A level of 6 ng/mL is immunosuppressive. Specifically, we see it used in this range to suppress organ rejection and when it goes lower than 3 ng/mL (in combination with other drugs) we start seeing organ rejection rates go up. Done as a sole drug for organ transplant
A short term study of 6 individuals for 8 weeks is unlikely to get adverse effects. So yes, someone wanting to do this for 8 weeks to potentially get these benefits - probably relatively safe. Doing this for years … I’d expect to see problems.
Here is a summary of blood levels that are actively immunosuppressing (and note it is <6 for several indications) based upon indication:
1. Kidney Transplantation (Renal Transplant)
Regimen / Scenario
Time Post-Transplant
Target Sirolimus Trough (ng/mL)
Notes
With Calcineurin Inhibitor (CNI) (e.g., tacrolimus or cyclosporine) – “CNI + sirolimus”
First 3–6 months
4–8
Most common early strategy
>6–12 months
3–7
Lower if stable
CNI-free / avoidance (sirolimus + MMF + steroids, or belatacept-based)
First 3–12 months
8–14 (often 10–12)
Higher exposure needed without CNI
Maintenance (>1 year)
5–12
CNI minimization or conversion (late switch from CNI to sirolimus)
After conversion
8–15
Especially in chronic allograft nephropathy or malignancy risk
2. Liver Transplantation
Regimen
Target Trough (ng/mL)
Notes
With tacrolimus (early or minimization)
4–8 (first 3–6 mo) → 3–6
Very common in many centers
CNI-free (sirolimus-based primary)
8–12
Less common, higher toxicity risk
3. Heart Transplantation
Regimen
Target Trough (ng/mL)
Notes
With CNI (proliferation signal inhibitor addition)
4–10
Often added for CAV prevention or renal sparing
Everolimus more common than sirolimus in heart tx, but if sirolimus used
5–10
4. Lung Transplantation
Regimen
Target Trough (ng/mL)
Notes
Usually everolimus preferred; if sirolimus used with CNI
3–8
For BOS prevention or CNI minimization
5. Pancreas or Simultaneous Pancreas-Kidney (SPK)
Regimen
Target Trough (ng/mL)
Notes
With low-dose tacrolimus
4–8
CNI-free
8–12
6. Lymphangioleiomyomatosis (LAM)
Indication
Target Sirolimus Trough (ng/mL)
Reference
Pulmonary LAM (TSC-associated or sporadic)
5–15 ng/mL (most guidelines aim for 8–12 or 10–15 in practice)
MILES trial (NEJM 2011), ATS/JRS guidelines 2017, and 2023 updates
Goal
Reduce VEGF-D, stabilize or improve FEV1, reduce chylous effusions
Just FYI, make sure not to do that with Rapamycin. The pills have a special coating which is needed to survive the stomach and make sure they are absorbed. (The PEARL trial kinda failed because they had much lower absorption than expected due to using some proprietary formulation rather than just using the real deal).
Tnx for the tip. Unfortunately I can’t take that advice. I’ve blood tested cyrolimous a dozen times with experiments of co-adjunivants; grapefruit extract, berberine, grape seed, peperine… (all affect same pathway +/-) and have seen mid 20’s but I have to take 12++ mg plus the adjunivants to get that high. My last test was a paultry 9 ng/dl. So I just take 2x that amount. ;( Some day we will have a target blood level from trials to know what to shoot for / not to exceed…
I’m forced to adjust rapa mg till I see decent blood values due to my personal absorption and protocol limitations. Tnx though!!! Curt
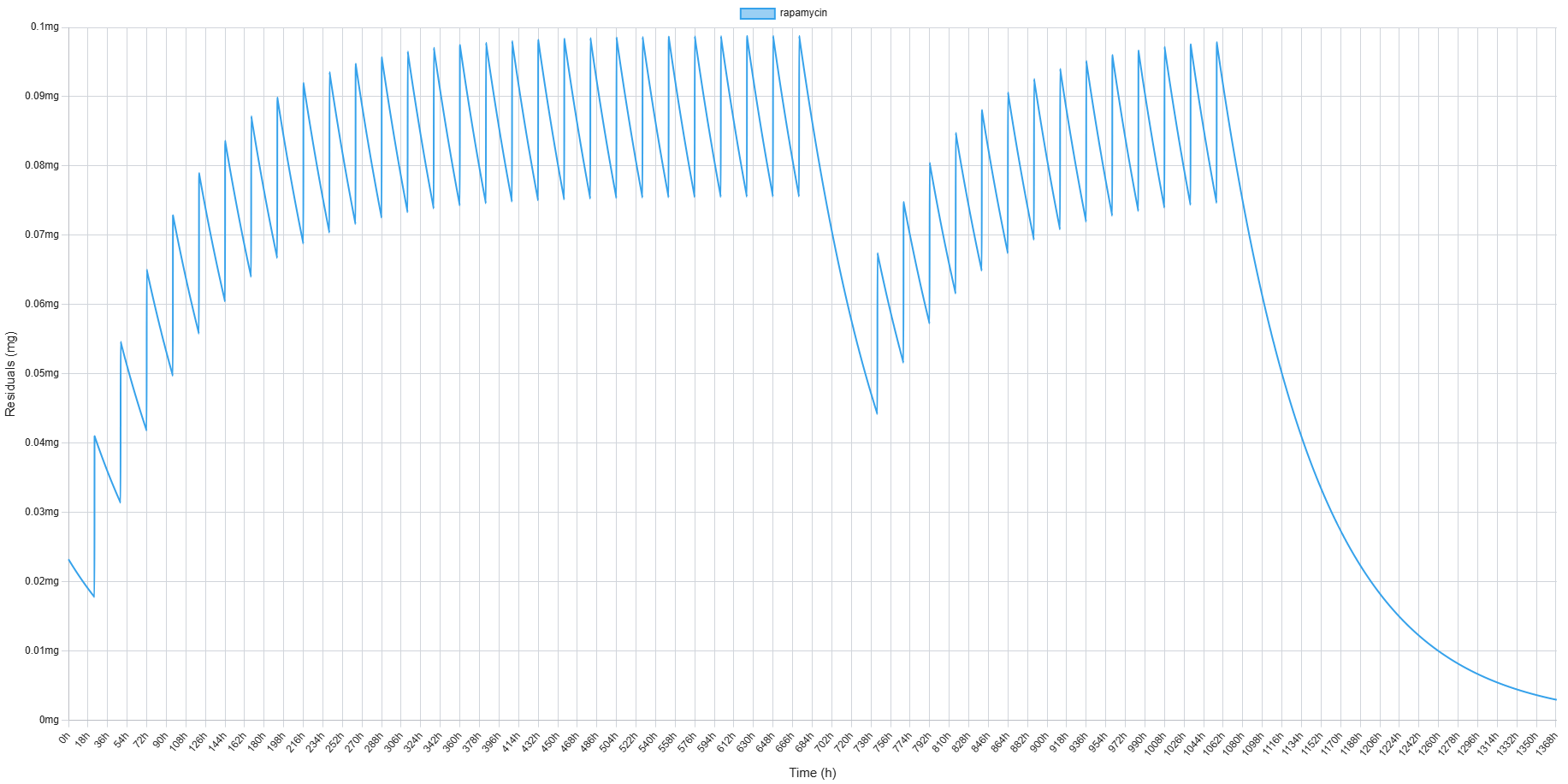
