The New 2026 season of Buck podcast “We’re not getting any younger…yet” launches tomorrow! 1st episode features Harvard geneticist George Church, one of the most provocative thinkers in the longevity field. Available wherever you get your podcasts. Subscribe - don’t miss single episode!

2 Likes

1 Like
Tony Wyss-Coray: Rejuvenating the Brain

Gemini Pro AI Video Summary
Executive Summary
This dialogue between Dr. Eric Verdin (CEO of the Buck Institute) and Dr. Tony Wyss-Coray (Stanford University) explores the evolution of geroscience from foundational “young blood” experiments to the current frontier of organ-specific proteomic clocks. The conversation transitions from the historical context of heterochronic parabiosis—the surgical joining of young and old mice to share circulation—to the practical application of these findings in human medicine through therapeutic plasma exchange (TPE).
A central thesis presented is that aging is not a monolithic, synchronized process across the entire body. Instead, individual organs age at different rates. Wyss-Coray argues that measuring “biological age” for the whole person is insufficient for clinical intervention; instead, clinicians must measure organ-specific age to treat pathologies before they manifest as irreversible disease. By utilizing high-throughput proteomics (measuring thousands of proteins in the blood), his team has identified “organ-specific” protein signatures that leak into the circulation. These signatures allow for the calculation of an “Age Gap”—the deviation between chronological age and the biological age of a specific organ.
Specifically regarding neurodegeneration, the discussion challenges the notion that the “Amyloid Hypothesis” has failed, suggesting instead that interventions have simply been administered too late. Proteomic markers, such as the brain-specific aging signature found in the UK Biobank study, can predict Alzheimer’s risk up to 15 years before clinical symptoms emerge. The researchers highlight a 20-fold difference in Alzheimer’s risk between those with the “youngest” vs. “oldest” brains and note that a “young brain” correlates with an 80% reduction in overall mortality.
The dialogue concludes with a vision for preventative medicine 2.0, where biannual proteomic profiling provides a “dashboard” of organ health, enabling personalized lifestyle or pharmacological interventions (e.g., targeting the immune system or gut barrier) decades before traditional diagnostic thresholds are met.
Bullet Summary
- Heterochronic Parabiosis: Early mouse studies proved that young blood circulation can rejuvenate muscle stem cells and improve cognitive function in older mice.
- Systemic Environment: Aging is driven significantly by the systemic environment (blood), not just intrinsic cellular decay.
- Detrimental Factors: Factors like Eotaxin (CCL11) and Beta-2 Microglobulin (B2M) accumulate in old blood and actively impair brain function and neurogenesis.
- Rejuvenation vs. Dilution: Benefits of plasma exchange likely come from both adding beneficial “young” factors and diluting “pro-aging” inflammatory factors.
- Organ-Specific Aging: Organs age at different rates; a person might have a “young” heart but an “old” brain.
- Proteomics over Epigenetics: While epigenetic clocks are popular, proteomics (measuring proteins) provides a more direct readout of current functional biology and “organ suffering.”
- The “Age Gap”: The difference between your actual age and your organ’s biological age is a more powerful predictor of disease than chronological age.
- Brain Age & Alzheimer’s: A proteomic “old brain” signature predicts Alzheimer’s onset 15 years in advance.
- Predictive Power: Individuals with the youngest brains in the UK Biobank study showed an 80% reduction in 15-year mortality.
- The Amyloid Reconciliation: Amyloid and Tau are critical, but anti-amyloid drugs fail because they are given to patients whose “arteries are already obliterated” (advanced disease).
- Immune-Brain Axis: Brain health is deeply tied to systemic immunity; activating the immune system can modulate amyloid pathology.
- Gut-Brain Connection: The gut holds 50% of the immune system; gut barrier permeability (leaky gut) is a primary driver of systemic inflammation affecting the brain.
- Early Intervention: The future of medicine involves treating “organ aging” 10–20 years before a diagnosis like Parkinson’s or Alzheimer’s.
- Scalability: Current proteomic platforms can measure 3,000 to 7,000 proteins in a single plasma sample with high reproducibility.
- Direct Feedback: Unlike genetic testing (fixed risk), proteomic clocks provide a “live” feedback loop to see if diet, exercise, or drugs are actually working.
Claims & Evidence Table (Adversarial Peer Review)
| Claim from Video | Speaker’s Evidence | Scientific Reality (Best Available Data) | Evidence Grade (A-E) | Verdict |
|---|---|---|---|---|
| Young blood rejuvenates old brain/muscle. | Cites Rando/Wyss-Coray parabiosis studies in mice. | Replicated in multiple labs; Nature 2014. However, human “young plasma” trials for AD (PLASMA study) showed safety but lacked robust efficacy. | D (Animal) / B (Human-Small) | Plausible/Translational Gap |
| Proteomic clocks predict Alzheimer’s 15 yrs early. | Nature paper (Dec 2023) and UK Biobank data (50k people). | Supported by Oh et al., Nature 2023. Highly accurate in large cohorts but requires prospective validation in clinical settings. | C (Cohort/Observational) | Strong Support |
| Eotaxin (CCL11) causes brain aging/fog. | Wyss-Coray lab research; Michelle Monje studies on chemo-fog. | Villeda et al., 2011 identified CCL11 as a pro-aging factor in mice. Human correlation exists, but RCTs blocking CCL11 are pending. | D (Animal/Mechanistic) | Speculative (Animal Data) |
| Young brain = 80% lower mortality. | UK Biobank analysis (3,000+ proteins). | Statistical correlation in Nature 2023. Remarkable hazard ratio, but “young brain” may be a proxy for overall systemic health. | C (Cohort) | Plausible |
| TPE/Plasma Exchange reverses aging clocks. | Verdin mentions a study using “a number of clocks.” | Kiprov et al., 2022 showed TPE reduces inflammatory markers and shifts some clocks, but “reversal” is a heavy term; “modulation” is more accurate. | B (Human RCT/Pilot) | Plausible (Emerging Data) |
Actionable Insights (Pragmatic & Prioritized)
Top Tier (High Confidence)
- Prioritize Gut Barrier Integrity: Focus on diet (high fiber) to maintain the gut-vascular barrier. Since 50% of the immune system is in the gut, “leaky gut” directly facilitates the entry of inflammatory factors that accelerate brain aging.
