Green mentions 2 weeks to allow rapa 62 hr half life to decrease blood level then re-dose.
Green mentioned on top of the desire to suppress mtor, he used the words: benefit of rapa is also due to a differential between blood level now vs post dose. I add the words; spiking, pulsing. VS continuously keep mtor supressed. Just attempting to bring Dr Green comments here. Best to all.
Wondering if there is any research or anecdotal information about rapamycin and resistance exercise. It seems pretty clear that while rapamycin supplementation reduces muscle wasting (sarcopenia) in aging mice, it also blocks protein synthesis. Since I do both cardio and resistance training, I wonder if one should schedule resistance training at 1. the end of the week after taking sirolimus or 2. during the washout vacation period? See
Interesting question regarding the differentiated issue of cardio and resistance training. I also do both - biking for an hour 3 or 4 times a week, and strength training 2 or 3 times a week for 45 minutes or so. I don’t change my schedule based on my rapamycin intake - but I do expect different results.
From what I’ve read, in the first few days after rapamycin intake you likely have much higher mTOR inhibition - so muscle growth after workout will likely be minimized. But - I think it was discussed by Peter Attia and Matt Kaeberlein in their recent podcast, or perhaps another one - generally the theory is just keep exercising on your regular schedule, and you’ll get some benefit. When mTOR is highly inhibited your workout will help to maintain your muscle and help prevent muscle wasting (due to lack of mTOR) - and then when the mTOR inhibition has receded - i.e. later in the week, you’ll get more gains.
On the broader issue of strength training / muscle building and rapamycin use - did you see this previous conversation?
I initially worried about rapamycin inhibiting muscle growth. However, something I read recently (frustrated that I didn’t record source) said that taking rapamycin periodically will enhance muscle growth because the periods of autophagy will enable the anabolic phase to work better.
thank you. after doing research and thinking about rapamycin for 2 years, i just took my first dose this morning. i went straight to 5mg of rapamune, figuring that this is probably the minimum effective dose, and can go to 6mg next week. i have done 3 day fasts several times, so i figured that i have some experience with inhibiting mtor the natural way. other then a small headache the first hour (very likely a placebo type of effect), i feel totally normal. i also put on a glucose monitor for the next two weeks to see if anything changes from my norm.
I just checked my ketones, as rapa seems to be somewhat of a fasting memetic, and is supposed to increase utilization of fatty acids. i was at 0.7mmol which is fairly low and may just be a result of not really eating much carbs today. (on a 3 day fast, i can hit on day 3 4-6mmol)
Oh wow, I jsut had some carbs (not a lot), about 11 hours after taking 5mg, and my glucose response was MUCH higher (around 40 points higher then where it should be after what I ate) the normal. Based on this I will be extra careful with carbs when at peak dosage, and maybe add back metformin or take acarbose when eating a carby meal.
I would highly recommend that people take a look at their post prandial glucose levels after dosing rapa
As a Type 1 diabetic, I keep a close eye on my blood glucose, and I have noticed no discernible effect of rapa. In fact, my blood glucose may be slightly lower during the first couple of days after dosing rapa.
i am not diabetic, but i find that its lower when on rapa if not eating carbs or at night its much flatter then normal. but when eating carbs, the response it more extreme, but comes down quickly.
i would assume that its similar to in a fasted state. when fasting and there are fatty acids at the muscles, they dont take up glucose as well (the glute 4 transporter get inhibited from intaking glucose into the muscle). the most likely reason is to preserve the glucose for the brain.
In terms of ApoE testing, even if you were ApoeE4 positive is there any data on this being a problem with rapamycin? Do most patients see increases in lipid markers and is the risk of this higher than potential benefits of rapamycin?
