https://twitter.com/DrMorganLevine/status/1769027566164472000?t=xN-SJWsNWE8Zze_9hD9TQg&s=19
4 Likes
My experience of discussing the science with some experts is that their knowledge of the science tends to be quite narrow.
There will, however, always be an issue with the popularisation of subtle scientific questions being done with inaccuracies. Realistically there are issues to debate in what appears in some scientific papers. Hence things done perhaps to a greater extent for clickbait are always likely to be less accurate. After all some scientific papers are at least in part written for clickbait.
5 Likes
This was a very interesting step up from the Sinclair — Kaeberlein blow up last week. The biological age measurements are definitely a work in process.
Trying to use small changes in volatile, black box algorithm outputs to assess progress in anti-aging is foolish at this point. I remain a fan of the blood marker based calculators (Levine) plus using other markers as used by @ConquerAging.
In blood markers at least we have the benefit of many years of study. Perhaps an overall age result is a bad idea since it only takes one bad organ to get you, so an organ scorecard approach or similar is probably best. My biological age should be my highest aged organ.
I’m glad there is some pushback against the marketing hype machines out there. It helps me to remain intellectually honest with myself.
5 Likes
If you don’t want to make longevity influencers look like psuedoscience:
- Stop with the biological age clocks and that nonsense.
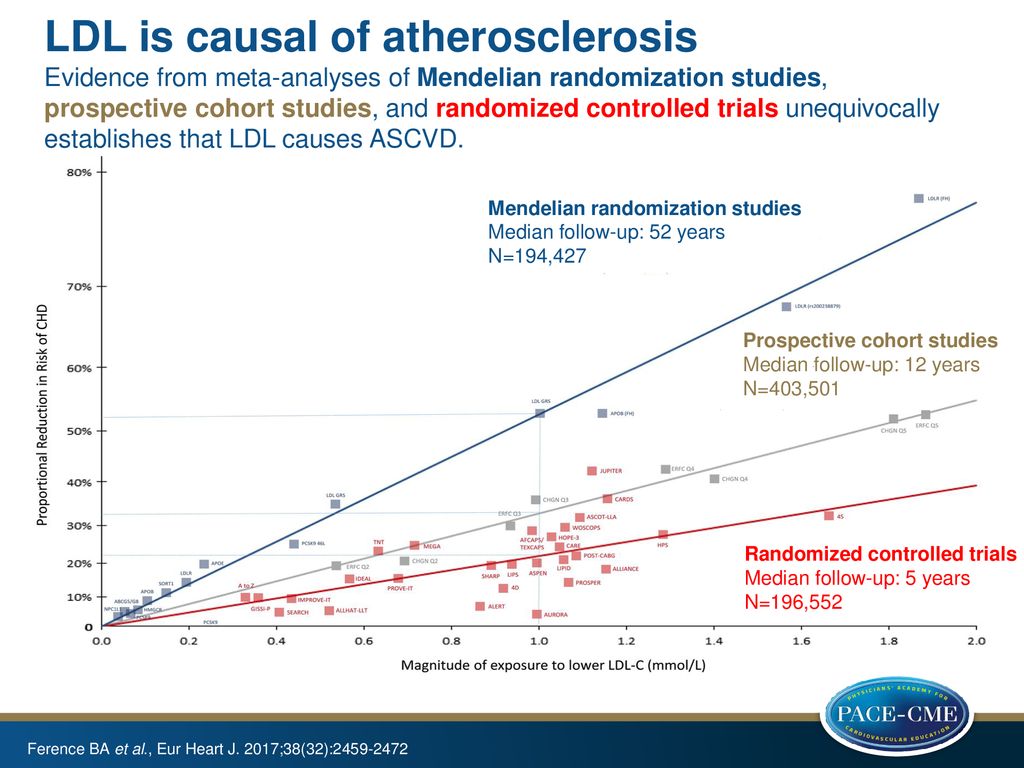
- Focus on drugs with proven beneficial outcomes in humans, based on clinical trials and mendelian randomization studies.
2.1 That means drugs like statins. If you don’t mention statins or other apoB lowering drugs ever you are probably a part of the problem.
2.2 Sun screen.
2.3 Possibly SGLT2i.
2.4. … - Recognize the difference of a TIME based and AGE based disease. If you cannot differentiate between those two, you are probably in psuedoscience territory. An example of this is believing heart disease is an AGE based disease, when TIME along with exposure to atherogenic particles is most likely playing the largest role based on mendelian randomization studies.
- Recognize the power of compounding effects of early treatment, outside of treatment duration in clinical trials, based on for example mendelian randomization studies.
- After talking about proven therapies and strategies a lot, then in passing you can mention that we don’t have clinical trials for drugs showing a lifespan increase in mice, but it is possible to sometimes take them safely and have a risk vs. reward calculation.
- Fund and talk about studies that will create clinical trials or mendelian randomization studies and drug repurposing studies based on the latter.
4 Likes
So we disagree about whether heart disease is at least in part an AGE based disease.
Looking at these I am not the only person who thinks there is an age related disease element to CVD. Describing that view as “pseudoscience” is basically wrong.
5 Likes
No we don’t, it is probably playing some role but it much more minor than those in/previously in psuedoscience territory have said. I have not seen you or anyone else explain how much of the difference in outcomes age plays vs. time and exposure to atherogenic particles. If you can’t quantify it or measure it…? Once exposure is very low outcomes go down drastically in genetic studies, so much for the age hypothesis of heart disease.
