I’m continuing my deep dives into the genetic pathways to get actionable insights as the previous ones have been incredible precise and useful. This time I’m looking at the thymus and Immunosenescence related genetic pathways.
Here is the general description of the pathways and their variants. I will put the finding about my own genome below it as an example of what useful and actionable insights you can get.
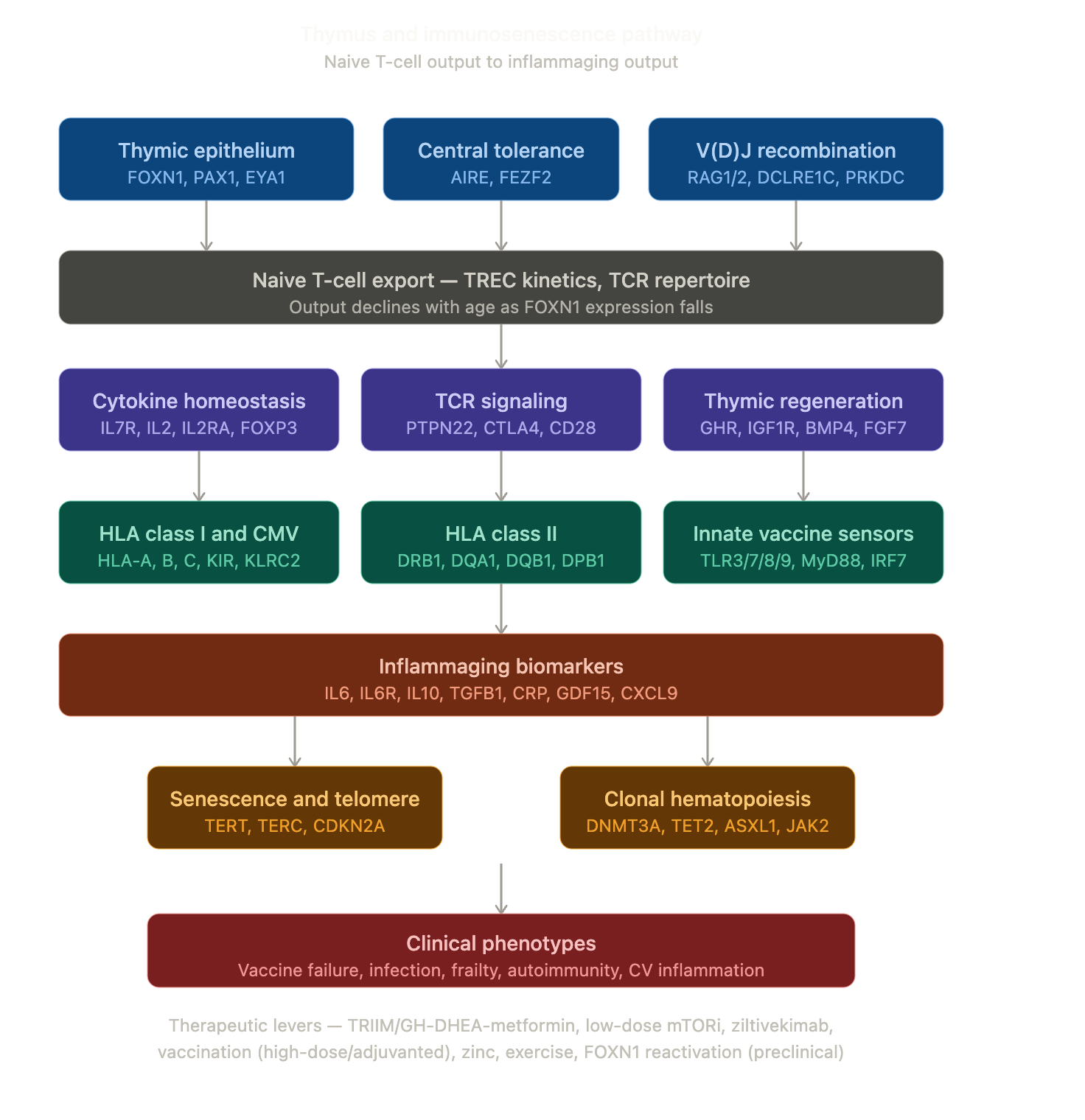
Thymus_Immunosenescence_Genetic_Pathway_Reference.pdf (605.7 KB)
The pdf report above is valid for everybody but here is the summary of the findings I get when I apply it to my own genome as an example.