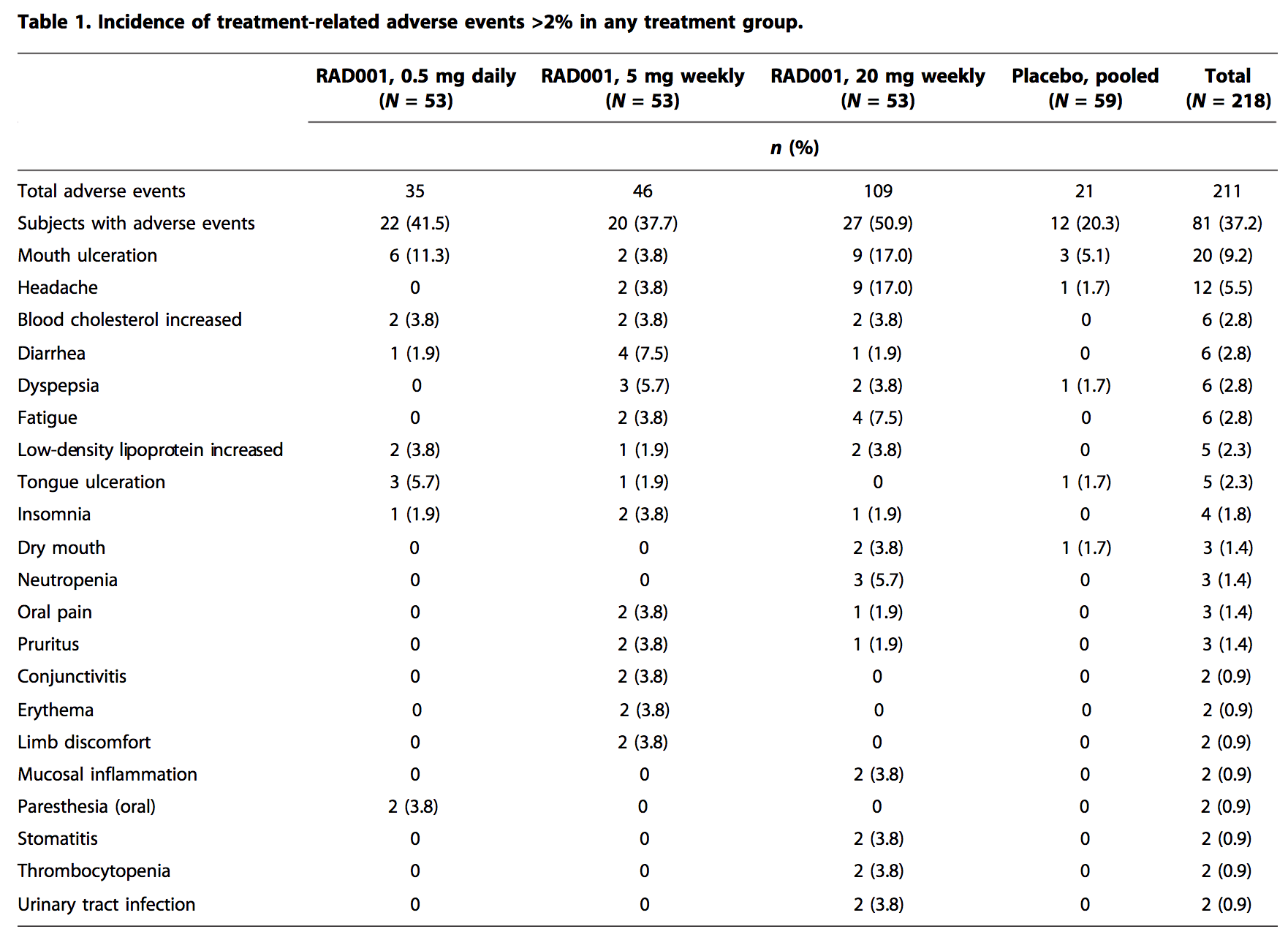
The difference between Evirolimus and Sirolimus is profound. Evirolimus is much weaker and thus requires more the block Tor 1 than Sirolimus does. So the Mannick study of 20 mg weekly would take a lot less Sirolimus to obtain same results. These rapalogs were really developed for everyday usage to prevent organ transplant rejection. Sirolimus with it much longer 1/2 life is really a much better drug for longevity purposes and it also gives you a much bigger bang for your buck.
Also, these dosages depend on your age, the older you are the stronger your Tor signal is and you need more SIrolimus to inhibit it. So a Dr. Attia taking 6 mg weekly at 48 yo., is not compartibile to a 70 yo taking the same 6 mg. weekly. 70 yo would get much less benefit and would need to increase his weekly dosage to get a compartible benefit. Now Dr. B taking 20 mg bi-weekly is probably more of a better guide. His age is probably around 63 yo.
Where do you get your information on the need for higher dose at older age? Seems to be at odds with some results. For example, Dr. Green unequivocally states that at 72 years of age he did 6 mg/week and it worked in many ways in obvious health benefits for him. It’s a very important point and you may be right. But need to know if this is your conjecture or has some other basis in fact. Dosing is one of the big unknowns with this drug.
I’m not sure that is accurate. On the Peter Attia / Lloyd Klickstein interview, Lloyd suggested the equivalent dose was a little lower for sirolimus vs. everolimus (20% to 30% or so) - see here.
And Matt doesn’t see much difference in the two drugs:
I was Dr. Green’s 2nd patient in April 2017 so have been following ever since. He was taking 20 mg every 2 weeks last I heard. The reason for the higher dose is we have learned a lot in the last 4 years on dosing. Also, Dr. Blagosklonny who is really the Godfather of rapa is also taking this dose and thinking about going to even higher dose. They both wait long enough for rapa to trough before next dose. They are elderly, and Tor signal increases with age. The thinking is swinging to the believe that higher doses get past the brain/blood barrier into the hippocampus part of brain and inhibt Tor 1 there. Many believe this is where ageing is regulated. We may never get a trial in humans on dosing. Who is going to pay for it? I personally follow the “experts” on my dosing. Dr. B has stated in his dosing paper that one can increase dose until you get side-effects then back off with no limit. Every person is different