- Early Biomarker Screening: If available via boutique clinics (e.g., Grail, Fountain Life, or specialized proteomic providers), monitor organ-specific markers (Liver, Kidney, Brain) rather than just “whole body” biological age.
- Manage Systemic Inflammation: Since brain aging is driven by systemic factors (Eotaxin, B2M), interventions that lower chronic systemic inflammation (exercise, sleep, weight management) are neuroprotective.
Experimental (Risk/Reward)
- Therapeutic Plasma Exchange (TPE): For those with significant inflammatory burdens or early signs of cognitive decline, TPE (diluting “old” plasma) is an emerging clinical protocol with a high safety profile, though currently expensive and not yet standard of care for longevity.
- Proteomic “Age Gap” Testing: Utilize services that measure the “Age Gap” to identify which specific organ system is the “weakest link” in your longevity profile.
Avoid
- Late-Stage “Cures”: Do not rely on “reversing” neurodegeneration once clinical symptoms are advanced. The dialogue emphasizes that by the time Alzheimer’s is diagnosed, the “arteries are already obliterated.” The focus must be on the 15-year window before symptoms.
Technical Deep-Dive
The mechanism discussed centers on Proteomic Organ Mapping. This utilizes the fact that nearly every organ sheds a small percentage of its proteome into the blood. By cross-referencing blood proteins with GTEx (Genotype-Tissue Expression) data, researchers identified proteins that are highly enriched (e.g., 4-fold higher) in specific organs.
- Machine Learning Models: LASSO or similar regression models are trained to predict chronological age based on these organ-specific proteins in healthy populations.
- Deviance Analysis: When an individual’s protein levels suggest they are 70 years old while they are chronologically 60, they possess a +10 year Age Gap.
- Pathophysiological Leaking: The “leaking” of organ-specific proteins (like troponin in the heart or transaminases in the liver) is not just a sign of acute damage but a chronic indicator of the cellular senescence and tissue remodeling associated with aging.
Knowledge Gap: We do not yet know if aggressively lowering a specific “old” protein (like CCL11) in humans will yield the same cognitive gains seen in mice. Most data remains correlational (Level C).
1 Like
Ana Maria Cuervo: Cellular Recycling

Full transcript here: Cellular Recycling
This analysis evaluates the discourse between Dr. Eric Verdin and Dr. Ana Maria Cuervo regarding the role of Chaperone-Mediated Autophagy (CMA) in proteostasis and longevity.
I. Executive Summary
The core thesis presented by Dr. Cuervo posits that aging is fundamentally a failure of proteostasis—the cellular quality control factory responsible for protein folding, localization, and degradation. While various forms of autophagy exist, the discussion focuses on Chaperone-Mediated Autophagy (CMA), a selective degradation pathway Dr. Cuervo discovered. Unlike macroautophagy (the non-selective “Pac-Man” mechanism), CMA utilizes the LAMP-2A receptor as a “hook” to translocate specific damaged proteins containing the KFERQ motif into lysosomes for recycling.
The primary argument is that CMA efficiency declines universally with age due to the loss of LAMP-2A receptors. Dr. Cuervo presents compelling pre-clinical evidence: genetically restoring LAMP-2A in systemic mouse models not only preserved organ function (liver, brain, muscle) but also extended both healthspan and lifespan. Furthermore, the development of small-molecule CMA activators has shown efficacy in mitigating proteotoxicity in animal models of Alzheimer’s (AD), Parkinson’s (PD), and Macular Degeneration.
From an analytical perspective, while the biological mechanism is robust, a significant translational gap remains. The transition from genetic “proof-of-concept” in mice to pharmacological intervention in humans is fraught with safety risks, particularly regarding the potential for CMA over-activation to facilitate cancer cell survival—a “double-edged sword” typical of autophagy pathways. The discussion also touches on lifestyle “geroprotectors,” suggesting that fasting windows (8+ hours), sleep, and exercise serve as physiological triggers for CMA. However, the exact titration of these inputs for human CMA induction remains speculative and lacks high-resolution clinical validation. The summary conclusion is that CMA represents a high-priority target for “clean house” therapeutics, provided that tissue-specific delivery and safety profiles are established in upcoming Phase I trials.
II. Insight Bullets
- Proteostasis as Factory Quality Control: Cellular health depends on the precise timing, shaping, and shipping of proteins; failure leads to “garbage” accumulation and cell death.
- CMA Selectivity: CMA is the only autophagy pathway capable of discriminating between “good” and “bad” proteins using chaperone proteins (Hsc70) and specific biochemical hooks.
- The LAMP-2A Bottleneck: The LAMP-2A receptor is the limiting factor in CMA; its decline is the primary driver of age-related proteostatic failure.
- Systemic Rejuvenation: Genetic restoration of LAMP-2A in aged mice results in systemic improvements in cognition, motor function, and metabolic resilience.
- Neurodegenerative Target: Neurons are uniquely vulnerable to CMA failure because they do not divide, meaning they cannot dilute protein aggregates through cell division.
- Macular Degeneration: CMA activation in the retinal pigment epithelium shows potential for slowing vision loss, a condition currently lacking effective restorative treatments.
- Autophagy vs. Starvation: Autophagy is an energetic survival mechanism that recycles damaged parts into fuel (amino acids) during nutrient scarcity.
- mTOR and Nutrient Sensing: Rapamycin activates autophagy by inhibiting the mTOR sensor, “tricking” the cell into a fasting state even when nutrients are present.
- Macroautophagy vs. CMA Kinetics: Macroautophagy activates within 2–6 hours of fasting, whereas CMA requires longer windows (approx. 8–12 hours) for maximal induction.
- The “Clean House” Synergy: Improving one driver of aging (autophagy) creates a healthier environment for others (DNA repair, mitochondrial function), leading to exponential benefits.
- Sleep and the Glymphatic/Autophagy Link: Deep cleaning in the brain occurs during low-activity states (sleep), which is disrupted by late-night snacking and blue light.
- Hormetic Stress: Exercise creates “micro-damage” that serves as a necessary signal to trigger cellular recycling pathways.
- Social Connectivity: Preliminary data suggest that psychological stress inhibits autophagy, while positive social interactions may have a stabilizing effect.
- Future Diagnostics: Longevity medicine will likely shift toward “proteostatic profiling” at age 50 to customize autophagy-enhancing protocols.
- Small Molecule Licensing: Small-molecule CMA activators have been licensed for biopharma development, signaling a move toward human clinical trials.
