Rifampicin is the most powerful known inducer of the hepaticcytochrome P450 enzyme system, including isoenzymes CYP2B6, CYP2C8, CYP2C9, CYP2C19, CYP3A4, CYP3A5, and CYP3A7.[41] It increases metabolism of many drugs[42] and as a consequence, can make them less effective, or even ineffective, by decreasing their levels.[43] For instance, patients undergoing long-term anticoagulation therapy with warfarin have to increase their dosage of warfarin and have their clotting time checked frequently because failure to do so could lead to inadequate anticoagulation, resulting in serious consequences of thromboembolism.
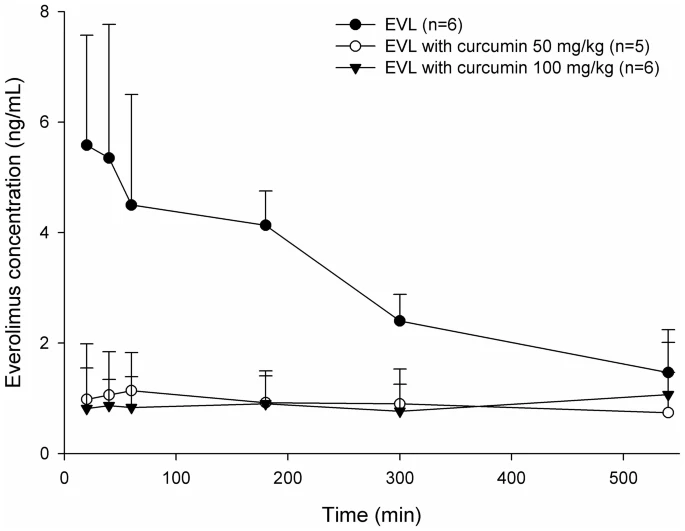
That’s great that it directly tests coadministration of Rapamycin(Everolimus) and Curcumin, and it decreased AUC by 70.6%, it seems that Curcumin significantly decreased the absorption of Everolimus.
Can we infer that “sequential” administration of Rapamycin then Curcumin also has the similar effect of "coadministration " of Rapamycin and Curcumin?
I.e. coadminstration of Curcumin decreased AUC of Everolimus mainly by decreasing bioavailability of Everolimus, but if there already existed high Everolimus blood concentration, then does sequential administration of Curcumin also increase the clearance of Everolimus?
One would assume that yes it still would speed the clearance of any CYP3A4 substrates which exist in the bloodstream. I think you want to make sure that the curcumin doesn’t have added piperine.
Curcumin bioavailability is very low so most formulations have a way to either deliver more (like Meriva) or slow the metabolism (with piperine for it’s CYP3A4 inhibition).
Our results have suggested that
rifampin enhanced the metabolism of risperidone
during both presystemic and elimination phases
CONCLUSION
This study shows that 5-day pretreatment with
600 mg of oral rifampin causes a significant
reduction in plasma concentration of risperidone
by enhancing its metabolism in the liver rather than
the small intestine.
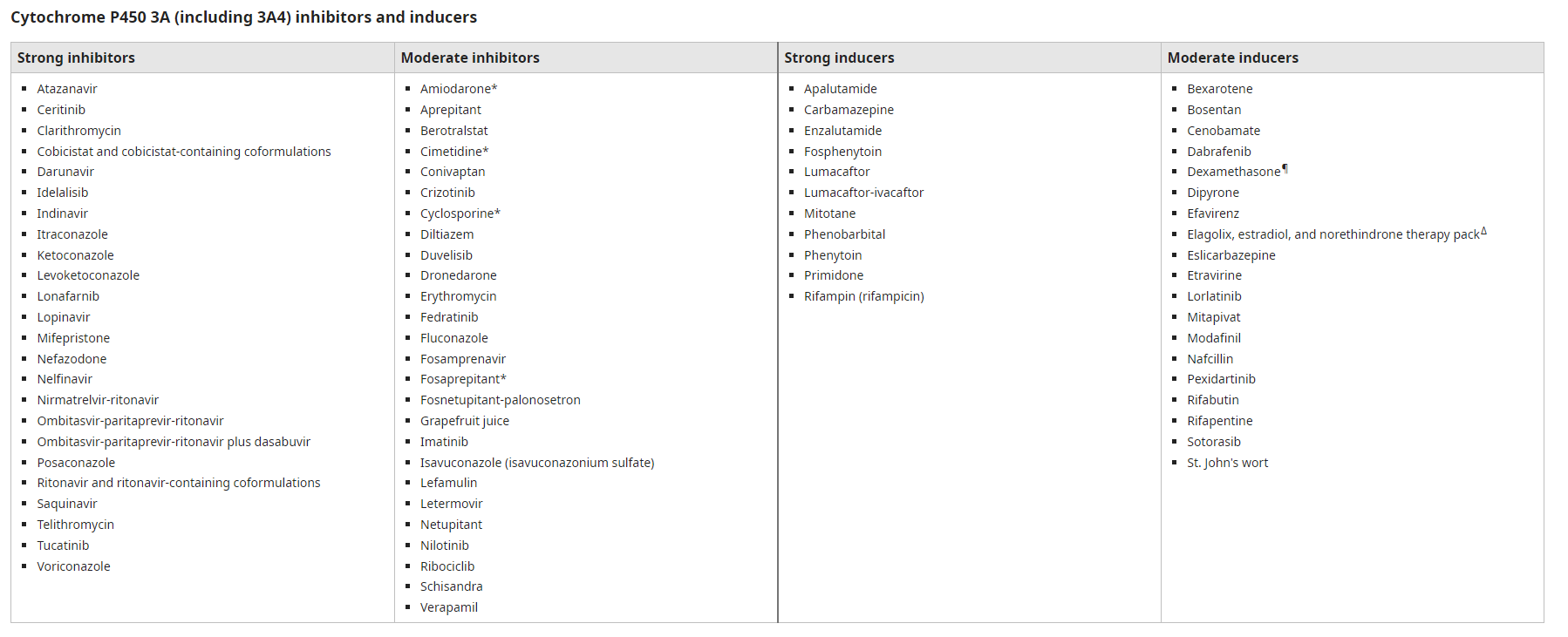
I found there are also some moderate/strong Cytochrome P450 3A inducers, but I am not very familiar with these drugs, anyone has any opinions on them?
