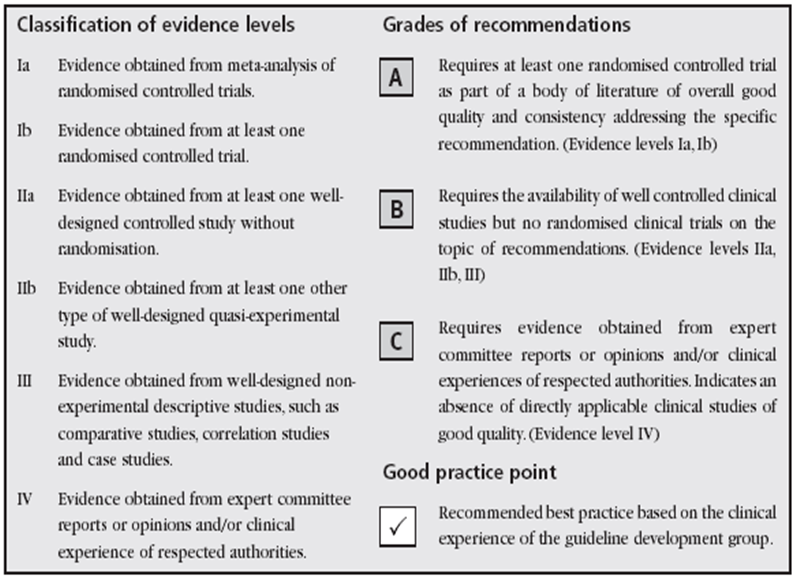
My favorite component of this site is the level of intellect and research that the members bring from all backgrounds. The discussion of how you make a decision to integrate a therapy option vs. not are great. Many involve intense back and forth with research articles that help support your decisions. My question is that when researching a subject relative to the topics on this site, what is your favorite place…Pub Med, NIA, YouTube ? Second, do you have a rational process to grade the information you find. The American College of Ob/Gyn use a grading system to evaluate levels of evidence that similar to many others that I have listed below.
4 Likes
I started out with Pubmed, but now I mainly use Google Scholar.
I try to find studies that have a large cohort, preferably humans, that are double-blind, long-term, etc.
5 Likes
Can I ask your back ground. You always have excellent input that is evidence based combined with common sense. At 80+ and doing so well, you become an expert in an area that does not have many ![]()
1 Like
Google first, pubmed is a terrible search engine.
I then go to pubmed for the papers as they link back often. But as you know, many (important) are paywalled. For that I use, sci-hub (@RapAdmin might not condone but haven’t been scolded yet). Failing that write the authors, if they respond, will send you the paper.
Very very often google will find obscure stuff that you’ll never find on pubmed. You have to try different search terms to really extract what you’re looking for, often missed first passes.
I don’t discount any study or reference per se, just absorb and filter for quality, journal, size, confounders, how close to target relevance, translatable, etc.
As to how to condense this into lifestyle intervention(s), well human trials data first and foremost. After that, interventions that have multiple beneficial pathways.
Peter Attia is a great reference because of his intellect, and he’s on the clinical front line treating people.
Other forums too.
3 Likes
I am a retired electrical engineer specializing in electronic design at the Department of Energy Remote Sensing Laboratory. Worked for EG&G, Lockheed Martin, and Defence Nuclear Agency.
https://www.nnss.gov/pages/facilities/RSL.html
1 Like
I love sci-hub and fully support Alexandra on her quest to provide easy access to all the world’s medical and biological research papers:
I just hope them success in the current trial in India so that they can continue their mission…
2 Likes
I use YouTube for ideas then usually a double check on pubmed. I also have a general overarching philosophy: I look for supplements that are metabolites and have a proven effect on athletic performance and supplements that have a proven effect on mitochondrial health, NAD-levels or autophagy. Rapamycin of course doesn’t fall into that category completely but it does have a lot of science
That is very impressive and make sense. Your posts are thoughtful and logical. Any thoughts on maximal effort exercise as you age? I have an athletic history and struggle between the thrill of competing with myself to improve performance vs. the potential harm of an all out effort.
@MAC Thanks for the response. Your post are always helpful and informative. I am not familiar with sci-hub, but excited to look into it. RCT are a great standard, but in the medical world translate into 100’s of millions if not billions of dollars. The insurance industry depends on this obstacle and hides behinds it support of evidence medicine to deny coverage from studies that do not meet this standards while many could possible benefit from intervention. Insulin resistance would be the most common example of this with 70% of Americans overweight or obese, but unless you are diabetic then treatment can be difficult to get covered. Appreciate your insights and posts!
Thank you for sharing and agree with the balance of enhancing with max performance that likely promote mTOR activation with Rapamycin that inhibits mTOR.
Its a pirate scientific paper distribution hub. The web address changes over time because companies are always trying to block them - but if the sci-hub.se address ever doesn’t work just search on “Current Sci-Hub domain that is working” or something like that - and you’ll find one that is functioning. They have pretty much all the scientific papers up until sometime in 2021 when the lawsuit in India forced them to put things on hold (they hope to win in India which would make things easier for them going forward).