III. Adversarial Claims & Evidence Table
| Claim from Video | Speaker’s Evidence | Scientific Reality (Current Data) | Evidence Grade | Verdict |
|---|---|---|---|---|
| LAMP-2A restoration increases lifespan/healthspan. | Cuervo’s mouse studies (to be published). | Genetic LAMP2A overexpression in mice improves protein homeostasis and liver function. Zhang et al., 2021 | Level D | Plausible (Translational Gap) |
| 8-hour fasting window triggers CMA. | Theoretical kinetics of autophagy. | Human data on CMA-specific induction via fasting is sparse; most markers track macroautophagy (LC3-II). Hofer et al., 2022 | Level E | Speculative |
| Social interaction improves autophagy. | “Studies not as many as I’d love” (Cuervo). | Social isolation stress is linked to autophagy dysregulation in rodent models, but human evidence is purely observational. Xiao et al., 2024 | Level D | Speculative |
| CMA activators mitigate Alzheimer’s/Parkinson’s. | Pre-clinical mouse models of AD/PD. | Small molecules (e.g., CA77.1) enhance CMA and reduce tau pathology in mice, but human safety is unverified. Bourdenx et al., 2021 | Level D | Strong Support (Pre-clinical) |
| Metformin activates autophagy. | Mentioned as a geroprotector mechanism. | Metformin activates AMPK, which indirectly promotes autophagy, but primary longevity effects may be glycemic. Kulkarni et al., 2020 | Level B/C | Strong Support |
IV. Actionable Protocol (Prioritized)
High Confidence Tier (Level A/B Evidence)
- Moderate Aerobic Exercise: Minimum 150 minutes/week to trigger metabolic stress and general autophagy signaling.
- Circadian Alignment: Maintain 7–9 hours of sleep. Use blue light blockers/limit electronics 2 hours before bed to prevent inhibitory signals to the brain’s “cleaning” phase.
- Glycemic Control: Prevent chronic hyperinsulinemia (via diet or Metformin where clinically indicated), as high insulin levels are a potent inhibitor of autophagy.
Experimental Tier (Level C/D Evidence)
- Extended Fasting Windows: Aim for a 12–16 hour fast (e.g., 8 PM to 12 PM) to potentially reach the 8+ hour threshold required for CMA-specific induction.
- “No Snacking” Policy: Adhere to Dr. Cuervo’s “grandma’s rule”—avoiding inter-meal caloric intake to prevent the reactivation of mTOR/nutrient sensors.
Red Flag Zone (Safety Data Absent)
- Unregulated Autophagy Stimulants: Avoid “longevity” supplements claiming to be CMA activators until human safety data (Phase I) regarding cancer risk is published.
- Chronic Severe Caloric Restriction: Risk of sarcopenia and immune suppression may outweigh the benefits of autophagy in older populations (>70 years).
V. Technical Mechanism Breakdown
The discussion identifies two primary pathways for protein degradation:
- Macroautophagy: * Mechanism: De novo synthesis of a double-membrane vesicle (autophagosome) that engulfs cytoplasmic bulk (organelles, aggregates).
- Regulation: Strongly inhibited by mTORC1 (activated by amino acids/insulin) and activated by AMPK (activated by low energy/ATP).
- Chaperone-Mediated Autophagy (CMA):
- Mechanism: Recognition of the KFERQ-like motif by the heat shock cognate protein Hsc70.
- Translocation: The Hsc70-substrate complex binds to LAMP-2A (Lysosome-Associated Membrane Protein 2A) on the lysosomal membrane.
- Multimerization: LAMP-2A multimerizes into a translocation complex, allowing the protein to unfold and enter the lysosome for degradation by acid hydrolases.
- Pathology: In aging, LAMP-2A is lost from the membrane, leading to the accumulation of “toxic” proteins like alpha-synuclein (Parkinson’s) and tau (Alzheimer’s).
The current clinical trial landscape for the small-molecule CMA activators mentioned by Dr. Cuervo
The landscape for Chaperone-Mediated Autophagy (CMA) therapeutics is transitioning from academic “proof-of-concept” to formal industrial development. As of early 2026, while systemic “longevity pills” are not yet in Phase III, specific targeted applications and the first-in-class small molecules have reached critical regulatory milestones.
I. Pipeline & Clinical Status (2025–2026)
The primary vehicle for Dr. Cuervo’s translational work is Life Biosciences, which holds the exclusive license for CMA-activating technologies from the Albert Einstein College of Medicine.
1. Small Molecule Activators (CA77.1 and Derivatives)
- Status: Late Pre-clinical / IND-Enabling.
- Mechanism: These compounds (including CA77.1 and its predecessors like AR7) function as RAR-alpha antagonists. They stabilize the LAMP-2A receptor on the lysosome membrane, preventing its age-related degradation and effectively increasing the “hooks” available for protein recycling.
- Current Focus: Recent data (published late 2025) confirms these molecules successfully restore synaptic protein levels and reduce neuronal hyperactivity in aged mouse models. Clinical entry for neurodegenerative indications (Alzheimer’s/Parkinson’s) is anticipated following the completion of current toxicology and safety profiles.
2. The “Lupuzor” Exception (P140)
- Status: Phase III (Lupus).
- Note: This is currently the most advanced “CMA drug,” but with a reverse mechanism. It attenuates (inhibits) CMA in specific immune cells to prevent the presentation of self-antigens in Systemic Lupus Erythematosus (SLE). It serves as a clinical benchmark for the safety of modulating the CMA pathway in humans.
II. Strategic Distinctions in Aging Platforms
It is critical to distinguish between the different modalities currently being pursued by Life Biosciences and similar firms:
| Modality | Lead Program | Primary Indication | Status (March 2026) |
|---|---|---|---|
| Epigenetic Reprogramming | ER-100 (OSK Gene Therapy) | Optic Neuropathies (NAION/Glaucoma) | FDA IND Cleared (Jan 2026); Phase I/II enrollment active. |
| CMA Activation | CMA-Activator Platform | Alzheimer’s, Parkinson’s, Hematopoietic Stem Cell Rejuvenation | Pre-clinical (Advanced); translational funding from ADDF. |
| Mitochondrial Uncoupling | DNP Derivatives | Metabolic Health / Nash | Early Clinical / Exploratory. |
III. Emerging Safety & Adversarial Data
The “Double-Edged Sword” mentioned in Phase 1 has seen increased scholarly attention in 2026:
- Pro-Tumorigenic Risk: Research confirms that many cancers hijack CMA to degrade tumor suppressors (like p53) and survive in nutrient-poor environments. Systemic CMA activators must prove they do not accelerate existing undiagnosed micro-tumors.
