Dr. Fahy born in 1950…so he’s close to 76 years… looks damn good.
Appreciate his slides.
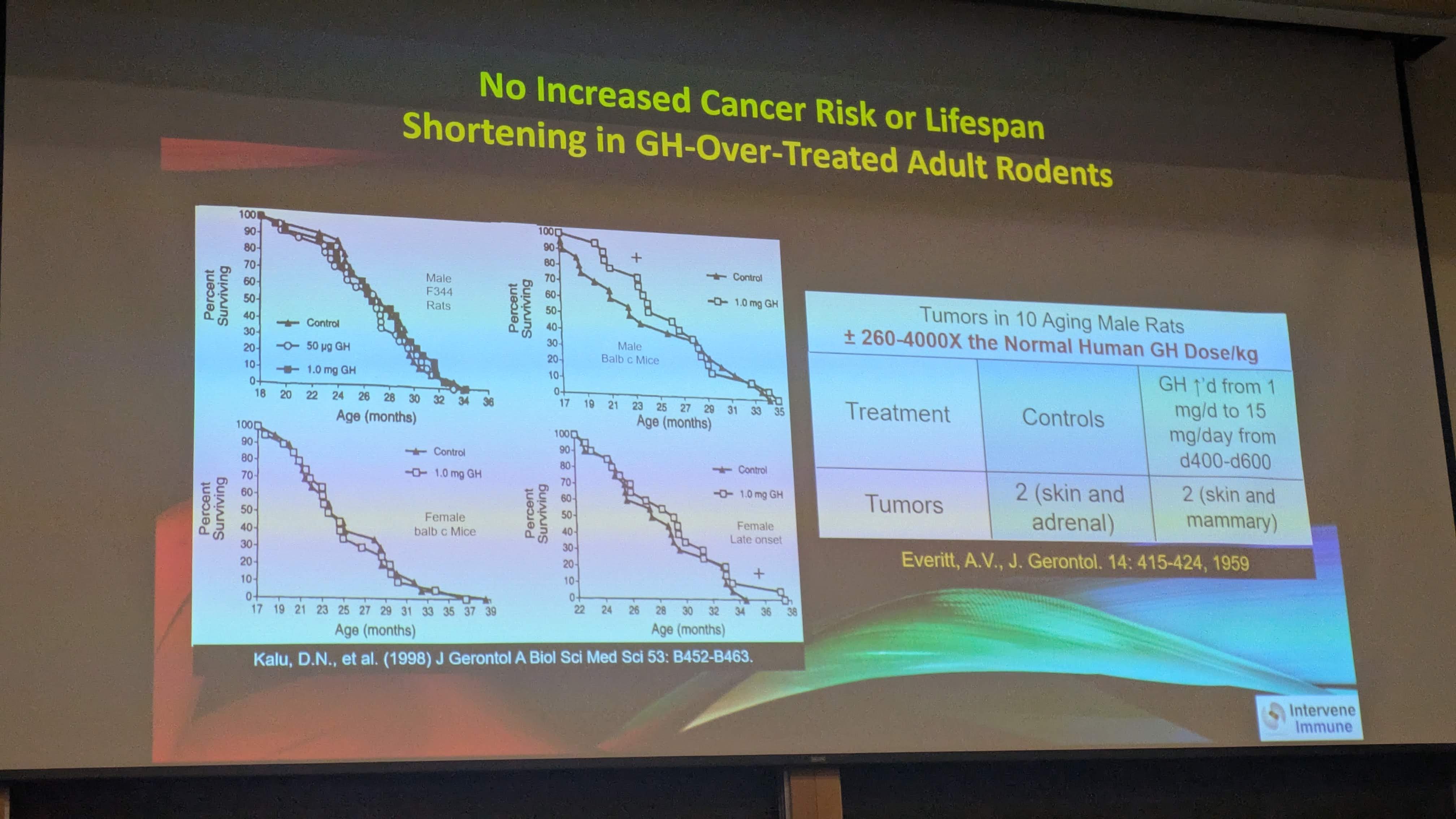
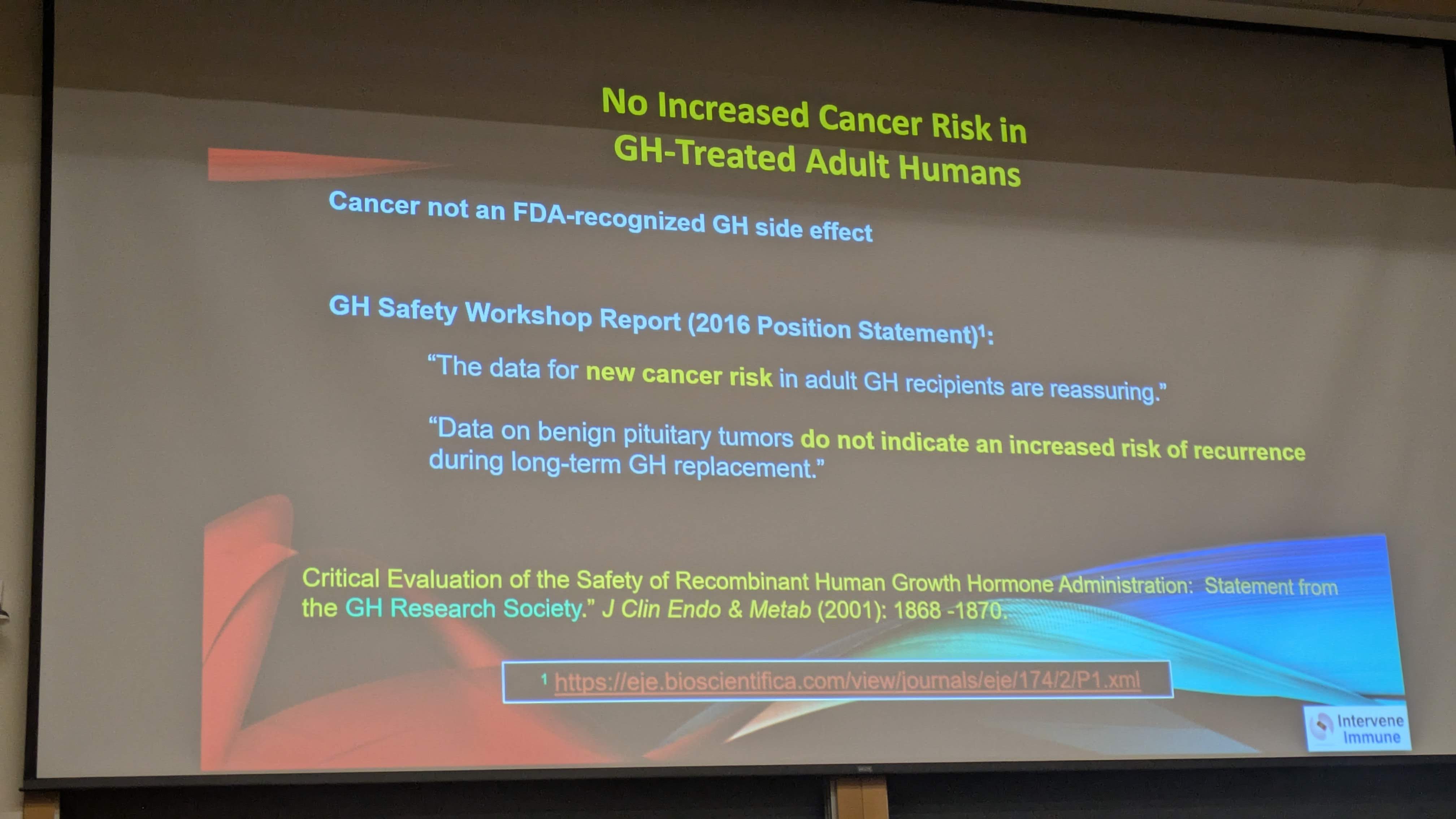
Like the no cancer risk report from GH use.