Steve, with your protocol are you measuring your trough level? Do you take into consideration daily decay factor (usually 0.707 but mine for example is 0.95). If yours is ≈ 0.707 (i.e., 70.7% remains each day) and it accumulated for 28 days and you have only a 2 day break, which means you are accumulating a lot.
According to the studies on this 1mg per day dose schedule, the accumulation level is not a big concern.
Since we have been doing this for close to 3 months now, we have not experienced any of the obvious “issues” other people have experienced with the peak and trough method. We had been doing an every 2 week x 6mg with GFJ for nearly 2 years before switching to this and neither of us had any issues with that protocol either.
Does it mean you don’t measure your levels and just follow the protocol in the study? The study followed that protocol only for 8 weeks. So no wonder they did not show much accumulation or immunosuppressive effects.
1mg is exactly what is prescribed to me for kidney transplant and it does accumulate which leads to immunosuppression enough to keep transplanted kidney. I track my numbers daily. When trough reaches 5 I have a break till it falls to 2.5 - 3 ng/mL and then start again to reach approximately 5.
why did you switch to 1 mg daily from the 6mg every other week w/GFJ? You would need more rapamycin on the once a day protocol. roughly 30 pills v.s 12 per month. (I do 6mg w GFJ every 21 days)
One of the latest research posts has the subjects taking 1 mg for 4 months and no immunosuppressive effects. See below excepts:
Rapamycin exerts its geroprotective effects in the ageing human immune system by enhancing resilience against DNA damage
Low-dose rapamycin reduces markers of senescence and DNA damage in humans in vivo
Taken together, our data so far show that age-related immune subsets exhibit features of DNA damage, cell senescence, and mTOR hyperactivation, and that human ageing is accompanied by increased mTOR activity across all immune cell types (Figure 7d-e). We have further demonstrated that treatment with low-dose mTOR inhibitors improve survival and reduce markers of senescence and DNA damage in human T cells treated with a genotoxic agent outside of the body. Such findings are important but require in vivo data before they support further clinical action. We therefore assessed whether rapamycin treatment impacts on immune cell DNA damage and senescence in vivo in humans, analysing PBMCs from participants of a single-blind, placebo-controlled trial (NCT05414292), in which older male volunteers received either 1 mg/day rapamycin (n=4) or placebo (n=5) for 4 months (Figure 8a). While the primary endpoint was to assess changes in muscle mass and protein synthesis, we aimed to assess features of immunosenescence in PBMCs isolated at several timepoints throughout the trial.
After 8 weeks of intervention, the concentration of rapamycin in the blood reached an average of 3.24 ± 1.81 nM in the treatment group (Figure S5a), i.e., within the same order of magnitude as the doses used in our in vitro experiments (10 nM). To address concerns of immunosuppression by rapamycin, the white blood cell count was assessed at 8 weeks; there were no significant differences in leukocyte counts in the blood over the initial 8-week rapamycin treatment period, and between rapamycin treated and placebo controls, suggesting that this low-dose rapamycin treatment regimen was not immunosuppressive (Figure S5b).