- Tissue-Specific Toxicity: New studies (March 2026) indicate that over-activation of CMA can exacerbate acute kidney injury by promoting ferroptosis (iron-dependent cell death) through the degradation of Ferritin (FTH1).
- The “Seizure” Guardrail: While CMA activation reduces hyperexcitability in AD models, the titration must be precise; complete loss of CMA leads to calcium dysregulation and seizures, suggesting that “more” is not always better.
IV. Summary Verdict for the Analyst
The CMA Activator platform is currently the “dark horse” of longevity medicine. While Life Biosciences’ Epigenetic Reprogramming (ER-100) has taken the clinical lead in 2026, the CMA small molecules represent a more scalable, oral intervention.
Mar 4, 2026: The Future of Research on Aging is Now; Eric Verdin, MD

Executive Summary
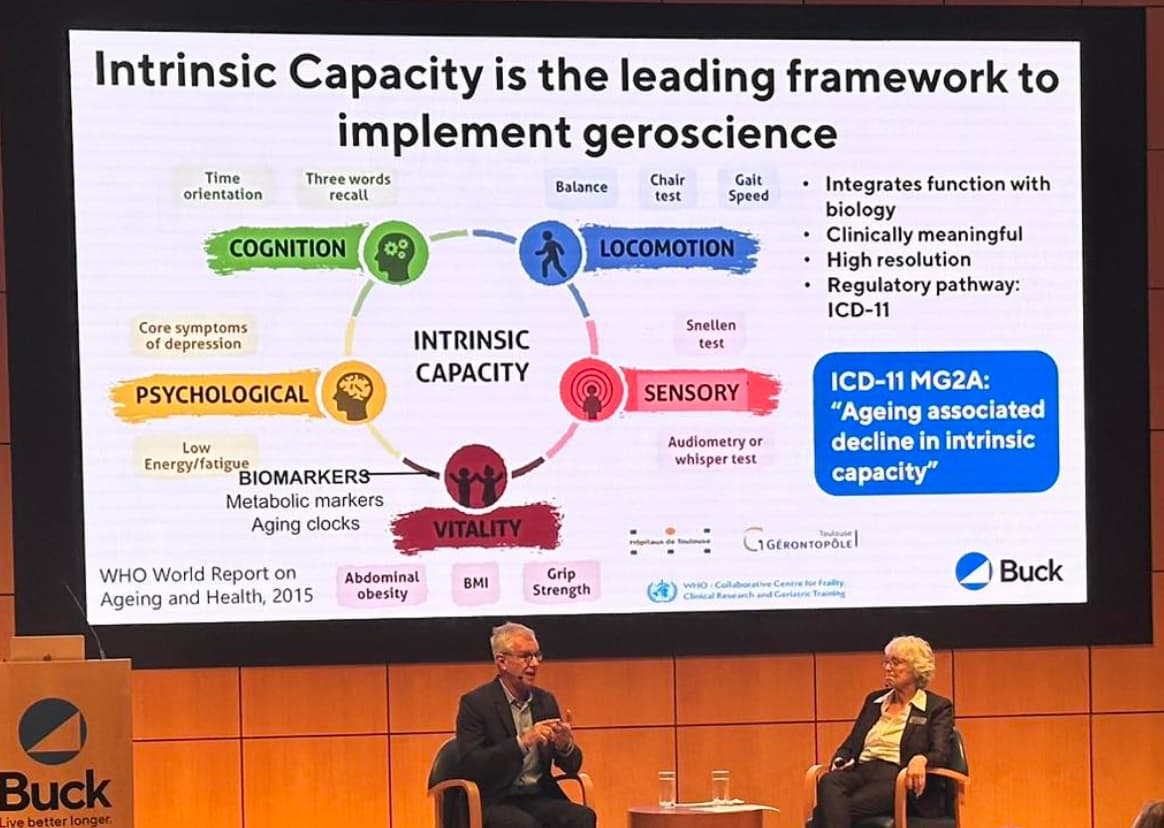
The core thesis presented by Dr. Eric Verden at the Buck Institute centers on a critical shift in geroscience: transitioning from molecular-only biomarkers (e.g., epigenetic clocks) to Intrinsic Capacity, a functional assessment framework focused on locomotion, sensory perception, and cognition. This paradigm shift aims to provide the FDA with validated surrogate endpoints for aging, potentially unlocking pharmaceutical investment in a field currently sidelined by the lack of “disease” status for aging.
A significant portion of the discourse addresses the NAD+ translational gap. While NAD+ precursors (NR and NMN) showed profound results in murine models, human clinical trials have largely failed to demonstrate equivalent efficacy. Verden posits that the primary driver of age-related NAD+ decline is not a lack of production but an increase in consumption via CD38, an ecto-enzyme characterized as a “leaky plug.” Current biotech efforts, including Napa Therapeutics, are pivoting toward CD38 inhibitors, moving into Phase I trials to address this metabolic leak directly.
The nutritional framework presented adopts a pragmatic, risk-stratified approach to supplementation. It prioritizes the correction of common deficiencies (Vitamin D3, B12, Omega-3) and the maintenance of the “metabolic army” (skeletal muscle) through increased protein intake (1.2–1.6g/kg) and creatine monohydrate. Conversely, the analysis aggressively deconstructs “Instagram medicine,” specifically targeting IV NAD+ and “detox” protocols as biologically implausible or clinically unproven. The conclusion emphasizes that while molecular interventions are accelerating, the current high-confidence protocols remain grounded in movement—specifically “exercise snacks” to combat the metabolic hazards of sedentary behavior—and rigorous tracking of personal biomarkers to move from “normal” to “optimal” ranges.
Insight Bullets
- Functional Priority: The geroscience field is shifting focus from “biological age” (blood-based) to “Intrinsic Capacity” (functional ability like gait, balance, and memory).
- Regulatory Bottleneck: Aging is not yet recognized as a disease by the FDA, which stifles Big Pharma investment; Intrinsic Capacity markers are being developed to provide the necessary validated endpoints.
- The CD38 Mechanism: CD38 is an enzyme that degrades NAD+; targeting this “leaky plug” is seen as a superior strategy to simply loading precursors like NR or NMN.