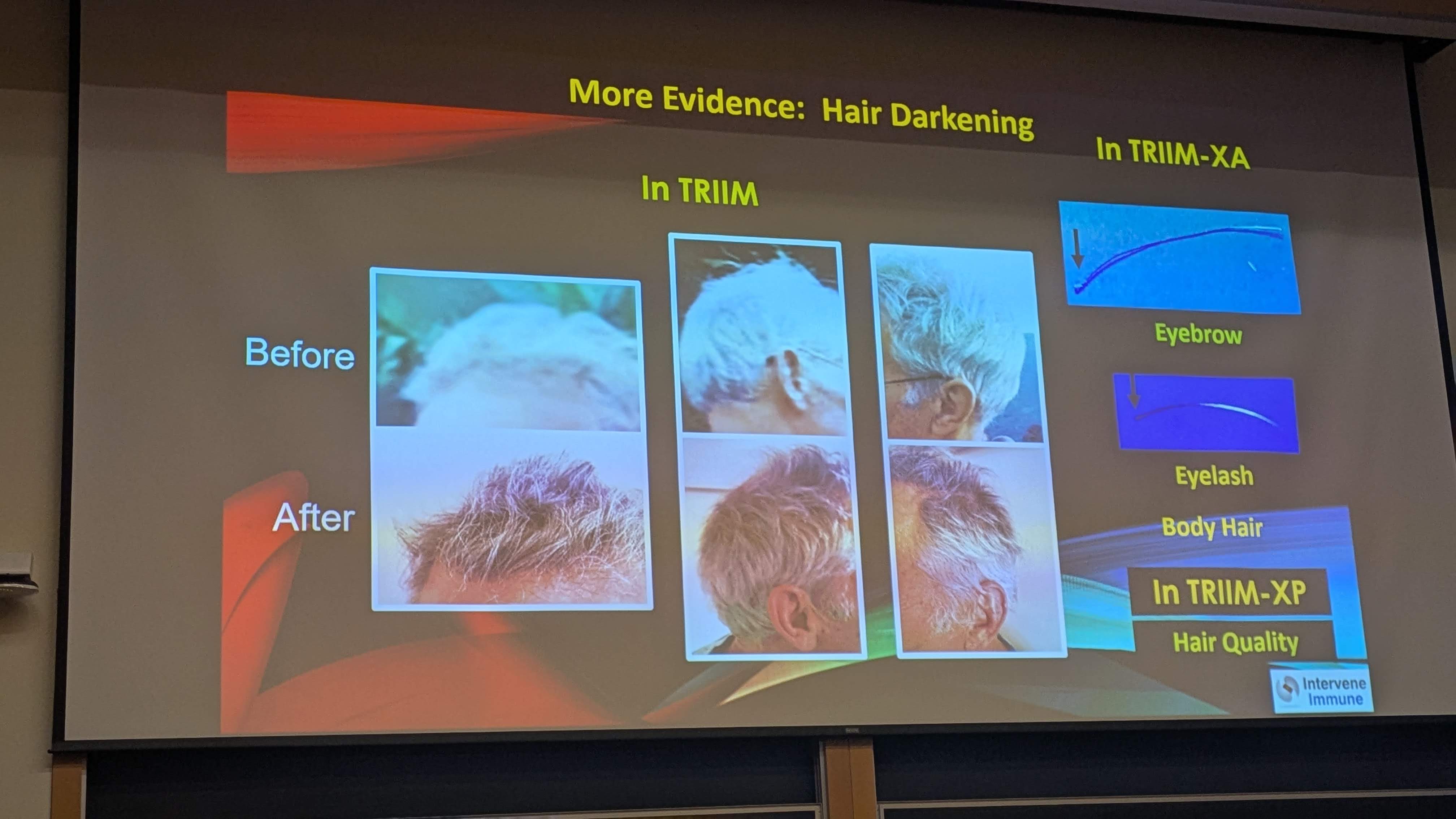
I concur on body hair growth… thick, long and dark hair. Arm hair like sasquatch… amazing. Medical professionals say hair growth is a good sign of health.
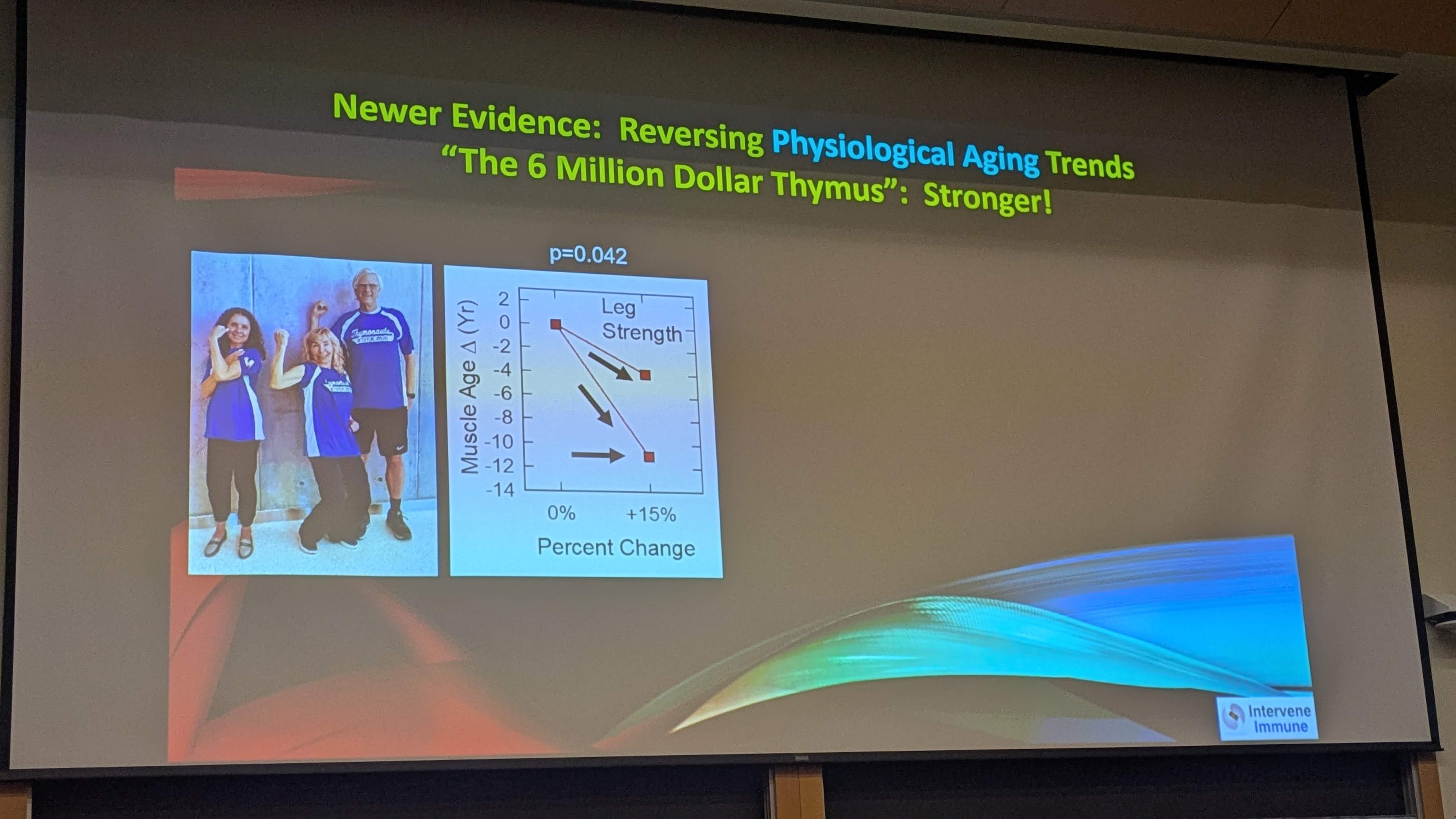
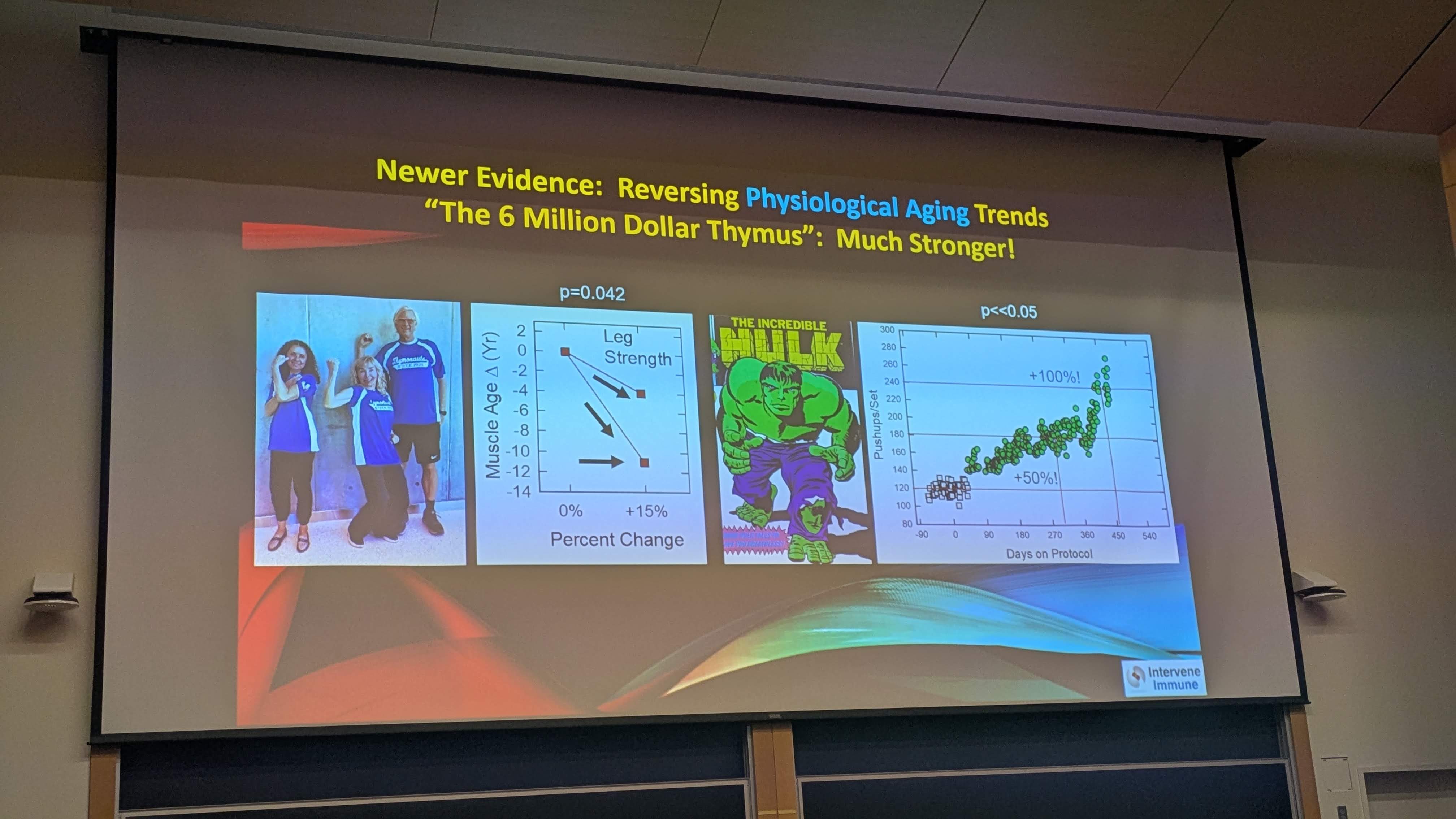
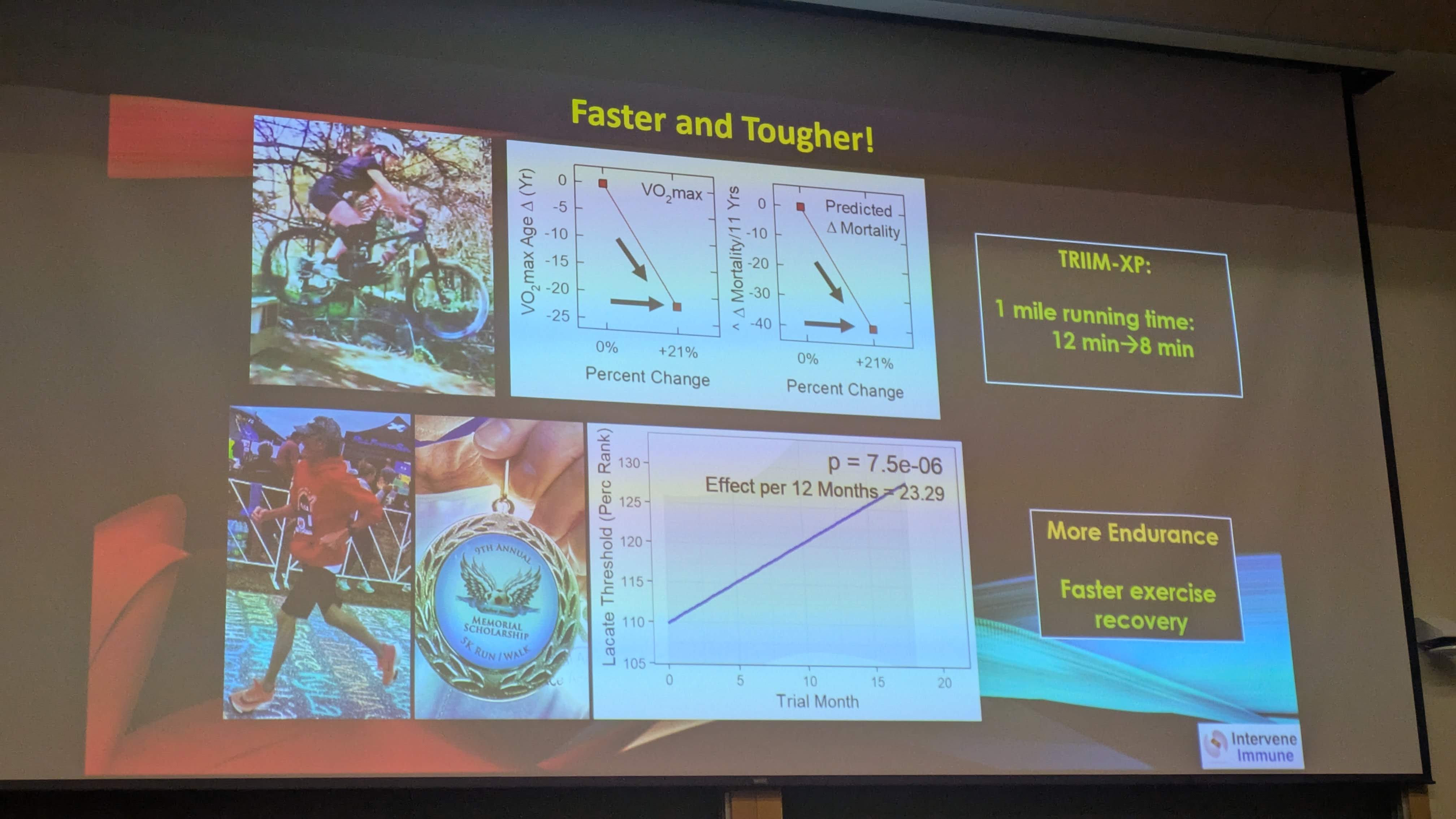
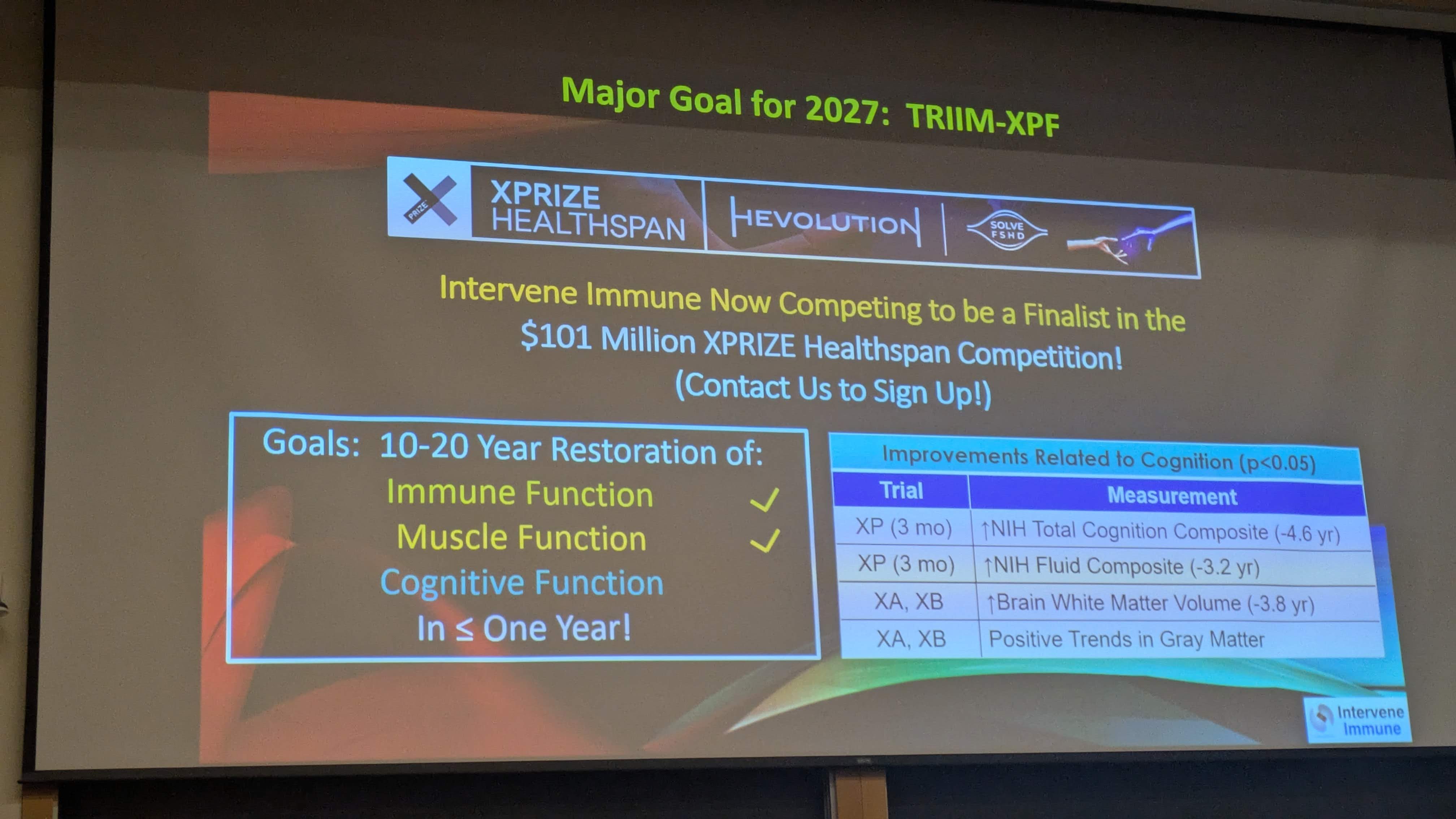
