There has to be a way to integrate all the data into one’s biobank database AND use it to retroactively update published correlations (and diagrams used by the data, esp if time-series-based) for ALL clinical trials that one is involved in.
Ha - good luck with this one.
This is a huge issue in the USA, lots of different (incompatible) EMR systems, very difficult to transfer data between them, or aggregate information from them and the independent labs we work with, the health monitoring devices we use daily… to the best of my knowledge nobody has solved this type of problem.
And, lots of incentive on the EMR company side to lock in the data to increase “switching costs” for hospitals and patients so as to lock customers/patients into their systems for the long term so as to maintain their revenue stream.
And, lots of incentive on the EMR company side to lock in the data to increase “switching costs” for hospitals and patients
Explain more?
I recommend you ask your healthcare systems that your medical records are in what EMR system they are using (to start with). Then you’d need to find the aggregator that can pull in that data, plus your lab work, etc.
My understanding, from working in the digital health field (startups doing health-related startups like EMRs, etc.) there is a basic level of data interoperability that has been specified by the govt. - basically like .cvs, or tab delimited files, in spreadsheets. But this is extremely basic. But then the EMR companies have vastly extended on their file formats over the years with new features, etc. So its not like you can just export your EMR record from one system, and import that file into another system. My understanding is that these software systems have become, in effect, very proprietary in their data format. Sure - you can technically get your healthcare records exported and given to you on a pile of CDROMS - but good luck doing anything with it.
The EMR system market in the US is pretty fragmented - so in effect, silo’d healthcare data.
This is a strategy frequently used in data oriented businesses to minimize competition, and to stop your customers from going to other competitors:
Here are the top EMR systems companies and their market shares:
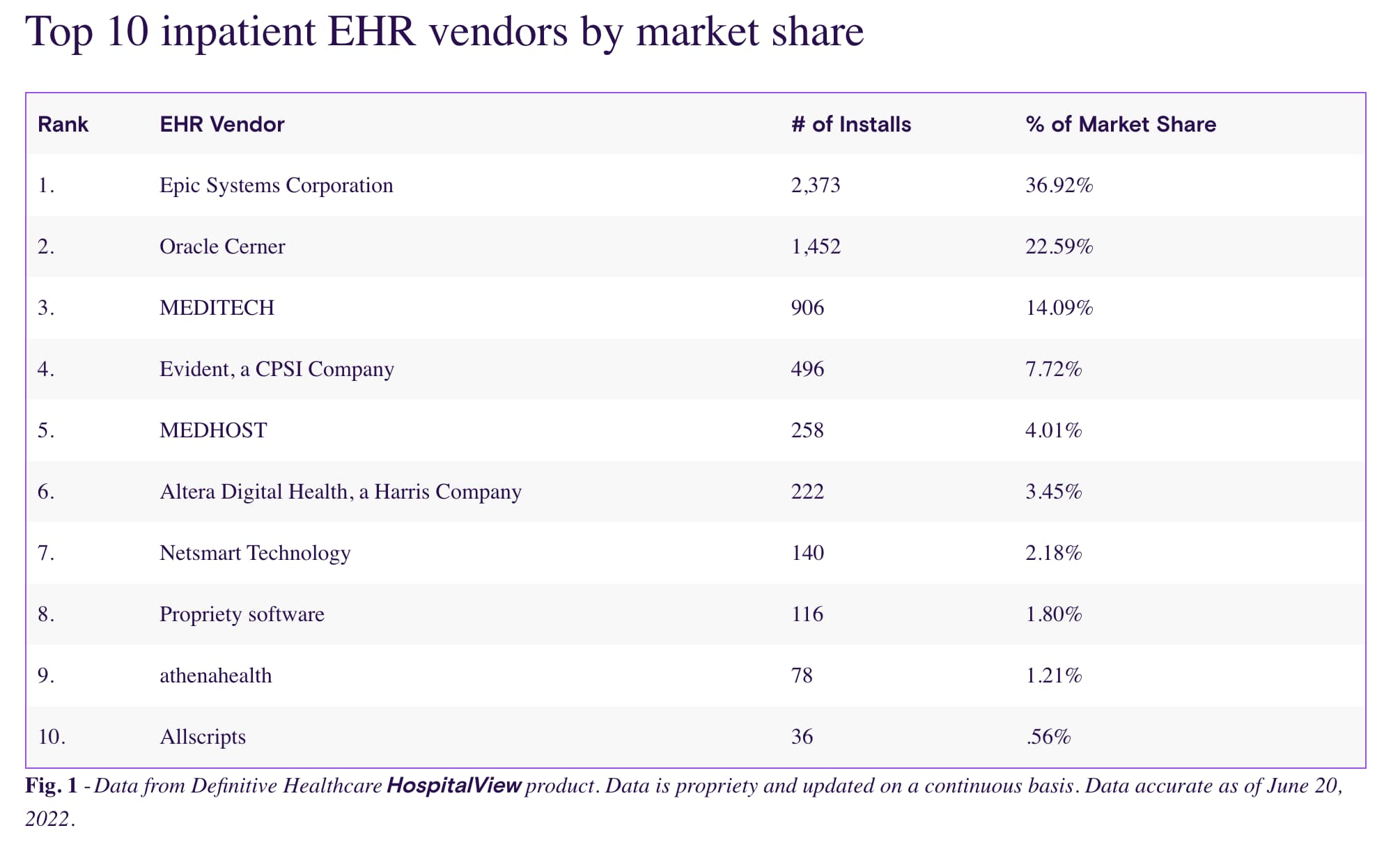
Source: https://www.definitivehc.com/blog/most-common-inpatient-ehr-systems
My concierge physician compiles all my medical records and testing results in one place. He has admin staff to handle records requests.