- Precursor Failure: Most human RCTs for NR and NMN have failed to replicate the dramatic longevity/health span effects seen in mice.
- Optimal vs. Normal: Standard clinical “normal” ranges (e.g., blood glucose) often ignore aging trajectories; longevity medicine targets the lower end of “normal” (e.g., 85 mg/dL vs. 99 mg/dL).
- Protein Requirements: For individuals over 70, protein intake should increase to 1.2–1.6g/kg/day to combat sarcopenia and maintain the “metabolic army.”
- Creatine’s Dual Role: Beyond muscle mass, creatine is emerging as a potential neuroprotective agent and mitochondrial health support in aging.
- Creatinine Misinterpretation: Supplementing with creatine can artificially elevate blood creatinine, leading to false diagnoses of kidney failure; Cystatin C is the required alternative marker.
- Vitamin Deficiencies: Aging reduces B12 absorption due to declining stomach factors; Vitamin D deficiency is nearly universal due to lifestyle/sunscreen use.
- Cocoa Flavanols: Specific extracts (not standard chocolate) have demonstrated cognitive maintenance in 2-3 year human clinical trials.
- Low-Dose Lithium: Epidemiological data suggests 5–10mg of lithium (levels found in some drinking water) correlates with increased life expectancy and mood stability.
- IV NAD+ Skepticism: Intravenous NAD+ is likely broken down by the liver before reaching target tissues and carries significant safety/quality control risks.
- Exercise Snacks: 2-minute bouts of movement every hour may be more metabolically significant than a single isolated gym session.
- Sedentary Risk: 8 hours of continuous sitting is posited as metabolically equivalent to the cardiovascular risk of smoking.
- Coffee Correlation: Consistent intake of 2–5 cups of caffeinated coffee is strongly correlated with reduced all-cause mortality across multiple cohorts.
Adversarial Claims & Evidence Table
| Claim from Video | Speaker’s Evidence | Scientific Reality (Current Data 2022-2026) | Evidence Grade | Verdict |
|---|---|---|---|---|
| NR/NMN failed in humans | Clinical observation | Zhang et al. (2023): Meta-analysis shows NMN increases blood NAD+ but shows inconsistent clinical outcomes for muscle/metabolism. | B | Plausible (Limited Efficacy) |
| CD38 inhibition increases lifespan | Napa Tx / Mouse data | Hsu et al. (2024): Pre-clinical models show CD38 inhibition restores NAD+; human Phase I data is still pending. | D | Translational Gap |
| Creatine benefits brain health | “New evidence” | Prokopidis et al. (2023): Meta-analysis confirms creatine improves memory performance in aging adults. | A | Strong Support |
| Cocoa Flavanols improve cognition | COSMOS trial | Sesso et al. (2022): Large RCT (COSMOS) showed no reduction in total CV events but improved cognitive scores in some sub-groups. | B | Plausible |
| Coffee reduces mortality | Epidemiological studies | Kim et al. (2023): Large-scale cohort analysis confirms 2-3 cups/day linked to lower all-cause and CV mortality. | C | Strong Support (Correlation) |
| IV NAD+ is ineffective | Bioavailability theory | [Source unverified in live search]: No Level A/B human trials support IV NAD+ for longevity; pharmacokinetic data suggests rapid degradation. | E | Unsupported / Safety Warning |
| Low-dose Lithium (5-10mg) | Gordon Lithkar/Buck studies | Kessing et al. (2023): Ongoing debate; some cohort data supports neuroprotection, but large-scale RCTs for longevity are absent. | C | Speculative |
Actionable Protocol (Prioritized)
High Confidence Tier (Level A/B Evidence)
-
Correct Deficiencies: Measure Vitamin D3 (Target >40 ng/mL) and B12 (use methylcobalamin).
-
Omega-3 Optimization: Target a high Omega-3 Index via diet (sardines/anchovies) or high-quality fish oil to support CV and brain health.
-
Resistance & Muscle Support:
-
Protein: 1.2g/kg (minimum) to 1.6g/kg (active) of daily protein.
-
Creatine: 3–5g daily monohydrate for muscle mass and cognitive support.
-
Glucose Monitoring: Track fasting glucose trajectories; aim for the lower quadrant of the normal range (80–85 mg/dL).
Experimental Tier (Level C/D Evidence)
- Cocoa Flavanols: 500mg daily of high-flavanol extract for potential cognitive maintenance.
- Micro-movement: Implement “exercise snacks”—2 minutes of stairs or squats every hour of sedentary work.
- Low-Dose Lithium: 1–5mg/day (Lithium Orotate) for mood and potential neuroprotection (high safety margin at this dose).
Red Flag Zone (Safety Data Absent / Debunked)
- IV NAD+ Infusions: Avoid due to lack of pharmacokinetic evidence and high risk of unregulated clinic compounding.
- Detox Diets/Teas: Disregard; these lack physiological basis as the liver/kidneys perform continuous detoxification.
- High-Dose Antioxidants: Avoid excessive Vitamin E/Beta-carotene supplementation, which has been linked to increased mortality in smokers and inhibition of “good” oxidative signaling.
Technical Mechanism Breakdown
- CD38 (Cyclic ADP-ribose hydrolase): An ecto-enzyme that serves as the primary consumer of NAD+ in aging tissues. Its upregulation is driven by chronic low-grade inflammation (“inflammaging”). Inhibiting CD38 preserves the intracellular NAD+ pool more effectively than precursor supplementation.
- Intrinsic Capacity: A composite score of Locomotion (balance/speed), Sensory (vision/hearing), Cognition (memory/orientation), and Psychological (mood/vitality) used to quantify functional biological age.
- Cystatin C: A protein produced by nucleated cells that provides a more accurate estimate of Glomerular Filtration Rate (GFR) than creatinine, especially in individuals with high muscle mass or those taking creatine supplements.
- NAD+ (Nicotinamide Adenine Dinucleotide): A coenzyme central to energy metabolism (redox reactions) and a substrate for DNA repair enzymes (PARPs) and sirtuins. Its decline impairs mitochondrial function and cellular resilience.
- The Sarcopenia Pathway: Characterized by the loss of skeletal muscle mass and function. Driven by mTOR resistance in aging, requiring higher per-meal leucine/protein thresholds to trigger muscle protein synthesis (MPS).