The gain of 10-20 year muscle and cognitive benefits are excellent. Immunity benefits and weight loss. I think my year plus dosing of HGH has been extremely beneficial to my longevity goals.
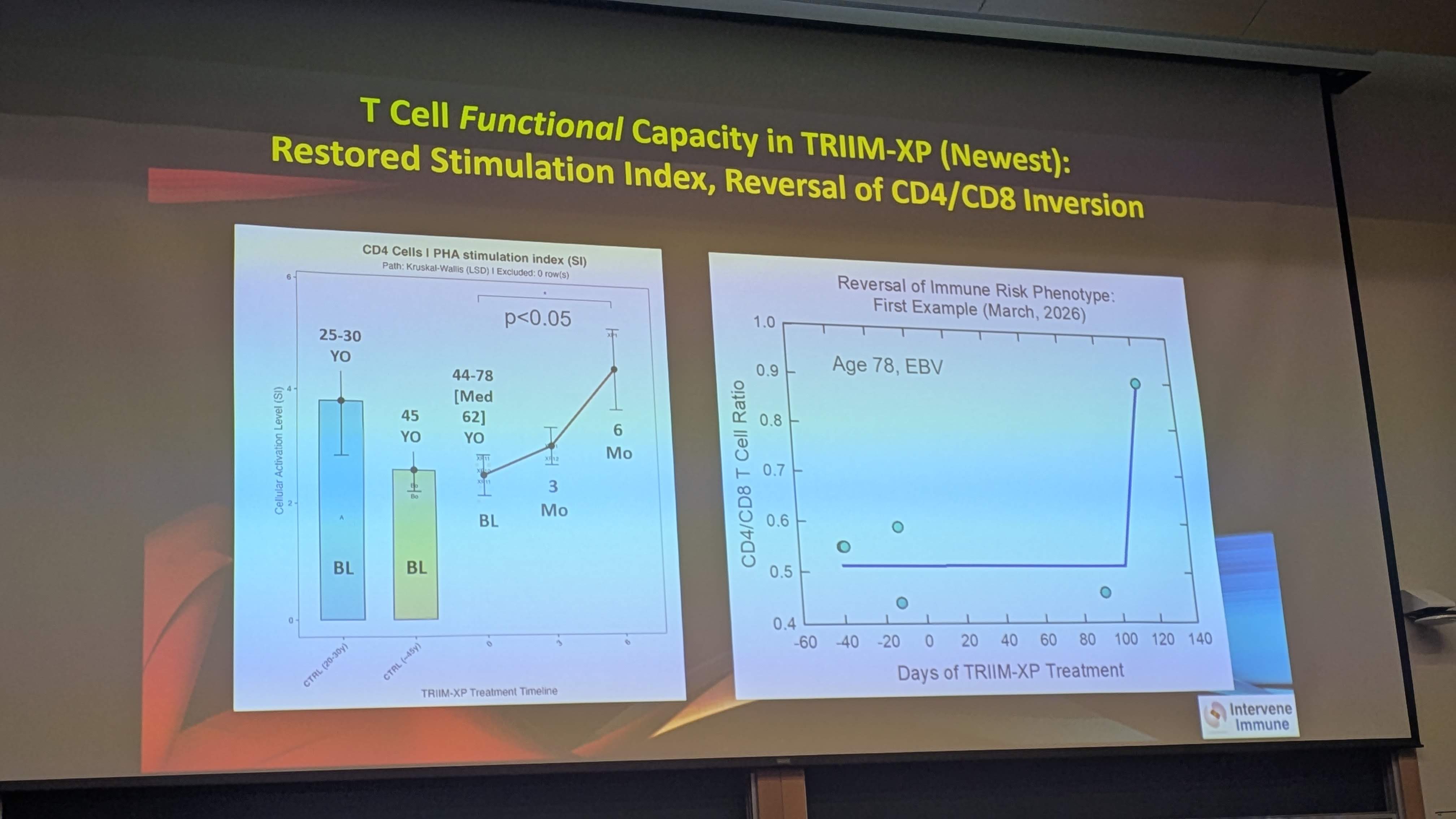
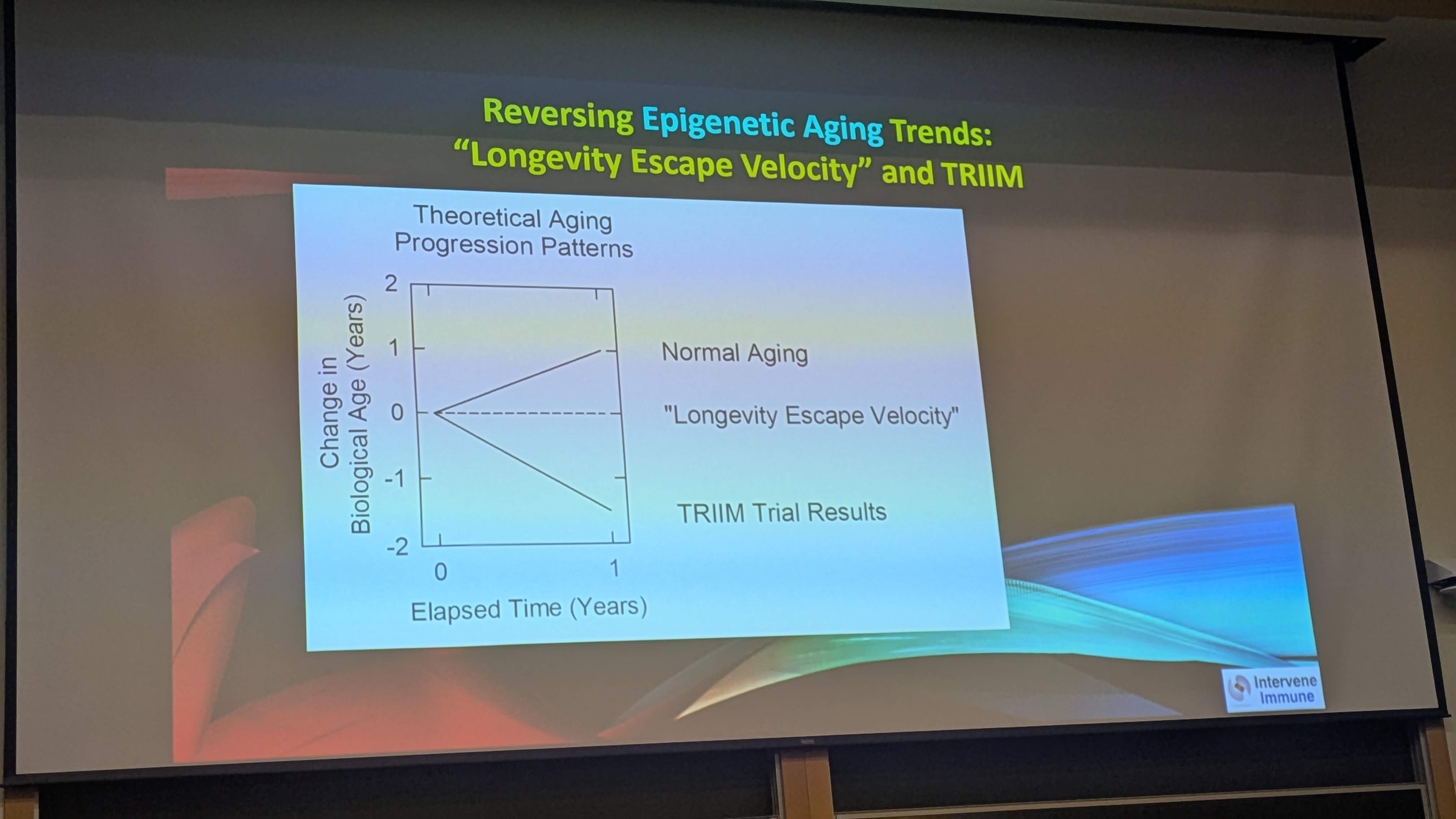
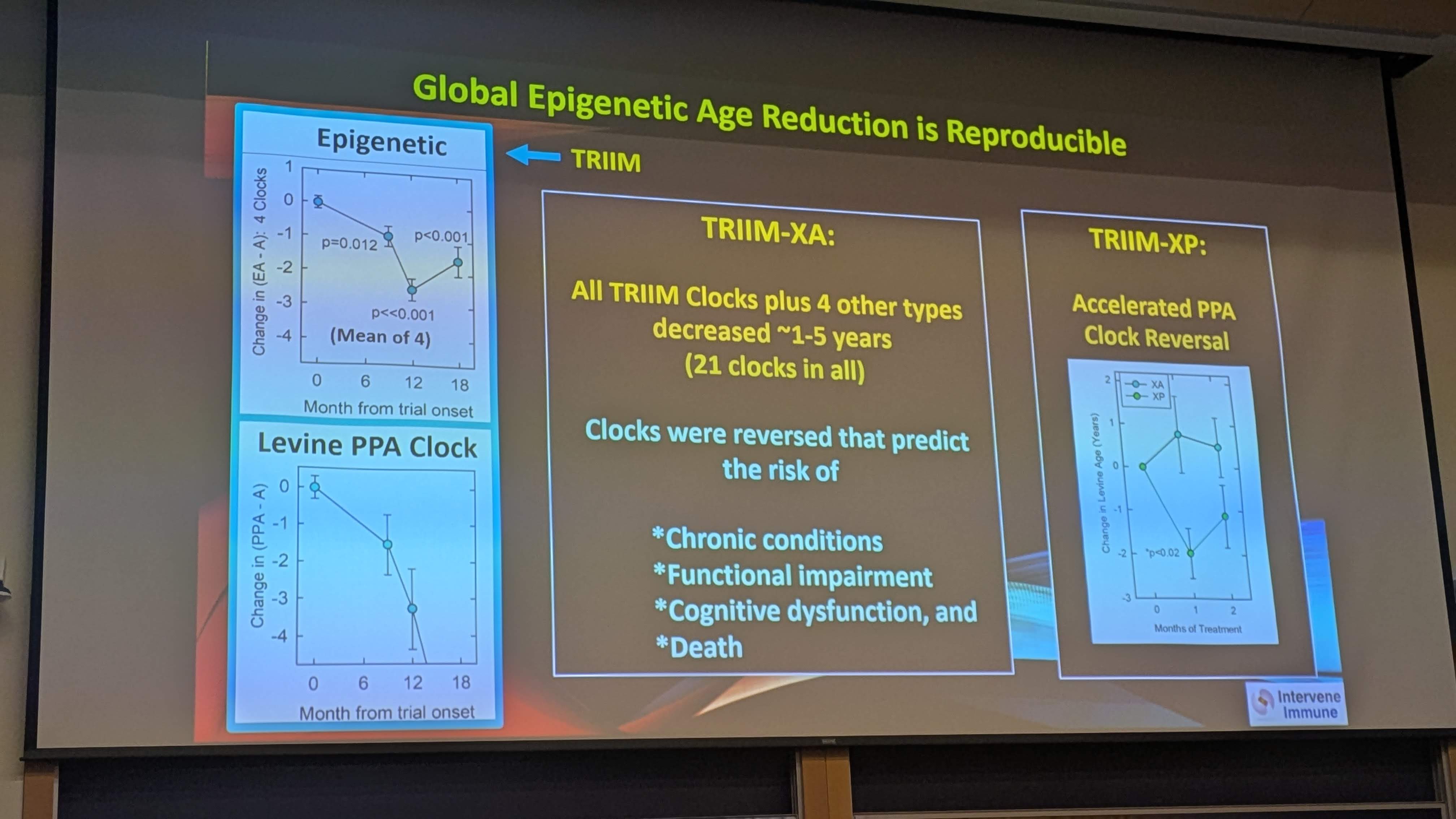
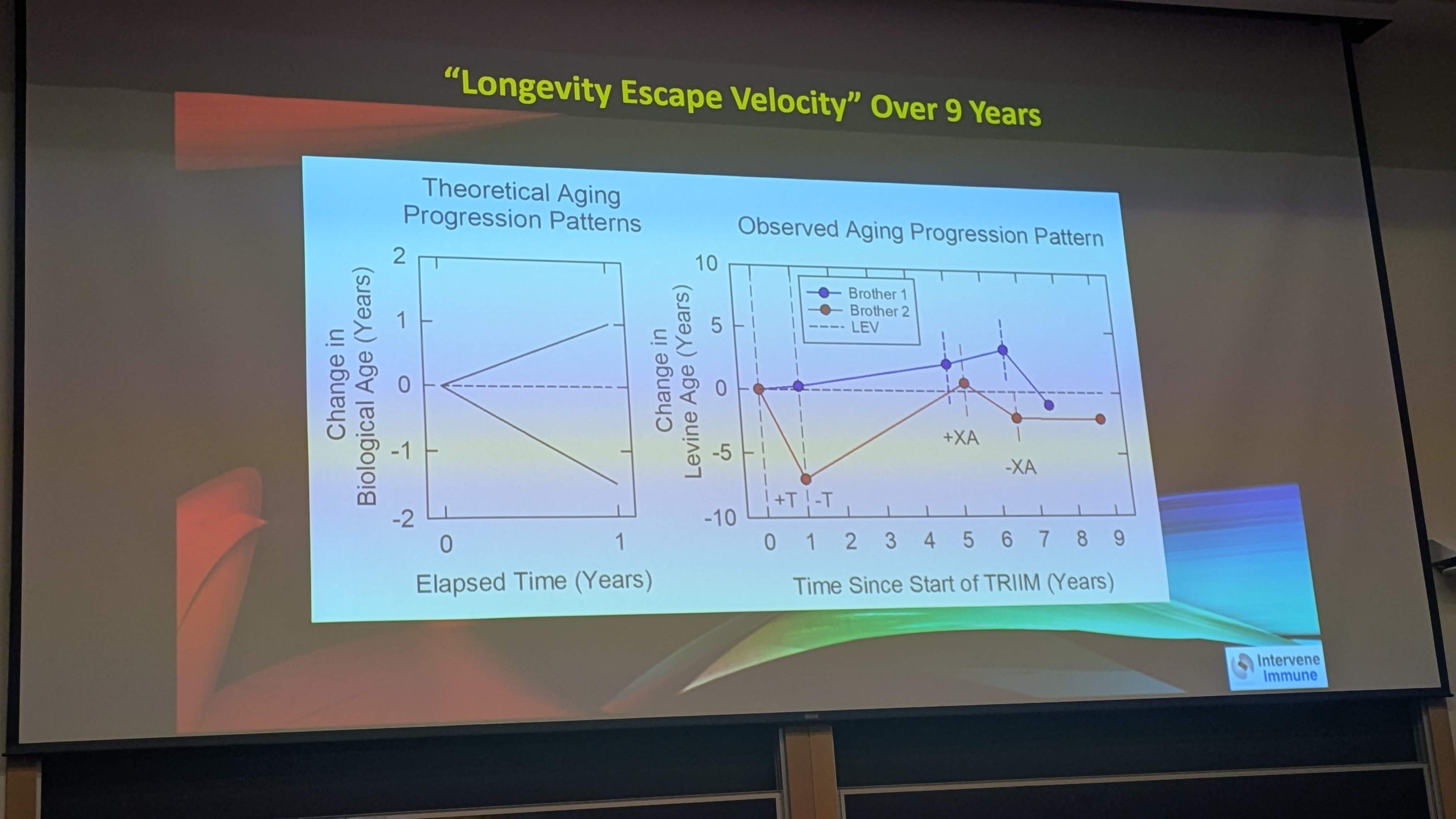
Fahy likes those acronyms TRIIM and series letters XA - the latest XP?