And a list of active Sci-Hub Domains:
2 Likes
Well, here’s what happens when you’re old. You are old: you find it hard to believe you can’t do things you used to do. This week I felt really great on Wednesday and went to the gym, lifted max weights, and did 5 sets instead of my usual 3. So, I am still paying for it. Two semi-sleepless nights because of aches and pains. Went to the gym today and used the spa and steam room to try and calm things down so I can sleep tonight. So, bottom line, don’t over do the gym.
7 Likes
You do a great deal actually.
Yeah, it’s recovery time that’s rough. When I go hiking with my son , I can keep up for a day or two, but then I need a break, but he doesn’t.
Recovery time, that’s the rub. Is it mitochondrial function, endothelial function, stem cells, cardiac ejection fraction? I don’t know.
I do know that since rapamycin it’s gotten better.
4 Likes
I am impressed you are doing max weights. My ego liked the results, but my joints and tendons complained at night to the point of interrupting sleep and difficulty doing small tasks like putting on sock and shoes. The Rapamycin has helped me with recovery and I am guessing that its blocking some of hyper inflammatory reaction. I am trying to move to yoga to improve my flexibility and balance, but yoga is not in my wheel house of strong skill sets. I can put on my shoes and socks now. The main reason for the questions was hoping to pull from you journey lessons for me. I go to an Orange Theory gym now and they will occasionally have bench mark timed days - such as your fasted mile on a treadmill or your fastest time at a 500m row. The competitive side of me loves this. Breaking my record and seeing progress is right up my alley. My concern is the down side of maximal effort as we age and not being a stepping stone to a better performance, rather a stressor that breaks the body down or even accelerates that aging process.
You are about 23 years ahead of me, so I appreciate your insights since I would hope to doing as well as you!
1 Like
Mainly, I have had to back off aerobic exercises because my ankles are trash from years of playing tennis on hard courts and running on asphalt. I wasn’t genetically endowed with good ankles. If I had it to do over again I would skip hard court tennis as it seemed to bother me more than the running. At 81 I feel great until I attempt to do too much.
The thing about resistance training is I have never regressed. My hands seem to be a limiting factor now. I like to hang and stretch my spine but if I do it too much it causes pain in my finger joints and I develop “trigger finger” that takes days to go away. That is what happened to me last time I overdid the weights. One of the negative things about feeling great at an older age is attempting to do too much. Rapamycin makes me feel younger than I am.
4 Likes
As an inventor, creator of IP, and business owner, it’s obvious sci-hub is a pirate/thief, without debate. She lost judgment in the US, never showed up to defend herself, has never paid.
https://www.nature.com/articles/nature.2017.22196
Stealing copyrighted knowledge and sharing without consideration, is illegal.
Creating and publishing high quality manuscripts costs money, this needs to be covered. But why are they “gatekeepers” of this knowledge?
Having said that, these publishers are running a cartel, charging exorbitant access fees. There needs to be a new paradigm/model for sharing publicly funded research, as the current “status quo” is not working. Governments and other entities who provide public funding should step in and deem the research in public in interest. The knowledge created is far too important to limit universal access.
5 Likes
Hard court tennis is brutal on ankles/knees. As a daily 3-4km runner, I need to minimize wear and tear for the long haul. I specifically avoid hard surface running for the reasons you allude, and run indoor treadmill. If I happen to run outdoor hard surface, my lower limbs are quite stressed post run. I feel nothing on my treadmill. That’s not to say the pounding is not having an impact on my knees/cartilage, but I’m betting on the reward/risk equation re all cause mortality risk reduction.
I have a funnel for my information…
I follow a wide variety of science news media, and whenever I see a new target or compound linked to longevity I enter it into Google Alerts so that I can easily follow the science around that topic as it progresses, and automatically get updates.
Here is a sample of the 100 plus terms I have in my Google Alerts listing:
Actually - I’ve copied my entire list from my Google Alerts, in case anyone is interested. Here (below) is the full list of topics / key words I get notified on anytime there is something new on the web published on any of these terms - all longevity related.
