It does not have that many references, but I thought people might like to see it.
https://twitter.com/healthspanmed/status/1713706369839456738
It does not have that many references, but I thought people might like to see it.
https://twitter.com/healthspanmed/status/1713706369839456738
Does anyone know why Mannick had a two week break between rapamycin use and the influenza vaccination? It might help answer the question why some people choose to cycle rapamycin and go on breaks every now and then.
It’s interesting that they note that only the 5 mg weekly dose and 0.5 mg daily dose met the primary endpoint, meaning a 1.2 fold increase (black line) for two influenza strains, and that 20 mg weekly did not do so. The 1.2 fold increase was chosen as a target since it was associated with a decrease in influenza illness.
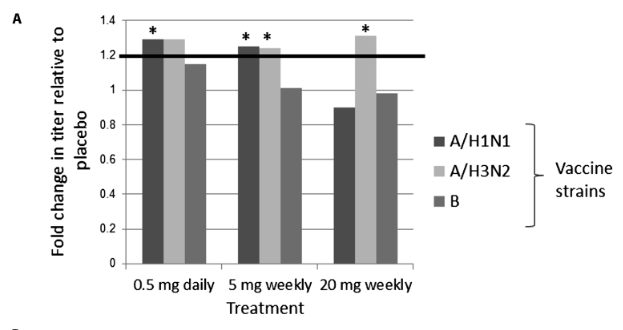
This suggest 20 mg weekly is not beneficial? @Olafurpall
Regardless, an improvement in age-related decline in immune function for those who aren’t aware suggest a preliminary age reversal in humans. At least for that.
I don’t remember the details of the Mannick study. I would guess the reason for the two week break is that they didn’t want the short term effects of rapamycin to influence the results but wanted to see the longer term effects of rapamycin. A two week break would be enough to get the rapamycin completely out of the system.
I wouldn’t say so. It probably means that 20 mg weekly is a high enough dose to start causing minor immunosuppressive effects in some subjects, but that doesn’t necessarily mean that dose isn’t beneficial overall still. The benefits of that dose could still very well outweight the negatives.
Good point, didn’t think of that.
The influenza vaccine was given two weeks after taking the 20 mg, in that case if it was beneficial for immunosenescence (and aging in general) the improvement would be larger after a longer break then after the higher dose? Unfortunate they didn’t have a longer break if so, so the immunosuppressive effects could be ruled out.
References would definitely help. Some statements need clarification. For example, #12 (The low-dose RAD001 groups (0.5 mg daily or 5 mg weekly) met the study’s primary endpoint) and #35 (When higher doses of rapamycin are used, or the drug is taken dailyits mTORC2 that ends up being inhibited).
#12 states that daily dose met primary endpoint, and #35 contradicts it.
What I do not understand here?