He looks amazingly good. And not in a “lots of work done” sort of way. That’s why I took and posted that photo. He says he has no time for bio hacking so only takes a few supplements. Recently he says he added a chin-up bar in the doorway of his office so he can do a little more exercise than he normally has done.
Its interesting… during a break I was standing with Greg Fahy and Irina Conboy, as Irina was asking more detailed questions about the study, and providing her input as an Immunologist (Greg is not an immunologist, so Irina understands a lot of the immunology science in this area better than Greg F., it seemed.
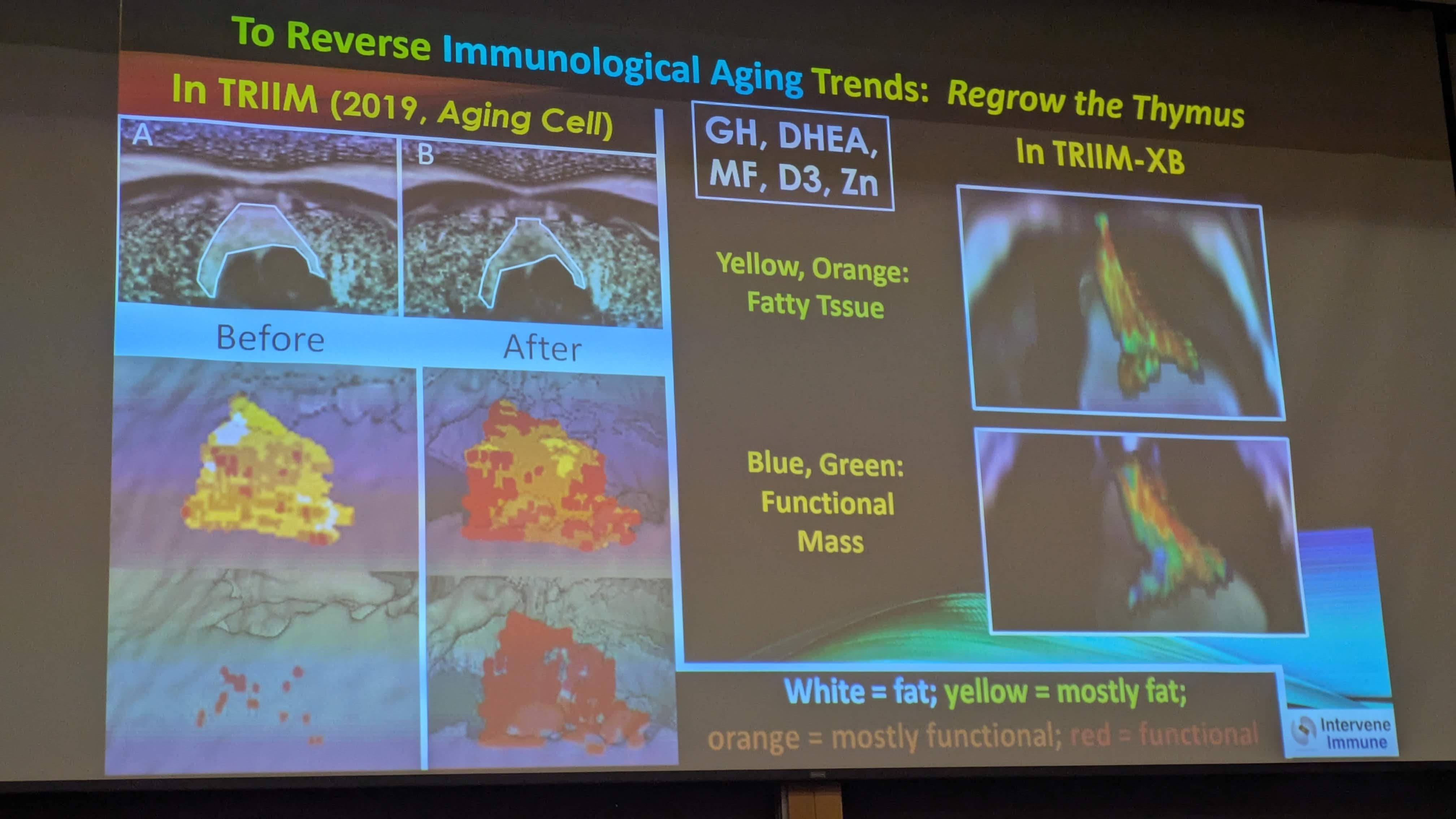
Irina Conboy said that while the results may be real, and the therapy may work, she was not convinced that he had regrown the Thymus. The n was too small, the measures too imprecise and limited, etc. And she has very little trust in the biological clocks that were being used, and how the testing was done. Moreover, she suggested that (I believe) that the first signs of immune system aging is actually in bone marrow. She suggested that perhaps the formulation (GH, etc.) improved the immune situation in the bone marrow, instead of the thymus.