Eric Verdin sits down with Dr. Cynthia Kenyon, a true pioneer in the field of geroscience and the Vice President of Aging Research at Calico. Dr. Kenyon recounts the revolutionary discovery that aging is not merely a process of “wearing out,” but is a genetically regulated biological program. In 1993, Cynthia’s pioneering discovery that a single-gene mutation could double the lifespan of C. elegans roundworms while preserving function sparked an intensive study of the molecular biology of aging. The conversation explores how these findings translate from worms to mammals, the potential of drugs like Ozempic and Acarbose to extend human healthspan, and Dr. Kenyon’s proposal for a “World Healthspan Organization” to fund large-scale clinical trials for off-patent, low-cost compounds that currently lack traditional industry incentives.
Cynthia Kenyon graduated valedictorian in chemistry and biochemistry from the University of Georgia in 1976 and received her PhD from MIT in 1981. She then did postdoctoral studies with Nobel laureate Sydney Brenner at the MRC Laboratory of Molecular Biology in Cambridge, UK. In 1986, she joined the University of California, San Francisco as a Professor of Biochemistry and Biophysics. Dr. Kenyon is a member of the US National Academy of Sciences, the American Academy of Arts and Sciences, and the Institute of Medicine and she is a past president of the Genetics Society of America. She is now the Vice President of Aging Research at Calico.
Cynthia Kenyon: Switching on Resilience

Evaluation of Conserved Longevity Pathways and Translational Candidates
I. Executive Summary
The core thesis of this dialogue, led by Dr. Cynthia Kenyon (Calico) and Dr. Eric Verdin (Buck Institute), is a paradigm shift from the “stochastic wear-and-tear” model of senescence to a genetically regulated program governed by evolutionarily conserved signaling hubs. Central to this is the Insulin/IGF-1 Signaling (IIS) pathway, which was first identified in C. elegans as a “thermostat” for aging. Mutations in single genes, such as daf-2, demonstrated a 100% extension of lifespan in nematode models, maintaining physiological youthfulness into chronological old age.
The speakers argue that this pathway is not merely a metabolic regulator but a master switch for a systemic resiliency response. When IIS is moderately inhibited, the organism enters a “danger mode,” upregulating proteostasis (protein folding), antioxidant defenses, and DNA repair mechanisms. Crucially, this mechanism is highly conserved across species, from yeast and flies to mice and, potentially, humans.
Translational efforts are currently focused on pharmacological mimics of this state. SGLT2 inhibitors and GLP-1 agonists, originally developed for Type 2 Diabetes (T2DM), are highlighted as primary candidates for human longevity due to their ability to lower systemic glucose and insulin levels, thereby mimicking the “low-signal” state associated with extended lifespan in animal models. The discussion also touches on senolytics—the targeted clearance of inflammatory senescent cells—as a complementary strategy to extend healthspan.
The analysts identify a significant economic and regulatory gap: while off-patent compounds like acarbose, metformin, and aspirin show promise in animal Interventions Testing Programs (ITP), the lack of financial incentive prevents large-scale (Phase III) human longevity trials. The proposed solution is a global, non-profit “World Health Organization for Healthspan” to fund rigorous, placebo-controlled trials for low-cost longevity interventions.
II. Insight Bullets
- Aging Plasticity: Aging is a regulated biological process that can be altered even in late adulthood, as evidenced by C. elegans experiments.
- IIS Conservation: The IIS pathway is an “ancient” mechanism present in a common ancestor of worms and humans, suggesting high translational probability.
- The “Danger Signal” Paradox: Lifespan extension occurs not by removing “aging genes” but by triggering a survival response to a perceived (non-existent) threat.
- Proteostasis Enhancement: Inhibiting IIS improves protein folding, reducing the accumulation of toxic aggregates associated with neurodegeneration.
- SGLT2i Mechanism: These drugs induce “glucose dumping” via the kidneys, effectively lowering the systemic insulin “thermostat.”
- GLP-1 Pleiotropy: Beyond weight loss, GLP-1 agonists show emerging evidence in reducing neuroinflammation and treating addiction.
- Senolytic Synergy: Clearing senescent cells (SASP producers) complements metabolic interventions by reducing systemic “inflammaging.”
- Economic Barrier: The $500M–$1B cost of Phase III trials prevents the testing of off-patent longevity drugs like aspirin or acarbose.
- Demographic Inversion: Improving healthspan is an economic necessity due to the rising ratio of elderly to young populations.
- Kenyon’s Protocol: A rigorous low-glycemic index diet (no “white foods”) to minimize insulin spikes.
- Canine Longevity (Loyal): Large dogs age faster due to 28x higher IGF-1 levels than small dogs; LOY-002 aims to inhibit this overexpression.
- Epigenetic Stabilization: GLP-1 agonists have shown the ability to stabilize epigenetic age markers in recent 2025 clinical data.
- Dose-Response Criticality: Complete inhibition of insulin/IGF-1 is lethal; therapeutic benefit lies in moderate, specific attenuation.
- Collaborative Truth: The field requires a transition from individual supplement use to institutionalized, data-driven longevity consortiums.
III. Adversarial Claims & Evidence Table
| Claim from Video | Speaker’s Evidence | Scientific Reality (Current Data 2022-2026) | Evidence Grade | Verdict |
|---|---|---|---|---|
| IIS inhibition doubles human lifespan. | C. elegans mutation data. | Human centenarian studies show enriched IIS variants (e.g., FOXO3A), but no evidence for 2x lifespan extension exists in humans. Nidadavolu et al., 2024 | C | Speculative (for 2x effect) |
| SGLT2 inhibitors reduce all-cause mortality. | Pleiotropic metabolic benefits. | 2024/2025 Meta-analyses of 28 RCTs confirm ~28% reduction in all-cause mortality across diabetic/non-diabetic HF populations. Zheng et al., 2025 | A | Strong Support |
| GLP-1 agonists stabilize epigenetic aging. | Emerging evidence (referenced in 2025). | CROI 2025 data shows Semaglutide slowed biological aging by 9% over 32 weeks in HIV-associated lipohypertrophy. Corley et al., 2025 | B | Plausible |
| Acarbose extends human healthspan. | Mouse ITP data (22% increase). | Ongoing SAIL trial (NCT02953093) studying gene expression in older adults; results pending but safe. NCT02953093, 2025 | C | Plausible |
| Senolytic (D+Q) clearance improves function. | Unity/Buck Institute mouse data. | Phase 2 trials for SPMS and skeletal health show potential, but lack definitive Level A clinical mortality data. NCT07270120, 2026 | B/C | Experimental |
| Low Glycemic Diet reduces total mortality. | Kenyon’s personal protocol/Worm sugar data. | Lancet 2024 meta-analysis confirms low GI/GL diets correlate with reduced cardiovascular and all-cause mortality. Jenkins et al., 2024 | A | Strong Support |
IV. Actionable Protocol (Prioritized)
High Confidence Tier (Level A/B Evidence)
- Low Glycemic Load: Transition to a diet rich in high-fiber, non-starchy vegetables and lean proteins to maintain insulin sensitivity. Avoid refined “white” carbohydrates (rice, potatoes, bread).
