What is the optimal BMI for the elderly or anyone? I am starting to have second thoughts about this.
I started rethinking this when I saw some information about the winner of the most recent PGA tournament. This guy weighs less than I did,145 lbs, he is the same height that I was when I was a senior in high school, and I was pencil thin.
“The “obesity paradox” in the elderly—the observation that being overweight (BMI 25–30) is associated with lower mortality than being “normal” weight (BMI 18.5–25)—is a highly debated topic in gerontology. While many large-scale observational studies support this paradox, a growing body of rigorous research suggests it is a methodological “mirage” caused by significant confounding factors.”
When these factors are properly controlled, the “optimal” BMI for longevity in older adults often shifts back down toward the lower end of the normal range (BMI 20–22)."
“Sarcopenia vs. Adiposity: A common theory is that the elderly need “more fat” to survive the “wastage” of acute illness (like pneumonia). However, critics argue it isn’t the fat that is protective, but the muscle mass. A BMI of 20 consisting of healthy muscle (low sarcopenia) is statistically superior to a BMI of 27 consisting of high body fat (sarcopenic obesity).”
“The increased risk of mortality observed in underweight people could at least partly be caused by residual confounding from prediagnostic disease.”
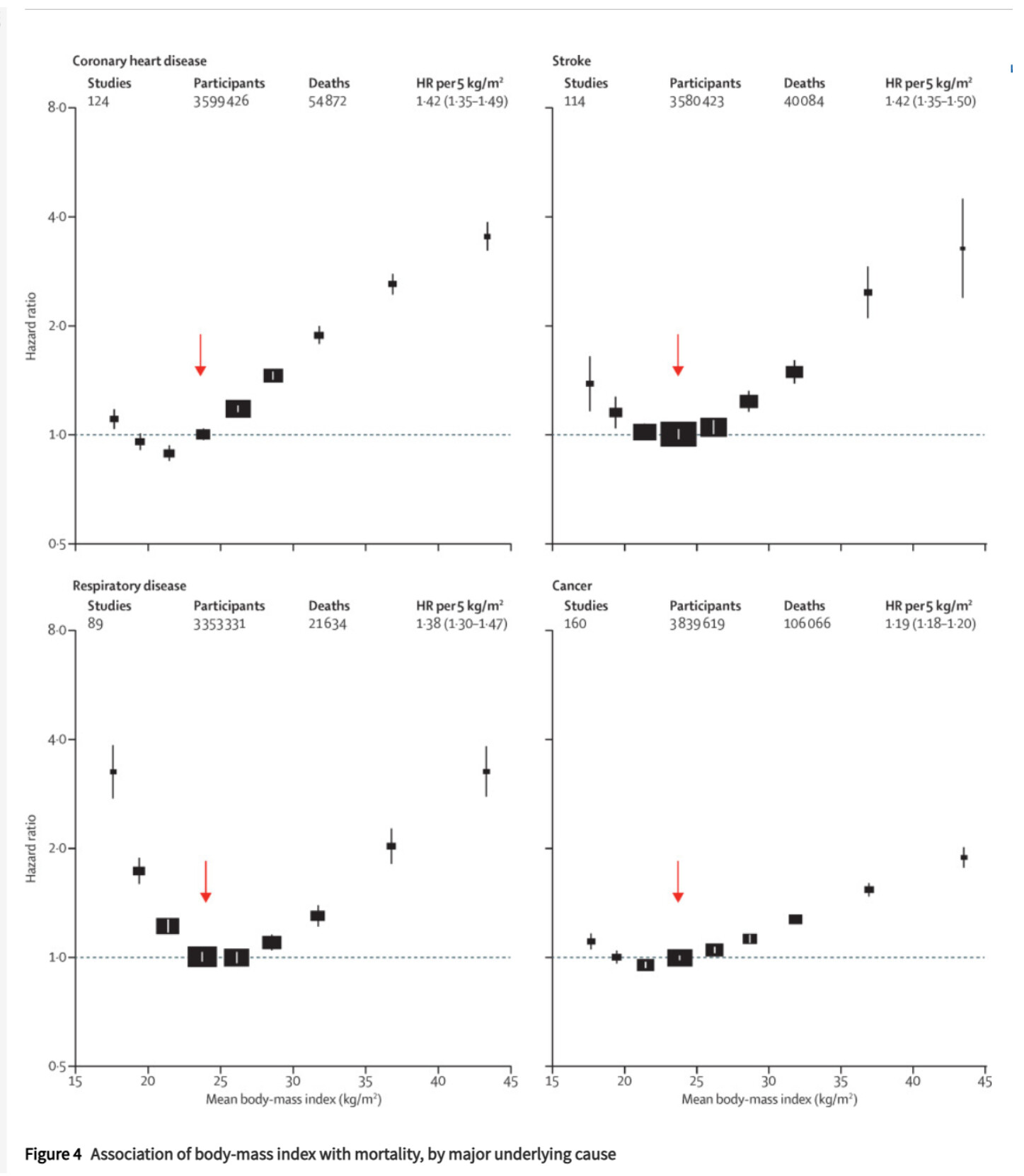
BMI and all cause mortality: systematic review and non-linear dose-response meta-analysis of 230 cohort studies with 3.74 million deaths among 30.3 million participants
One note of caution. Bhatia is genetically South East Asian, from the Indian subcontinent. Folks from that region have a very specific relationship with BMI. They get overwhelmingly more diabetes at shockingly low BMI (like 22). They tend to have a LOT more visceral fat. They’re famous for the TOFI phenotype (Thin Outside Fat Inside). They have vastly more CVD at lower BMI than folks from a Northern European stock (Charles, you are mostly Anglo, no?).
