Both individuals taking rapamycin, an anti-aging drug, and those not taking it will ultimately succumb to age-related diseases. However, the former, if administered disease-oriented dosages for a long time, may experience a delayed onset of such diseases and live longer. The goal is to delay a particular disease that is expected to be life-limiting in a particular person. Age-related diseases, quasi-programmed during development, progress at varying rates in different individuals. Rapamycin is a prophylactic anti-aging drug that decelerates early development of age-related diseases. I further discuss hyperfunction theory of quasi-programmed diseases, which challenges the need for the traditional concept of aging itself.
Currently, doses and schedules of rapamycin for longevity are based on the wrong objective: to avoid side effects. Nothing else. The doses of all other drugs are chosen to achieve therapeutic goals. For aspirin’s example, rheumatoid arthritis patients received high-dose aspirin (3600 mg/day) daily [31], while for prevention of cardiovascular diseases we use low-dose aspirin (81 mg). Depending on the pathology, aspirin usage can be intermittent or continuous [32, 33]. Side effects avoidance is a secondary goal, even though side effects may be deadly.
Side effects of rapamycin are not remarkable at all. They even less dangerous than the side effects of most other drugs [34, 35]. Since 1999, millions of patients with serious illnesses tolerated rapamycin well. Continuous (everyday) even high doses were studied successfully in patients [36]. A failed suicide attempt (103 tablets or 103 mg) caused no effects except elevated blood lipids [37]. In some studies, side effects were higher in the placebo group than in the rapamycin-treated group [38].
I really like reading Blagoskonny and his way of thinking is really remarkable not only in scientific but in philosophical way as well. He is really playful and creative with ideas. It is curious and so simple idea that the same “power” that makes us grow from a single cell to an adult human makes us later in life age and die. Just fascinating thought.
Yes, this is a really interesting paper! I had though the interview with him yesterday so not possible to suggest more questions In that interview he mentioned this paper and I really like the part that the aging is replaced with the term age-related diseases. It makes the theory more elegant in a way and easier to take in
**
However, (rapamycin), if administered disease-oriented dosages for a long time, may experience a delayed onset of such diseases and live longer.
**
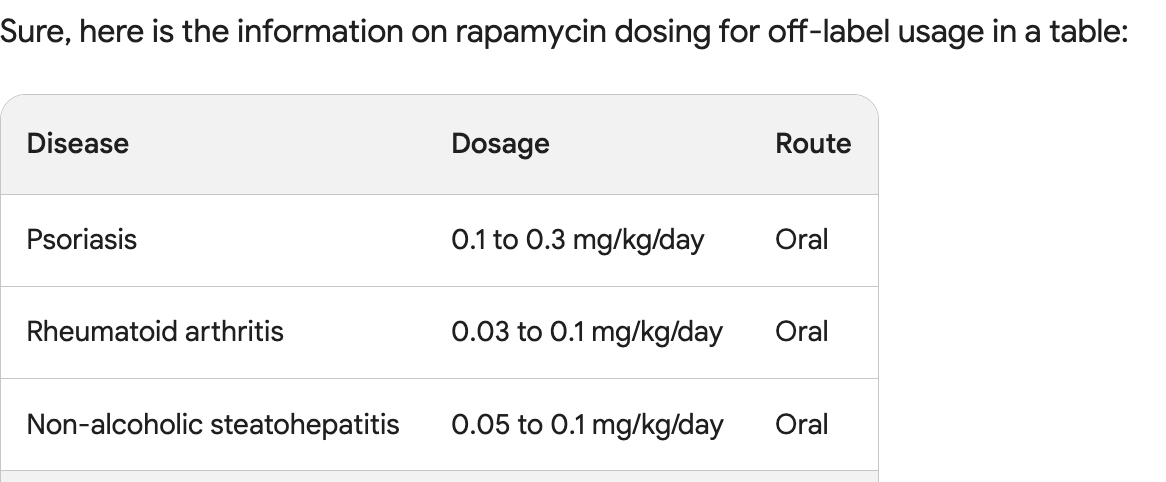
Can someone point me to a list of disease-oriented rapamycin dosages?
Rapamycin is basically anti-inflammatory so whatever the anti-inflammatory medications you are on, for instance prednisone or biologics, one can use low dose Rapa in combination with reduced dosage of the other. In psoriasis, the study used low dosage of rapa combined with reduced Cyclosporin (a very toxic medication).
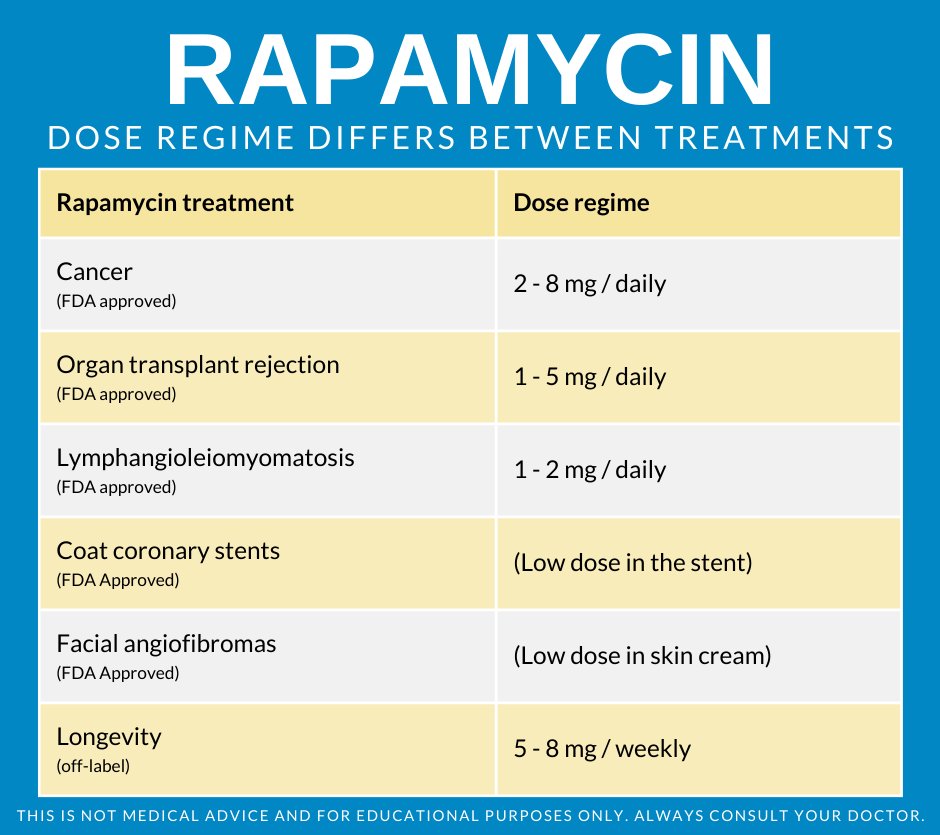
@Krister_Kauppi had a summary table graphic he did (I seem to remember) of all the different dosing levels used in different disease applications. Perhaps he can post it again.
Is that table based on data from chatgpt because as we seen before the data and sources it delivers are many time fake. Can you provide the sources to those dose regimes?