They made it sound like rejuvenating drugs will prevent heart disease despite the fact that the majority of young people have atherosclerotic plaque. It is dangerous because it makes people wait and be passive as well as being false.
3 Likes
I am not going to engage in a long discussion about the subtleties of this, but I believe on everything I have read that age has more effect. I think it is one of those things that happens as the genome stops fully functioning. Young people get scarring as well.
3 Likes
What people say is lowest in the evidence hiearchy: The Evidence Hierarchy - Evidence Based Medicine - Levy Library Guides at Icahn School of Medicine at Mount Sinai
All the studies on age and heart disease are confounded by time and exposure to atherogenic particles. Once exposure to atherogenic particles goes down, disease progression reverses and long-term outcomes are massively improved up to 80% reduction in heart disease and probably more, depending on time for the reduction.
If age played such an important role we wouldn’t see such a massive reduction in heart attacks. Occam’s razor.
3 Likes
Excellent post! I don’t agree with everything but it’s a clear presentation of your valuable point of view. I think the epigenetic clocks are making a lot of progress and will be quite valuable. Your focus on statins, in the big picture, is right. If everyone took statins that needed them and started earlier, it would dramatically change the landscape of heart disease.
What proportion of heart disease is TIME or AGE based is debatable but I think your point that the TIME factor is overlooked is correct. As also the importance of early treatment.
3 Likes
The following is a good explanation of what athrogenic particles are and their role:
Atherogenic particles are lipoprotein particles that play a crucial role in cardiovascular health. Here’s what you need to know:
-
Lipoprotein Particles:
- Cholesterol and triglycerides are fats that circulate in your blood. They can’t dissolve in blood directly, so they travel within lipoprotein particles.
- These particles act as containers, carrying cholesterol and triglycerides throughout your body.
- Notable lipoprotein particles include:
- Low-Density Lipoprotein (LDL): Often miscategorized as “bad” cholesterol, LDL particles carry mostly cholesterol. Over 90% of atherogenic particles are LDL particles.
- High-Density Lipoprotein (HDL): Often miscategorized as “good” cholesterol, HDL particles also carry cholesterol.
- Chylomicrons and Very-Low-Density Lipoprotein (VLDL): These particles primarily carry triglycerides.
-
Atherogenic Particles:
- Atherogenic particles are those that contribute to plaque formation in your arteries.
- They share a common characteristic: each has one apolipoprotein B (ApoB) molecule on its outer surface.
- Over 90% of these atherogenic particles are LDL particles.
- Whether small or large, all LDL particles are equally bad and capable of driving arterial plaque formation.
- As atherogenic particle levels increase, more particles deposit in artery walls, promoting plaque formation.
- The higher your atherogenic particle number, the greater your risk of cardiovascular events.
- LDL Particle Score (LDL-P) and ApoB Score directly quantify these potentially atherogenic particles.
Remember, it’s not just about “good” or “bad” cholesterol—understanding the particles carrying these lipids is key to assessing your cardiovascular health¹²³. ![]()
Source: Conversation with Bing, 3/18/2024
(1) What you Need to Know About your Atherogenic Particle Number (LDL-P or … What you Need to Know About your Atherogenic Particle Number (LDL-P or ApoB) — Precision Health Reports.
(2) Atherosclerosis Development and Progression: The Role of Atherogenic … Medicina | Free Full-Text | Atherosclerosis Development and Progression: The Role of Atherogenic Small, Dense LDL.
(3) Atherogenic Lipoprotein Particles in Atherosclerosis - AHA/ASA Journals. https://www.ahajournals.org/doi/pdf/10.1161/01.cir.0000131511.50734.44.
5 Likes
tbf, Mike Lustgarten is also kind of guilty of the same thing (though he’s not misleading, the Levine biological age isn’t exactly the best indicator of “age reversal” either)
Christin Gloriso posted on LinkedIn that her results on different aging clocks were all over the place. Same with Kaeberlein, same with Jason Mercurio. Divergences between clocks seems especially common in a lot of healthy older people…
3 Likes
He’s increasing his LDL because a dumb clock said it’s good. It’s madness to consider every blood biomarker the equal weight when some are seriously implicated in common disease and it is not fitted on an exponential curve and using evidence other than association studies. Some mathematician or engineer can make an actually good calculator based on causal risk factors / compounding risks / benefits (i.e apoB exposure over a lifetime, blood pressure, etc).
2 Likes
yeah, he goes over A LOT but I’m afraid he has the opportunity to be collecting really important data, but he’s going after the wrong markers (we WILL see better markers soon, eg Teal Omics]
also weighing them equally in terms of (+) good and (-) bad isn’t valid given that their weightings are heavily unequal
3 Likes
Someone just needs to start a website where they list all of the most important biomarkers, actually important biomarkers, references to studies, and then create a calculator based on those biomarkers for an overall score. They should be categorized for every common disease, like cardiovascular disease then cancer. ApoB is going to be weighted heavily. Hence why if only one marker should be tested it is that.
The website must have a good user interface and modern design too.
1 Like
Just saw the thread on Teal. Any idea when they will start offering a test? @Neo mentioned " Enroll Now to Request a Spot in our 2024 Launch", any info on that?
1 Like