Thymus & Immunosenescence — One-Page Summary Card
Personalized analysis · Generated 8 May 2026 · 60× WGS · GRCh38 · 67/67 SNPs resolved (24 non-REF + 43 REF/REF)
TOP 10 ACTIONABLE FINDINGS
| # | Finding | Direction | Action |
|---|---|---|---|
| 1 | PTPN22 R620W: G/G (homozygous wild-type) |
|
NO copy of largest non-HLA autoimmune-priming allele. Substantially below-average autoimmune-disease genetic risk. Reassuring. |
| 2 | IL6 −174: G/G + IL6R D358A: A/A |
|
Homozygous high-IL-6 producer + non-protective IL-6R. Quarterly hsCRP. Watch ZEUS trial 2026-2027 for ziltivekimab. Do NOT add colchicine (CLEAR SYNERGY 2024 negative). |
| 3 | IL2RA compound homozygous risk haplotype (rs2104286 G/G + rs12722489 T/T) |
|
Reduced CD25/IL-2 signaling → modest Treg-functional reserve. Rapamycin (already in regimen) preferentially expands FOXP3+ Tregs and partially compensates. |
| 4 | FCGR2A H131R: G/G = R/R (homozygous lower IgG2 binding) |
|
Blunted opsonization of polysaccharide-encapsulated pathogens. Confirm PCV20 or PCV21, Shingrix 2-dose, high-dose flu (Fluzone HD or Fluad). |
| 5 | IL7R T244I: T/T (homozygous protective for MS, recessive OR 0.84) |
|
No action; reassuring for peripheral T-cell homeostasis. |
| 6 | TERT intron 2: A/A (homozygous shorter-LTL allele) |
|
Predicted shorter leukocyte telomere length. Consider one-time direct LTL measurement (flow-FISH). |
| 7 | 9p21 (CDKN2BAS1) heterozygous CAD risk (rs10757278 A/G + rs1333049 G/C) |
|
One copy of the major CAD-risk haplotype. Current Pitavastatin 4 mg + Repatha 140 mg q2wk + Ezetimibe + Aspirin regimen aligned and well-controlled. |
| 8 | TGFB1 L10P + −509: A/A + C/C (homozygous lower-TGF-β1 producer) |
|
Favorable for cardiac/renal aging trajectory. No action; supportive. |
| 9 | CMV IgG serology unknown |
|
Single most important variable for immunosenescence trajectory calibration. Get one-time CMV IgG. |
| 10 | Do NOT add low-dose colchicine for inflammaging-CV risk |
|
CLEAR SYNERGY (NEJM 2024, n=7062 post-MI, 3.5y follow-up) negative for primary endpoint despite confirmed CRP reduction — supersedes COLCOT 2019 and LoDoCo2 2020. |
CONVERGENCE PATTERNS (3)
- Inflammaging Bottleneck: IL6 G/G → IL6R A/A (no protective sIL6R sink) → IL10 het → TERT A/A (shorter LTL → more SASP) → 9p21 het CAD risk. Central biology-of-aging finding. Maps to ZEUS / ziltivekimab 2026-2027.
- Treg Homeostasis Compound Vulnerability: IL2RA rs2104286 G/G + rs12722489 T/T compound homozygous → reduced CD25/IL-2/STAT5 signal. Rapamycin compensates.
- Encapsulated-Pathogen Vulnerability: FCGR2A R/R lower IgG2 binding → confirm PCV20/PCV21 + Shingrix + high-dose flu.