In other words, when it comes to BMI, if you are not SE Asian, looking at the SE Asian phenotype you are not likely to learn much.
All that said, BMI and the elderly is an interesting subject. For general health, low BMI is advantageous. That said, it has downsides, particularly for the elderly. One is bone health - much greater rates of osteoporosis. You really need to crank up the exercise including impact, get a bit more protein (past age 65). The other thing is something that has been seen repeatedly in ERs. Folks with some subcutaneous fat reserves do better in surgery and in illness - it’s a kind of additional “reserve” which is protective. So, if you plan to get all the advantages of low (or very low) BMI, make sure you exercise with impact, get enough protein and avoid visits to the ER, get all your vaccinations in and try not to break bones or get into accidents. Ironically, that’s kind of what we see in CR’d animals - they do live longer, but that’s in lab conditions where their living conditions are superior, there are fewer pathogens, fewer accidents etc. - out in the wild that would be a different story.
Bottom line, if you can protect yourself from external trauma or infections, lower BMI will give you a greater lifespan and healthspan.
What do you get when you treat an independent variable as if is were well-measured and continuous, regressing it against precision dichotomous variables – dead/alive, coronary event/no event, T2D/no T2D – when in fact it’s a lossy, systematically biased proxy for several distinct, differently behaving and sometimes polar opposite, underlying constructs. Whatever you get, it isn’t science.
Sarcopenia and Osteopenia is no joke for the elderly (edit: or anyone for that matter). One fall is all it takes. I lost my dad that way.
I wonder if tesamorelin would be an acceptable drug for the elderly? Seems like it’s being researched for that purpose atm.
AI summary:
Tesamorelin is being investigated for its potential benefits in elderly individuals, particularly related to age-related declines in growth hormone (GH) and insulin-like growth factor-1 (IGF-1), a condition sometimes referred to as “somatopause.”
Visceral Fat Reduction: Clinical studies show that tesamorelin significantly reduces visceral adipose tissue (VAT), the dangerous fat around abdominal organs, in older adults. This effect is observed without affecting subcutaneous fat and is linked to improved cardiometabolic health.
Cognitive Function: Research indicates that tesamorelin may improve executive function, attention, planning, and verbal memory in healthy older adults and those with mild cognitive impairment. These benefits are thought to stem from restored GH and IGF-1 levels, which support brain health and synaptic plasticity.
Metabolic and Cardiovascular Health: Tesamorelin has been shown to reduce carotid intima-media thickness (cIMT), a marker of atherosclerosis, and lower triglycerides and C-reactive protein (CRP)—key indicators of inflammation and cardiovascular risk—without causing insulin resistance.
Mechanism and Safety: As a growth hormone-releasing hormone (GHRH) analog, tesamorelin stimulates the body’s natural pulsatile GH release, avoiding the risks associated with direct GH supplementation. It is generally well-tolerated, with mild side effects such as injection site reactions, joint pain, and temporary increases in blood glucose (which normalize with long-term use).
FDA Approval and Use: While approved by the FDA for reducing visceral fat in adults with HIV-associated lipodystrophy, its use in healthy elderly individuals for anti-aging or longevity is considered off-label and not yet FDA-approved. Long-term use (e.g., over 6 months) may be needed to maintain benefits.
There are genetic differences with respect to BMI beyond Indian subcon.
Insurance treats all Asians the same when it comes to risk of high BMI. I haven’t looked hard but I suspect Indian subs are more sensitive than Chinese.
SE asia always makes me think of Vietnam and I’m not old enough to think that way.
Africans can probably tolerate a higher BMI then Europeans.
So hopefully all these studies are genetically restrictive but I have a feeling they are not.
I remember a bit part of the potential paradox is that people tend to lose weight from a variety of chronic illness that also cause mortality. So you AD patient that isn’t eating, has a BMI of 20 from 28 earlier has a high mortality. I feel like the paradox is still there when this was corrected for.
My general guess based on experience is that low BMI isn’t great when you get infections or have to recover from emergency surgery. So to me there is a downside but whether that overwhelms the CV or other risk, IDK. Sure muscle mass is important but doesn’t provide as much calories as good old fashioned fat.