This decreased my homocysteine from 15 to 8, for what it’s worth, but I’m testing methylcobalamin now only.
I’ve gotten my levels down to 7.4 and am happy with that.
Eric Verdin commented in Attia’s podcast that NMN and NR raised his homocysteine from ~8 to ~ twice that. It quickly reversed when he quit.
Methylfolate, Methyl B12 and TMG are essential in longevity stacks IMO, for the remethylation of homocysteine.
These supplements might be beneficial by themselves but not for their homocysteine-lowering effect. See: Parkinson's disease - #914 by adssx
Yes, I was just responding to the above off-topic chatter about lowering it. Should have been more clear.

Prescription drugs of all types increase it …
Fibrates…
Short answer: yes, especially after protein-heavy meals. Not a crisis, just normal biochem being dramatic.
Here’s the deal, fast and useful:
What rises: Total homocysteine (tHcy) in blood.
Why: Meals with methionine (an amino acid abundant in meat, eggs, some dairy) temporarily flood the remethylation/transsulfuration pathways. The “methionine load” test in clinics literally exploits this to see how well your methylation handles a surge.
How much:
- Mixed, normal meals: usually a small bump (often ~1–3 μmol/L above your fasting baseline).
- Very methionine-rich bolus (think: huge steak, methionine-load test): can be a larger spike.
Timing: Starts rising within 2–4 hours, often peaks around 4–8 hours, then drifts back toward baseline by 8–12+ hours. This is why labs want a fasting draw.
Who spikes more: People low in folate, B12, B6, or with sluggish kidney function, hypothyroidism, or certain meds can show bigger and longer spikes.
What blunts it:
- TMG (betaine) taken with or near a protein-heavy meal can flatten the post-meal rise.
- Adequate folate/B12/B6 status.
- Pair protein with vegetables/greens (folate) instead of going full “protein comet.”
- Don’t chug multiple strong coffees alongside a huge methionine hit if you’re chasing a pristine post-meal curve.
Bottom line: Meals, especially high-methionine ones, do cause a temporary homocysteine bump. Your fasting number is the one to track for long-term risk. If you’re actively trying to damp post-meal spikes, keep B-vitamins on point and consider TMG 500–1000 mg with big protein meals.
I’m here to figure out if the AI from Good labs is correct in advising me to take methylated folate.
My homocysteine levels jumped from 6 to 11.
There is a chance it’s not my folate levels because I was very recently experimenting with NAD subq injections (not a high dose and only a handful of times), but due to my CVD, I’m stopping out of an abundance of caution.
Also,
I had the Vibrant Micronutrient Test done last Jan, and it and my doc said my folate numbers were good, and due to my WFPB diet, that tracks…. But….
After uploading those results in Good Labs, their AI told to me part of my problem might be my low folate (a human confirmed it). After some googling, it seems that the Vibrant test uses a lower optimal range, but because the ranges don’t seem to be universally accepted, I wanted to double check and get everyone’s thoughts.
It showed my serum folate was >20 ng/ml, and Vibrants ref range said anything over 4.6 ng/ml is good…
It showed my RBC folate was 239 ng/ml, and their ref range shows that anything over 95 ng/ml is good
However…
I was told RBC is a more important measure, and 239 ng/ml shows I’m low and might be contributing to my higher homocysteine. Goodlabs ref range shows it should be above 333. Health Matters IO says their optimal range is 499 - 1504 ng/mL.
Before I add yet one more supplement to my huge stack, I just wanted to see if the hivemind knows better than what I’m reading. ![]() Thank you!
Thank you!
Also, while I have you, how long should I wait for a new homocysteine lab to show a change?
Do you take TMG? That would be my next step with homocysteine, because your folate numbers don’t look bad, I doubt that’s the issue (assuming decent B12 levels). You can get Bulk Supplements TMG and do 1.5g - 3g daily, dissolves pretty good in tea and the like (I take it in my morning drink mix with taurine, FOS, blueberry, cranberry extracts, all in green tea). The TMG can also help with exercise. Worth a try.
Thank you Cronos!
I always get warnings about my B12 being too high, so I’ll order TMG right now!!! Thx for the tip on getting the powder and sharing your source.
Appreciate this, thx
This meta shows slightly higher dose of TMG to be effective, but I found lower doses to work just as well:
Betaine supplementation decreases plasma homocysteine in healthy adult participants: a meta-analysis
If you’re using creatine 2g or more per day, you’ll cut your methyl group demands by another 40%. So together with TMG and methylated vitamin B you should have more than enough methyl groups. I take all of that in the morning and then glycine in the evening to pick up the “surplus”.
While positioned as possibly insignificant in this paper, it is worth looking at the effect of TMG on TC and LDL-C
Yes, but as always, any drug/supplement/intervention should not be looked at in isolation, but in the whole context of the body in a particular individual (personalized precision medicine). It is my understanding that Beth is under powerful LLT, and in this context any impact of TMG on lipids is likely going to be trivial. As always, measure. Do an intervention, measure the impact of before and after. Not every intervention is going to be suitable in any given individual. TMG is one option to explore.
RobTuck, thank you for pointing that out!
And yes, CronosTempi, you remember correctly, my lipids are extremely well managed (repatha, etc)
So, I received my tmg last night and excitedly took 3grams…
And in being overzealous (patience is not my strong suit), today I took 6grams.
My thinking was if that was in the study, I’d try it for a week or two just to get a kickstart on lowering my homocysteine, and then I’d lower it for more of a maintenance dose until I got new labs…
Oh, mistakes were made!!!
I never ever get nauseous, but this did it, and I even threw up my lunch,
*sitting here in shame until this wears off.
Nausea is not a frequent reaction, but it’s better to work up to it, and even if taking 6g, don’t do it all at once, split the dose in two, 3g morning and evening.
I’ve heard Chris Masterjohn say that r5p is the right way to take riboflavin. Like you I’m heterozygous and confused about MTHFR. I just take the homocystex:
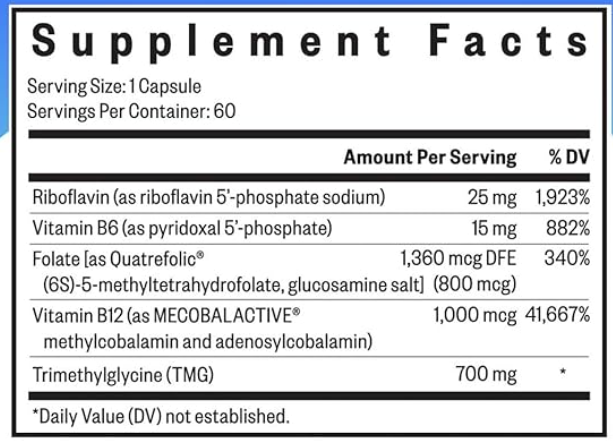
It sounds like you’re doing everything right. The folate chills me out, kind of like lithium. This Supp is a pleasure for me to use. expensive though.
Aww, thanks for the reply @Bicep! I ended up deleting my question when I realized I was too confused about the topic to even ask it clearly, so I really do appreciate the recommendation