If you know the EHR system most likely used in the nearby ER and other tricks - there is a “backdoor” way in some of the most common EHR systems to avoid delays in records requests depending on the EHR system by allowing access automatically. Not well known. Same with clinical trials. It is actually possible to automatically show up in some cases. But it’s like bug bounty systems in cybersecurity - you need to know the system architecture and where to look to “hack” the system to actually find any meaningful ways to bypass anything.
Navigating the system efficiently is important but most people won’t realize system complexity until they hit barriers again and again, then get run into a loop.
Sounds like you’re just starting to realize how bad it is. This is partly why healthcare “AI” has tons of barriers on top of regulatory and I’ve seen way too much incredibly uninformed thinking. The data can get incredibly messy - so “garbage in, garbage out” for “AI” training. I had to request changes to my medical records a few times to avoid insurance issues because of human errors ie some random scribe puts in vaping use under tobacco use when I never mentioned it nor do I ever use any nicotine products.
Another example is it is extremely common to see patients who have meds on the EHR they aren’t taking on the list such that a “med rec” is important but few staff wants to do such record cleaning work. I’ve seen enough records that are a hot mess such that things that should have gotten done don’t get done. Although uncommon, treatments get delayed and it is possible to have dangerous issues from poor medical records. Add in the literal “public health crisis” from physician burnout according to the Harvard T.H. Chan School of Public Health and you compound issues.
I try to keep my records as clean as possible via another “backdoor”. Even the “best doctors in the world” can’t give efficient care if they are reading faulty data, let alone some “AI” fed faulty data for training.
Yes - as a doctor, I think you have some idea about the issues.
@AlexKChen , some reading if you want to learn more about the issues… perhaps people are or have been working on some areas of this since I last looked at it:
1 Like
I also happen to be familiar with clinical informatics and have direct experience working briefly at an EHR startup that got acquired. Anyone can try coding with FHIR data standards vs the older ones based on XML-only.
As you probably already know, the probable solution is somewhere along the lines of an HIE, but as you mentioned no incentives. There are tons of incentives to keep data siloed. Not only that, I’ve tried almost every single major EHR system with a significant market share. Most are incredibly unintuitive and look outdated. They don’t have the same incentives to update user-friendliness as much - pretty much most of them just rather pay trainers to visit clinics and hospitals instead of making their software easier to use. The EHR is more designed for billing than any other function.
I’ll also mention I’m quite familiar with which EHR systems that have a history of software bugs and compatibility issues. This can lead to orders not being transmitted and sometimes, death, albeit rare. The contracts hospitals sign have “gag orders” and a lot of this never sees the light of day. Hospitals tend to side with the EHR systems. Doctors who call out the technical errors on EHR systems just end up in a blame game - EHR just blames the docs on human error.
Try identifying EHR related adverse events database FDA MAUDE some time and you’ll see how bad it is to even compile all the patient safety screw-ups. Add in that not required to report unlike medical devices. Good luck trying to fix it - the major EHR vendors are tied to politics heavily - ie athenahealth and Jonathan Bush and maintain healthy profit margins to keep this going with oligopoly lock-in on the hospital side. Like everything else in healthcare as you mentioned - incredibly fragmented and it’s hard to navigate without knowing all the complex “operational legalese”.
The main way for an individual to “beat the system” in this scenario is to know the system better than the EHR companies themselves and legally exploit and “hack” all the possible ways to patch up integration/interoperability issues on your own if you know where to look.
1 Like
Which gives a good reason to know your own data and its limitations.
" nam et ipsa potestas est"
Properly translated as “Knowledge in itself is power”
In the UK, Canada and elsewhere - the EMR situation is quite different. it would be interesting to know if people in countries with universal healthcare and standardized healthcare record systems are able to get access to their data in a way that is helpful in longevity tracking.
I am in the UK. I don’t think anything about the NHS facilitates access to this sort of information. The only useful information I have obtained is outwith the NHS. That does not mean that it is impossible that the NHS would provide useful information, however.
My take on EMR’s, having used several:
If I ranked them based on usability, it would be the same rank as market share above.
There is little communication between systems, although that has begun to change.
As far as communication, more important than the EMR, is the health care system using it.
EMR are not optimized for using clinical data. They’re optimized for billing.
It is difficult to get outside information into the EMR.
1 Like
I don’t know what formats you’re talking about. I just take copies of documents and save them as readable pictures or pdf files on my laptop. For blood tests, I get them in different formats from different places I have had them, but usually it’s on paper so I take them and input all the results in a single excel sheet to keep them all in one place and easily comparable in terms of the date of the tests. That’s a quite a bit of hassle to take the results and input it into excel but it’s the only method that works.
I also have a summary spreadsheet for blood results. It is essential to enable review.
1 Like