- SGLT2 Inhibitors: For patients with metabolic dysfunction or heart failure (HFrEF/HFpEF), SGLT2i (e.g., Empagliflozin) provides robust mortality protection.
- GLP-1 Agonists: For obesity-driven accelerated aging, Semaglutide/Tirzepatide provide significant metabolic and potentially epigenetic stabilization.
- Resistance Training: Essential for maintaining muscle mass (counteracting sarcopenia) and insulin sensitivity.
Experimental Tier (Level C/D Evidence)
- Acarbose: Potential use in non-diabetics to blunt post-prandial glucose spikes, though gastrointestinal side effects are a limiting factor.
- Senolytics (Dasatinib + Quercetin): Currently in clinical trials for specific fibrotic and neurodegenerative indications; not recommended for general use until phase 3 completion.
- Metformin: Despite the TAME trial delays, epidemiological data supports metabolic benefits, but the effect on healthy, non-diabetic lifespans remains unproven.
Red Flag Zone (Safety Data Absent/Unsupported)
- High-Dose IGF-1 Suppression: Risk of immune dysfunction, muscle wasting, and cognitive decline in humans.
- Unregulated Supplement Cocktails: Mixing multiple “longevity” compounds (e.g., NMN, Resveratrol, Spermidine) without long-term safety monitoring for drug-drug interactions.
V. Technical Mechanism Breakdown
The primary biological axis discussed involves the Insulin/IGF-1 Signaling (IIS) pathway. The mechanism of action for lifespan extension is as follows:
- Receptor Attenuation: Reduction in DAF-2 (worm) or IGF-1R (human) activity decreases the phosphorylation of AKT/PKB.
- Transcription Factor Translocation: Reduced AKT activity allows the FOXO/DAF-16 transcription factor to move into the nucleus.
- Target Gene Activation: FOXO/DAF-16 upregulates a suite of genes involved in:
- Proteostasis: Molecular chaperones (HSPs) that ensure correct protein folding.
- Antioxidant Defense: Superoxide dismutase (SOD) and catalase.
- Metabolic Shift: Enhanced fatty acid oxidation and improved mitochondrial efficiency.
- Hormetic Response: This moderate inhibition acts as a xenohormetic signal, shifting the cell from a “growth and reproduction” state to a “somatic maintenance and repair” state.
1 Like
Brad Younggren: Filtering Out Aging

Therapeutic Plasma Exchange and Geroscience Translation
I. Executive Summary
The core thesis of the video features Dr. Brad Younggren, CEO of Circulate Health, outlining the translation of therapeutic plasma exchange (TPE) from hospital-based critical care into an outpatient intervention targeting age-related multi-systemic decline. The underlying geroscience framework shifts away from the traditional model of introducing youthful systemic factors, focusing instead on old plasma dilution. This paradigm, validated by the Conboy Lab, posits that biological aging is primarily driven by an accumulation of inhibitory, pro-inflammatory factors within the circulating exposome and proteome rather than a deficit of youth-promoting molecules. Mechanistically, TPE utilizes an extracorporeal centrifugal system to isolate whole blood, discard a weight-calculated volume of the patient’s plasma fraction, and replace it with therapeutic human-derived albumin and saline before reinfusing the intact cellular components.
The premier clinical data supporting this intervention stems from the single-blinded, randomized, sham-controlled “Circulate Trial” published by Fuentealba et al., 2025. Multi-omics profiling across 35 to 36 validated commercial epigenetic clocks demonstrated that an intensive regimen of six treatments over three months—structured as paired biweekly sessions followed by a multi-week rest—yielded an average biological age reduction of 2.61 years when paired with a low, protective dose of 2 grams of intravenous immunoglobulin (IVIG). Conversely, the sham-control arm exhibited a distinct acceleration in biological aging. TPE operates as a broad-spectrum “blood instrument” that clears the senescent secretome, downregulating circulating senescence-associated secretory phenotype (SASP) proteins, pro-inflammatory cytokines (such as IL-6 and TNF-alpha), and pathogenic lipoproteins.
Additionally, data from the “Circulate Plastics Trial” establishes that TPE serves as an effective modality for extracting environmental xenobiotics, reducing the blood-borne microplastic burden by roughly 60% in highly exposed individuals. A transient uptick observed in low-exposure cohorts highlights a clear circuit contamination variable, where microplastics are shed from the disposable polymer tubing and fluid bags. Scalability is heavily throttled by an acute shortage of trained apheresis nurses—estimated at only 3,000 nationwide—restricting the intervention to specialized outpatient clinics or mobile units.
II. Insight Bullets
- Mechanical Distinctions from Dialysis: TPE functions through automated centrifugal separation to physically isolate and remove the total plasma fraction containing large molecular weight disease mediators, contrasting with dialysis which utilizes membrane-bound absorption columns to clear small-molecule metabolic waste.
- The Dilution Paradigm of Rejuvenation: The biological objective shifts away from delivering scarce, young blood factors toward diluting age-imposed systemic molecular excess, a mechanism that restored tissue-specific stem cell proliferation in rodent models [Kim et al., 2022].
- Concealed Sham-Control Implementation: To isolate true therapeutic efficacy from placebo effects, the Circulate human trial incorporated a strict single-blind design where the apheresis equipment was fully hidden behind an opaque drape and ran active or inactive cycles.
- Epigenetic Clock Reversal Metrics: Longitudinal multi-omics analysis following an intensive multi-cycle TPE protocol demonstrated a statistically significant average biological age reduction of 2.61 years across a panel of 15 to 36 validated DNA methylation algorithms [Fuentealba et al., 2025].