Considering the safety and there was a trial of Curcumin with rapamycin (everolimus), I would like to try Curcumin next time, but any opinions of other inducers are also welcomed.
On the issue of mTOR inhibition - I had read the same paper you’ve read, but Dudley Lamming, who I think is a much better and more experienced person when it comes to mTOR and rapamycin studies says no, that is not true. They see less mTOR2 inhibition with Everolimus.
I recommend you watch this video, at least the mTOR 2 inhibition sections (some of the questions / comments by the transhumanist participants in the video seem like a waste of time).
A good presentation covering rapamycin and rapalogs by two experts in the field; Dudley Lamming and Adam Konopka. Covers rapamycin, as well as rapamycin/metformin simultaneous use, everolimus and mTOR2 inhibition, immtor, etc.
I have finished the presentation, very informing, Dudley Lamming clearly explained mTorc1 and mTorc2, and mentioned that Everolimus disrupts less glucose homeostasis than sirolimus.
RapAdmin, do you know any expert or MD in the field has changed sirolimus to everolimus?
some side effects are correlated with peak levels (diarrhea, GI issues, etc.) but the bigger side effect issues (immune suppression) are correlated with chronic (daily) and ongoing rapamycin use and trough levels (the higher the trough levels, the greater the immune suppression)
I have no idea. We need to read up, its not exactly obvious:
The effect of rifampin on the pharmacokinetics of sirolimus in healthy volunteers
Sirolimus, metabolized primarily by intestinal and hepatic CYP3A4, is a substrate for P-glycoprotein. CYP3A4 inducers would be expected to decrease sirolimus exposure. This open-label, nonrandomized study investigated effects of CYP3A4 induction, by rifampin, on sirolimus pharmacokinetics. Healthy volunteers received sirolimus 20 mg on day 1. After washout period, multiple 600-mg rifampin doses were administered daily for 14 days. On day 9, one 20-mg sirolimus dose was administered after an overnight fast (≥10 hours). Whole blood samples for sirolimus collected for 144 hours after each dose were analyzed by liquid chromatography/tandem mass spectrometry. Pharmacokinetic parameters, assessed using noncompartmental methods, were compared using analysis of variance. Geometric mean ratios of Cmax and AUCinf were 29% (90% CI: 26, 32%) and 18% (90% CI: 16, 21%), respectively, with rifampin co-administration versus sirolimus alone. Corresponding decreases in Cmax and AUC were 71% and 82%, respectively, which would likely cause trough concentrations to fall below the recommended therapeutic range. Mean CL/F increased approximately fivefold with rifampin versus sirolimus alone. Co-administering sirolimus and potent CYP3A inducers is not recommended. If co-administration is necessary, dose adjustment and concentration monitoring should be conducted.
Effect of rifampicin to inhibit rapamycin-induced autophagy via the suppression of protein phosphatase 2A activity
Here, we demonstrate that the rapamycin-induced autophagy is dependent on protein phosphatase (PP) 2A activity and rifampicin inhibits the activity of PP2A by reducing expressions of PP2A subunits A and C. In addition, rifampicin slightly, but significantly, inhibited the rapamycin-induced dephosphorylation of p70 ribosomal protein S6 kinase (p70S6K) at Thr421/Ser424, which are regulated dually by both rapamycin and PP2A, but not at the rapamycin dephosphorylation site located at Thr389. These results show that rifampicin inhibits rapamycin-induced autophagy, at least in part, via the suppression of PP2A activity.
I would just note that this hypothesis seems to be wrong given my conversation with Adam Salmon a while back. At least he believes that the longevity effects of rapamycin are likely the AUC, not the peak (CMax) levels of rapamycin.
Currently, I think many scientists (Dudley Lamming, etc.) think its the trough levels of rapamycin are the most important factor in side effects. The higher the trough level, the greater the side effects (due to mTORC2 inhibition) is the hypothesis.