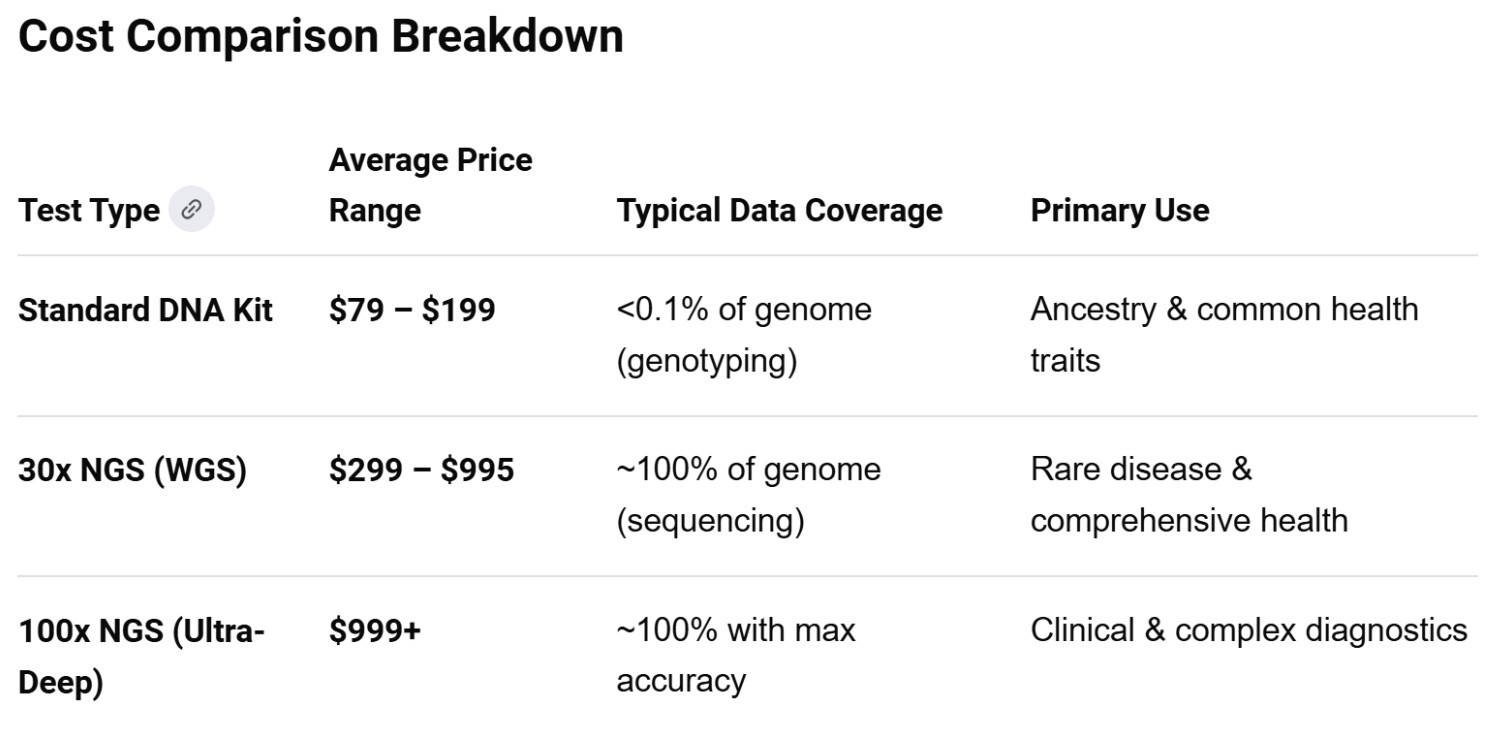
1. Standard Whole Genome Sequencing (WGS)
-
Mechanism: Standard WGS targets the entire cellular DNA extraction. Because mtDNA is highly abundant relative to nuclear DNA, a standard 30x nuclear genome sequencing run naturally yields an “off-target” mitochondrial coverage depth ranging from 100x to over 1,000x.
-
Sensitivity: This depth allows for the reliable detection and quantification of heteroplasmy levels down to approximately 1% to 5%. Any mutation existing below this frequency threshold generally falls into the baseline sequencing noise of standard WGS pipelines.
2. Targeted deep mtDNA Sequencing
-
Mechanism: This approach isolates or selectively amplifies the 16,569 base-pair mitochondrial genome using long-range Polymerase Chain Reaction (LR-PCR) prior to sequencing.
-
Sensitivity: By concentrating sequencing power exclusively on the mitochondrial genome, coverage depth frequently exceeds 10,000x to 100,000x. This extreme depth allows bioinformatic pipelines to confidently identify ultra-low frequency somatic mutations (micro-heteroplasmy) down to 0.1% or lower.
Technical Challenges and Confounding Factors
While technically feasible, accurate quantification of mtDNA mutations via sequencing must overcome two primary biological and methodological hurdles:
Nuclear Mitochondrial Segments (NUMTs)
Over evolutionary timescales, fragments of mtDNA have migrated and integrated into the nuclear genome, becoming pseudogenes known as NUMTs (Nuclear Mitochondrial DNA segments). Standard sequencing read-alignment tools can mistake these ancient, mutated nuclear fragments for true mitochondrial variants. Advanced bioinformatic filtering is mandatory to separate true mitochondrial reads from background NUMT sequences to prevent false-positive heteroplasmy readings.
Tissue Specificity and Mosaicism
The level of mtDNA mutations is not uniform throughout the human body. Somatic mtDNA mutations accumulate unevenly across different organs.
-
Blood (Liquid Biopsy): Easiest to sample, but rapidly dividing hematopoietic cells actively select against highly deleterious mtDNA mutations over time.
-
Post-Mitotic Tissues: High-energy, non-dividing tissues such as skeletal muscle, cardiac muscle, and cerebral cortex typically accumulate significantly higher levels of somatic mtDNA mutations with age.
-
Implication: A standard blood-derived WGS report may show 0% heteroplasmy for a specific mutation that sits at 40% heteroplasmy in the individual’s muscle tissue.
Relevance to Longevity and Geroscience
In the context of healthspan extension, mapping the accumulation of somatic mtDNA mutations provides a direct readout of mitochondrial decay.
Unlike nuclear DNA, mtDNA lacks protective histones and features less redundant repair mechanisms, leaving it highly susceptible to oxidative damage. While inherited mitochondrial diseases typically require a “biochemical threshold” of 60% to 90% heteroplasmy to manifest as clinical pathology, low-level age-related micro-heteroplasmy (sub-5% shifts spread across multiple loci) degrades electron transport chain efficiency, drives cellular senescence, and accelerates the energetic decline characteristic of biological aging.