Please - if anyone has suggestions on other compounds, therapeutics that may be interesting to follow - please post them here. I’m always looking for new additions…
- Lef1 factor
- “Interventions Testing Program” (ITP)
- 15-PGDH
- 17‐α estradiol
- 3-hydroxyanthranilic acid lifespan
- 3,4-dimethoxychalcone
- acarbose
- Age-related macular degeneration
- Alfatradiol
- Alkahest
- alpha-ketoglutarate (AKG)
- AlphaCT1
- altos labs
- Amazentis
- apigenin
- Artemisia scoparia lifespan
- Astaxanthin
- Atentiv
- autophagy
- Canagliflozin
- David Sabatini
- Digoxin obesity
- Dimethyl Fumarate lifespan
- dr alan green rapamycin
- epicatechin
- Epirium
- ergothioneine
- executive function childhood stress
- FGF skin aging
- fibroblast growth factor aging
- Flow Neuroscience
- Gdf11
- Gemfibrozil aging
- GTP-3
- Harold Katcher
- Hevolution
- Hevolution foundation
- Hydrogen Sulfide lifespan
- IMYu
- Intra-Cellular Therapies
- irisin exercise
- ISRIB
- John Overington MDC
- Juvenescence
- kat7 gene
- Longevica
- Longevity Science Foundation
- Lumateperone
- lymphoid enhancer-binding factor 1 (LEF1)
- metolazone
- montelukast aging
- MOTS-c age
- mTOR inhibitor
- Mycophenolic Acid lifespan
- MYSM1
- n-methylglycine
- navitor pharmaceuticals
- NIA interventions testing program ITP
- NIA ITP
- nicotinamide mononucleotide
- nicotinamide riboside
- Nir Barzilai
- nugenics
- Oisín Biotech
- PDLH rejuvant
- Prkar2a
- Rapalogs
- Rapamycin
- Rapamycin Acarbose lifespan
- REVEL PHARMACEUTICALS
- Rhodiola
- sarcosine
- Senisca
- Senolytic
- senomorphic
- Sestrin
- SGLT2
- sirolimus
- Sodium phenylbutyrate lifespan
- Sodium phenylbutyrate sleep
- spermidine
- stem cell CNS
- Sulindac lifespan
- Tony Wyss-Coray
- torin2
- UNITY Biotechnology eye
- UNR844 presbiopia
- Urolithin A
- VCAM1
- vcam1 age
- verteporfin anti-scar
- verteporfin scarring
- Yamanaka factors
- YTHDF2
- ZGN-1062
For the most interesting compounds (e.g. rapamycin, canaglilfozin, etc.)
I also set up alerts for new papers on the topic - in Pubmed and BioRxIV
Podcasts/Youtube:
I follow sporadically the podcasts we list here on our site to get inside perspectives on the research via interviews with the scientists doing the work:
When the new research / compound/therapeutic process is identified, the next step is Pubmed or contact the author to get the paper (Sci-hub was great until it stopped being updated a year or so ago).
As far as a rational process to grade the information - the key, rough guideline I use to rank the study is a well designed, controlled study (obviously in humans much more valuable than mice), number of people /subjects in trial, improvement (in lifespan/or other measure) significance, and source /academic group for the paper, and funding source for the paper (Industry-funded papers are obviously less reliable, more biased, and negative results hidden more, than in NIA/NIH funded studies). And really, in the past decade, the NIA ITP program with its three-way study on each compound is just head and shoulders above all the individual, un-replicated study results - so they have become the unquestioned leader in terms of studies on longevity compounds and are so much more valuable because of this.
For new compounds to try personally, the calculations get much more complex… and Rapamycin is a good example. Rapamycin had been on my radar since it first started showing results in drosophila back in the early 2000s, so I followed it as the mouse studies came out and also looked good. But, the perceived risk around it was too great until I saw the 2014 Mannick Paper where they tested rapalogs in healthy population and had good results. At that point, the risk was well quantified and as people started using it, the risk/reward profile changed to one I was comfortable with.
The side effect profile was pretty benign, and dosing was easily modified over time to adjust any potential side effects.
As a point of comparison - Testosterone supplementation is something that has been around for decades, but I’m aware of no significant lifespan benefits, in clinical studies in any mammals. I’m not aware of any academic groups that have done lifespan tests. So while it might provide some perceived healthspan benefits, as long as I am healthy, athletic and active, I prioritize the compounds with strong clinical evidence with lifespan AND healthspan benefits over anything with just healthspan benefits. I want to keep my stack as simple as possible, and I realize that “more” could very easily mean “less” in terms of adding different compounds or supplements or treatments.
Its interesting, but for drugs that are already FDA approved, the adoption seems like it will be relatively quick in terms of use by longevity enthusiasts… so we are seeing drugs with good clinical / FDA history and NIA ITP results (like acarbose and canagliflozin) moving quickly into use (admittedly by the fringe of society interested in significantly longer/healthier lifespans).
This is especially true as the drugs go generic and prices decrease dramatically - for example at $600/month Canagliflozin in the USA is probably more than most people want to pay, but when you can buy the same drug for $60/month from India - the adoption rate goes up quickly.
So - I see the Mannick paper of 2014 as a good model for FDA drugs that might boost longevity, but which have a perceived higher risk of concerning side effects. Once its proven reasonably well in healthy people, then adoption will start rising quickly.
mannick2014Everolimus.pdf (354.2 KB)
10 Likes
Wow! This is so good and I will have to read it a few times to take it in small bites, but wow! So thoughtful and methodical. Thank you!
FDA approved drugs make it easier to use due to the off label use criteria.
Longevity is important to me, but I have decided that Health span holds higher value in my determination of my personal approach. Also, my 401k may not last long enough if I live too long:) . Testosterone had dramatic health span improvements for myself and many of my patients, but I do not recommend anyone start it if they do not have symptoms issues that it may help or continue treatment if they do not see a quality of life improvement to balance the risks.
1 Like
Awesome! Thank you for taking care of this for the benefit of all of us.
1 Like