And, it has to be said, that Greg Fahy has more than a purely academic role in this study. He’s working to build a biotech company based on this research, so there is a financial incentive.
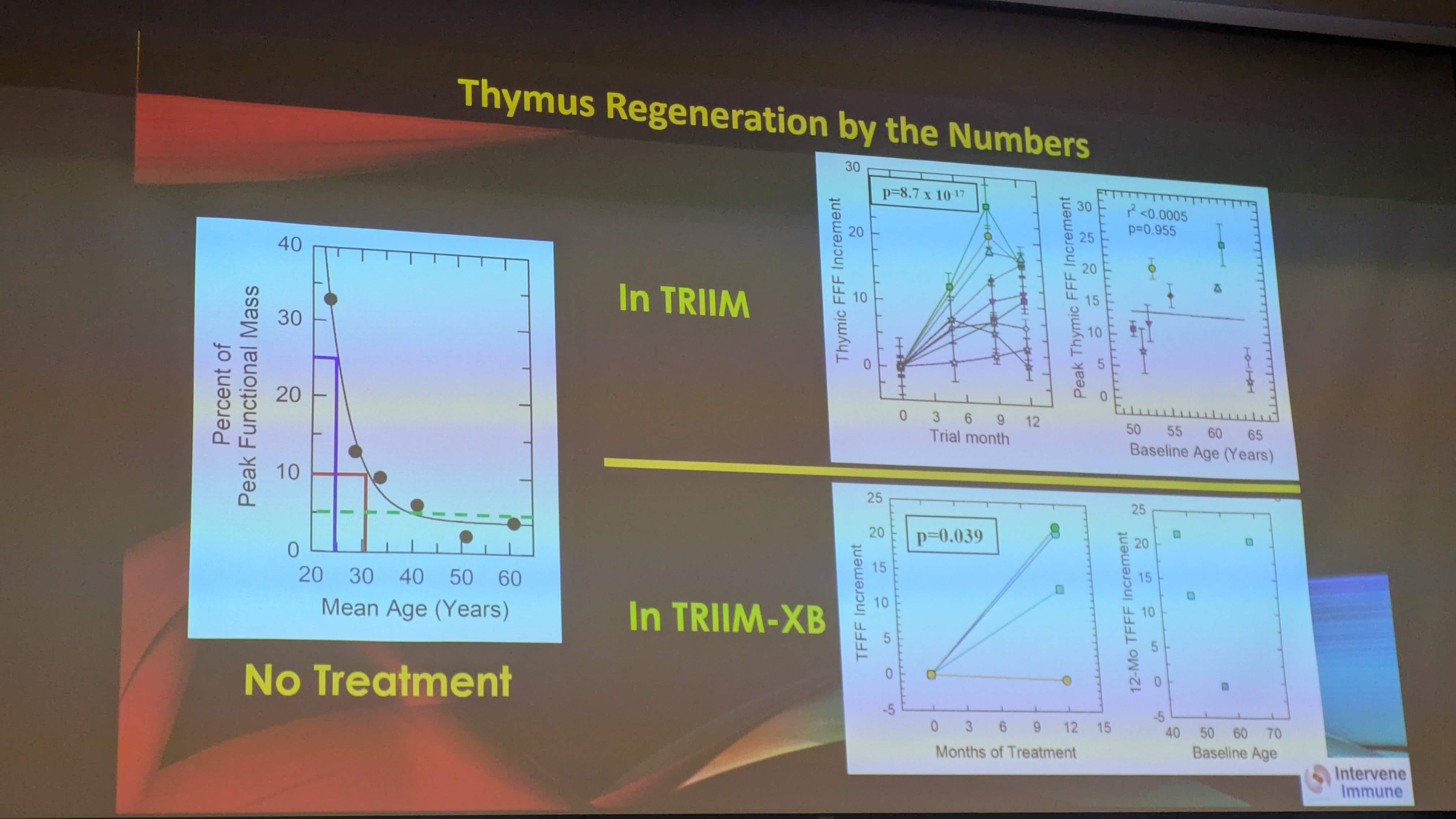
A new machine learning algorithm for looking at thymus health (i.e. not just size, which can be affected by fat etc). Sadly the algorithm is closed source, and the authors will commercialise it. I am imagining that it will be like a Cleery for thymus, where the imaging and data analysis will be done as a package.
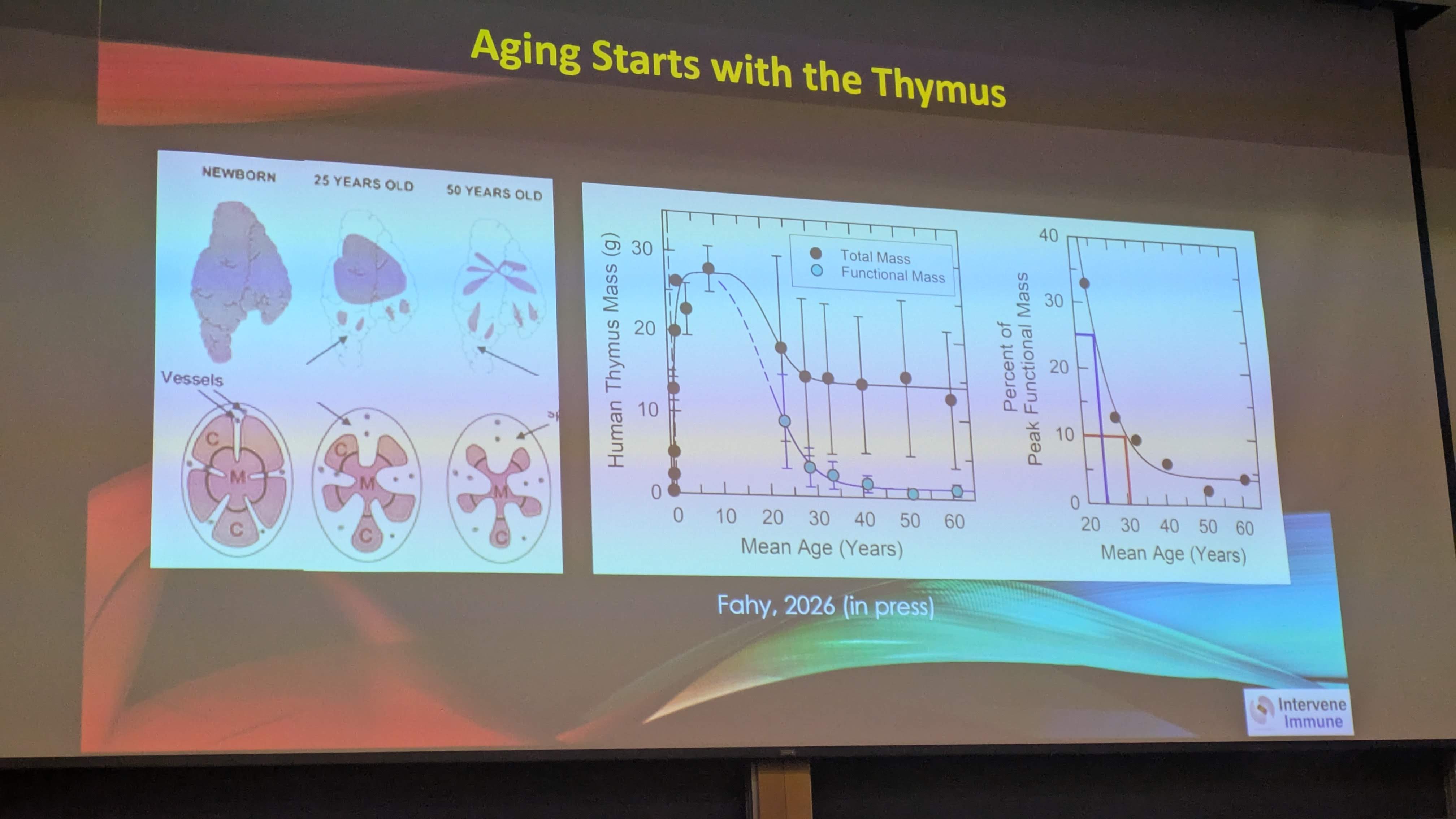
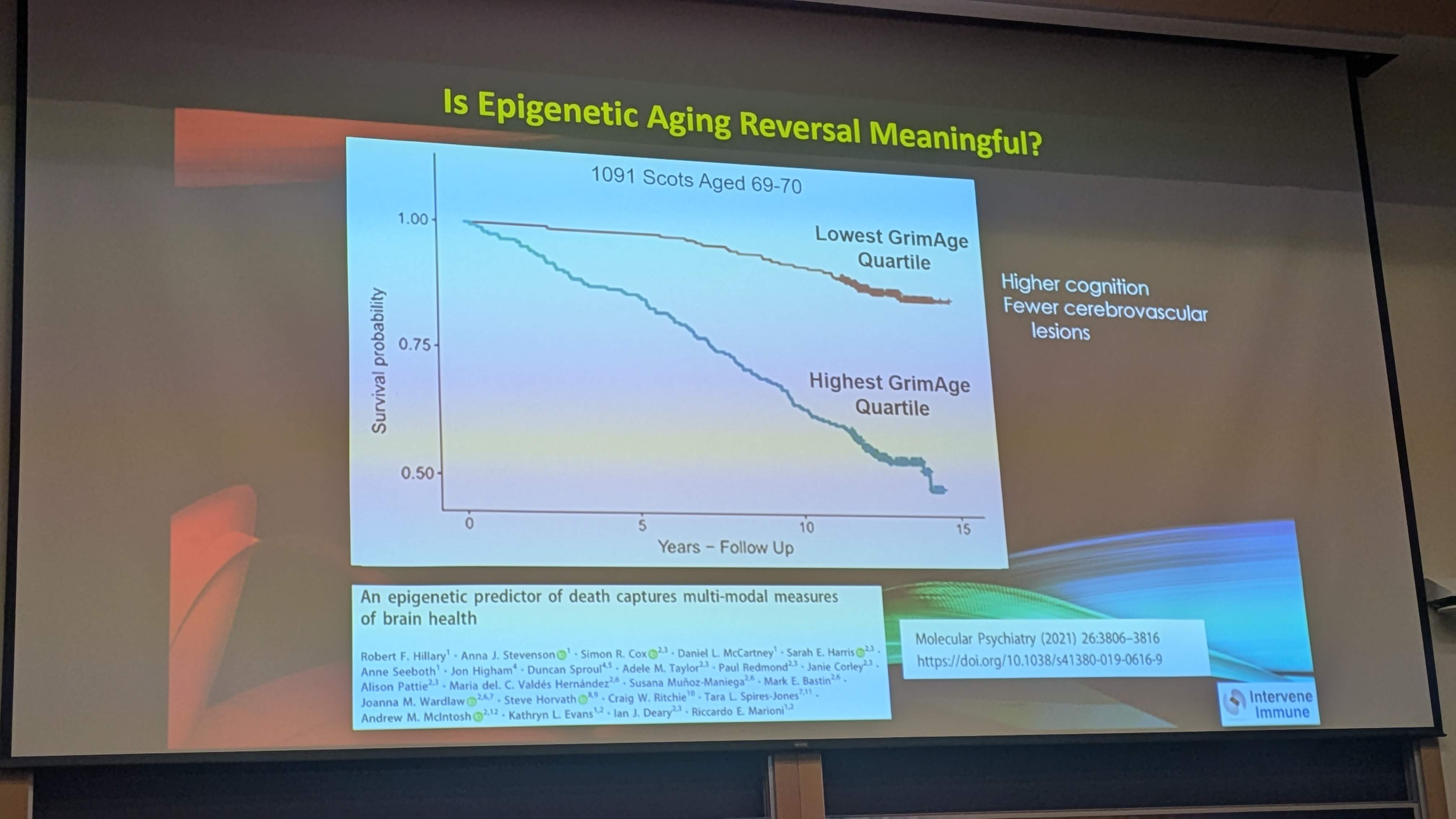
Thymus seems very important for population-level outcomes. Better thymus means lower all-cause mortality etc. However, it’s massively confounded by being healthier and younger (since all the things that make your thymus worse make your general health worse too)
The second paper is about immunotherapy, and I think unsurprisingly, those with better thymus function experienced better outcomes from cancer immunotherapy. This was consistent across multiple cancer and immunotherapy types, and could be used to predict patient responses. There’s no strong causal explanation provided, but IMO the correlation is strong enough, and mechanism plausible enough that it doesn’t really matter. What would be SICK is doing some sort of TRIIM-style intervention and improving patient responses to immunotherapy.
Personally, I am still a bit skeptical that anything can truly regenerate the thymus (but I would LOVE to be proven wrong). However, I definitely think we can slow down the involution, by doing all the things we already do - not smoking, exercising regularly, staying a healthy body weight. lower inflammation etc.