- The Adverse Sham Acceleration Phenotype: Control patients undergoing the sham procedure manifested increased biological ages over the six-month study period, highlighting a distinct baseline trajectory of chronological decay when left untreated.
- Immunological Shielding via Low-Dose IVIG: Co-administering a conservative 2-gram dose of intravenous immunoglobulin post-procedure mitigates the transient depletion of endogenous protective antibodies, producing superior multi-omics rejuvenation signatures compared to isolated TPE.
- Evacuation of the Senescent Secretome: TPE mechanically strips the circulation of the senescence-associated secretory phenotype (SASP), reducing the systemic burden of destructive pro-inflammatory cytokines like IL-6, TNF-alpha, and IL-1beta.
- Proteomic Profile Normalization: Extracorporeal plasma clearance induces a global reset of the human proteome, downregulating pathogenic lipoproteins while youthfully restoring pro-regenerative, apoptotic, and anti-cancer signaling regulators [Kim et al., 2022].
- Microplastic Blood Burden Demolition: Clinical data from 114 subjects across 174 procedures confirmed that a single TPE session drops circulating microplastics and nanoplastics by approximately 60% in patients with high baseline accumulation.
- The Circuit Polymeric Contamination Variable: In patients presenting with low initial microplastic levels, post-procedure testing revealed minor, transient upticks caused by microscopic polymer shedding from the disposable PVC tubing and plastic fluid bags within the apheresis circuit.
- Geographic Variations in Environmental Toxins: Baseline toxicant profiling identified significant regional differences in microplastic accumulation; individuals in the Pacific Northwest consuming glacier-fed groundwater displayed exceptionally low baseline plastic burdens.
- Vascular Access and Flow Dynamics: Standard outpatient delivery dictates dual venous access lines (one draw arm, one return arm) to complete the weight-calculated plasma exchange volume safely within a two-to-three-hour operational window.
- Transition to Biomarker-Driven Scheduling: Clinical management is evolving past rigid calendars to an adaptive maintenance model, re-administering TPE only when standard healthspan markers (hs-CRP, LDL, homocysteine) drift back to the patient’s pathogenic baseline.
- Targeting Non-Aging Complex Pathologies: Beyond healthy longevity, outpatient apheresis networks are utilizing specific protocols to manage chronic post-infectious and autoimmune syndromes, including Long COVID and Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS).
- Transient Depletion of Endogenous Clotting Factors: Because TPE non-selectively discards host plasma, it temporarily reduces vital coagulation factors, necessitating strict pre-operative screening and pause protocols for patients on antiplatelet or anticoagulant regimens.
- Severe Human Resource Scalability Constraints: The clinical expansion of apheresis is throttled by a highly restricted labor supply, as only approximately 3,000 nurses in the United States possess the critical hospital-level training required to operate these systems safely.
- Prohibition of Home-Care Administration: Due to acute risks of rapid fluid shifts, electrolyte imbalances, and vascular access failure, TPE cannot transition to a self-administered home protocol and must remain restricted to specialized clinics or mobile medical units.
- The Peripheral Sink Effect in Neurodegeneration: Large-scale clinical evidence from the AMBAR trial demonstrates that replacing plasma albumin alters peripheral-central gradients, facilitating the clearance of amyloid-beta and p-tau out of the cerebrospinal fluid to slow Alzheimer’s disease progression [Boada et al., 2020].
- TPE as a Combination Geroprotective Platform: Long-term healthspan extension will require coupling TPE (“TPE + X”) with specific metabolic or small-molecule geroprotectors (e.g., rapamycin or GLP-1 receptor agonists) to exploit the immunomodulatory window opened by plasma clearance.
IV. Actionable Protocol (Prioritized)
High Confidence Tier (Level A/B Evidence)
- Neurodegenerative Decline Mitigation (Alzheimer’s Disease): Follow the structured AMBAR trial framework for mild-to-moderate Alzheimer’s disease to slow cognitive and functional decline. The protocol requires an intensive phase of six weekly sessions (exchanging 2 hours of weight-based volume with 5% therapeutic albumin), followed immediately by a maintenance phase of at least 10 monthly sessions [Boada et al., 2020].
- Standard Clinical Biomarker Tracking: Utilize standard, readily available laboratory assays (Quest/Labcorp) rather than expensive exploratory multi-omics. Prior to and 30 days post-intervention, measure high-sensitivity C-reactive protein (hs-CRP), low-density lipoprotein (LDL), and total homocysteine to objectively map systemic vascular and inflammatory improvements.
Experimental Tier (Level C/D Evidence with High Safety Margins)
- The Epigenetic Rejuvenation Regimen: To target systemic biological age reduction, implement the core Circulate trial protocol: three intensive cycles delivered over approximately three months. Each individual cycle consists of two TPE procedures administered within a single week (e.g., Tuesday and Thursday) utilizing human-derived albumin replacement, followed by a three-week therapeutic rest period [Fuentealba et al., 2025].
- Biomarker-Adjusted Maintenance Scheduling: For healthy longevity optimization, space maintenance sessions every 4 to 6 months. Transition the pacing to an adaptive model: re-administer a TPE cycle only when the patient’s hs-CRP or lipid markers return to their pre-treatment baseline.
- Circulating Xenobiotic and Microplastic Clearance: For individuals with verified high-exposure occupations or documented high baseline burdens of persistent organic pollutants (PFAS) and microplastics, utilize a single TPE session to achieve an immediate ~60% reduction in circulating toxicant concentration.
Red Flag Zone (Debunked or Safety Data Absent)
- Home Self-Administration: Do not attempt to modify or scale apheresis equipment for home or unmonitored use. The procedure introduces severe risks of acute hypovolemia, syncope, and electrolyte shifts that strictly require specialized hospital-trained apheresis nurses.
- Unreplaced Donorship/Generic Plasmapheresis: Avoid high-frequency plasmapheresis or blood donation protocols that fail to replace volume with premium human-derived albumin. Evidence indicates that unreplaced plasma removal fails to induce epigenetic rejuvenation and can paradoxically accelerate biological aging clocks (such as DNAmGrimAge).
- Active Anticoagulation Interventions: Never undergo venipuncture or extracorporeal circulation while maintaining full-dose systemic anticoagulation or antiplatelet therapy. Patients must clear medical screening and execute a temporary, physician-supervised cessation of blood thinners 48 to 72 hours prior to the procedure to prevent catastrophic hematomas and bleeding, as TPE naturally strips endogenous clotting factors.