CURRENT REGIMEN — KEY ALIGNMENTS
![]() Highly aligned: Rapamycin 12 mg q3wk · Tirzepatide 2.6 mg 2x/wk · Pitavastatin 4 mg + Repatha 140 mg q2wk + Ezetimibe + Aspirin · EPA/DHA combined ~2.6 g EPA + 0.8 g DHA daily · Empagliflozin 25 mg
Highly aligned: Rapamycin 12 mg q3wk · Tirzepatide 2.6 mg 2x/wk · Pitavastatin 4 mg + Repatha 140 mg q2wk + Ezetimibe + Aspirin · EPA/DHA combined ~2.6 g EPA + 0.8 g DHA daily · Empagliflozin 25 mg
![]() Aligned: Vitamin D3 5000 IU EOD · Olive Leaf Extract · Avmacol (sulforaphane) · Zinc 15 mg (Momentous Multi) · Telmisartan 80 mg · Tadalafil 10 mg · Doxycycline 20 mg BID · DHEA 25 mg EOD (TRIIM-aligned)
Aligned: Vitamin D3 5000 IU EOD · Olive Leaf Extract · Avmacol (sulforaphane) · Zinc 15 mg (Momentous Multi) · Telmisartan 80 mg · Tadalafil 10 mg · Doxycycline 20 mg BID · DHEA 25 mg EOD (TRIIM-aligned)
![]() Neutral: Other supplements (no contradictions)
Neutral: Other supplements (no contradictions)
TOP 5 PRIORITY INTERVENTIONS
- HIGH — Confirm vaccinations: RZV (Shingrix 2-dose), PCV20 or PCV21, annual high-dose/adjuvanted influenza, current COVID booster
- HIGH — One-time CMV IgG serology
- HIGH — Continue current regimen unchanged (already directly aligned with all major findings)
- MODERATE — Add to standard panel: quarterly hsCRP; one-time baseline IL-6, GDF15; once-only LTL (flow-FISH preferred)
- MODERATE — Discuss vaccination timing during rapamycin trough window (~2 weeks after dose, before next dose) with prescribing clinician
TOP CAUTIONS
- Do NOT add low-dose colchicine for inflammaging-CV risk (CLEAR SYNERGY NEJM 2024 negative)
- Avoid grapefruit / St. John’s wort during rapamycin window (CYP3A4 unpredictability)
- Aware of cumulative antiplatelet/anticoagulant load (aspirin + nattokinase + EPA/DHA + tadalafil) for any procedural/surgical context
- Separate doxycycline 20 mg from magnesium/calcium by ≥2 hours (divalent-cation chelation reduces absorption)
CROSS-REFERENCE PRIOR REPORTS
- IGF-1: IGF1 / IGF1R het signals; rapamycin alignment
- Rapamycin/mTOR: Direct overlap — rapamycin compensates IL2RA risk + augments vaccine response
- Glucose: Tirzepatide + Empagliflozin + Imeglimin context
- ApoB / Lipoprotein: 9p21 CAD risk fully addressed by statin/PCSK9/ezetimibe
- Endothelial: IL-6 + 9p21 → endothelial dysfunction; Telmisartan + Tadalafil supportive
- Inflammation/Immune: Direct overlap — IL6/CRP/EPA-DHA convergence
- Pharmacogenomics: FCGR3A F/V chart-flag for future therapeutic mAbs; CYP/SLCO1B1 cross-ref
- Mitochondrial: Ubiquinol form / NQO1 cross-ref
- Homocysteine: MTHFR / B-vitamin form cross-ref
LITERATURE FRESHNESS
- Report current through May 2026
- Suggested next refresh: November 2026 (6-month cadence; ZEUS readout window, TRIIM-X publication likely)
- Earlier refresh triggered by: ZEUS readout · TRIIM-X publication · medication change · abnormal hsCRP/IL-6/GDF15 baseline · CMV serology result