Lastly, the slides look interesting, but it’s maybe a bit misleading to say that cancer isn’t a GH side effect. I don’t think cancer initiation is the issue. The issue is that if you do happen to get cancer, GH/IGF-1 can promote the speed of growth.
Still, I’m really happy that people are working on this stuff.
In the Optispan - Kaeberlein and Fahy interview… both indicated rapamycin hss an effect on the thymus, in a positive way. So, if not by HGH… perhaps it’s rapamycin that clears the adipose tissue out of the thymus… much like iit does to visceral fat…after 3 months, starts clearing the visceral fat out of whole body.
Regardless of which it is… my thymus is rocking based on the CT scan imagr.
Both bonne marrow, and thymus interact, since B and immature T cells come from marrow (the source), and the thymus is where T cells mature.
According to AI, the scenario suggested by Conboy would look different than what data Fahy claims to have
What happens if only bone marrow is being rejuvenated
If the bone marrow “pushes” more T-cell precursors (progenitor cells) into the system while the thymus remains “closed for business” due to involution, the result is a massive bottleneck.
The immune system doesn’t just “work anyway”; instead, it creates a specific set of clinical problems. Here is the breakdown of what happens:
1. The “Traffic Jam” of Progenitor Cells
The bone marrow produces Pre-thymic Progenitors. These cells are essentially “uneducated” and cannot fight infections on their own.
Without a functional thymus to receive them, these cells either die off prematurely in the bloodstream or are redirected to other tissues.
They cannot spontaneously turn into functional T cells in the blood; they require the specific microenvironment of the thymic cortex to transform.
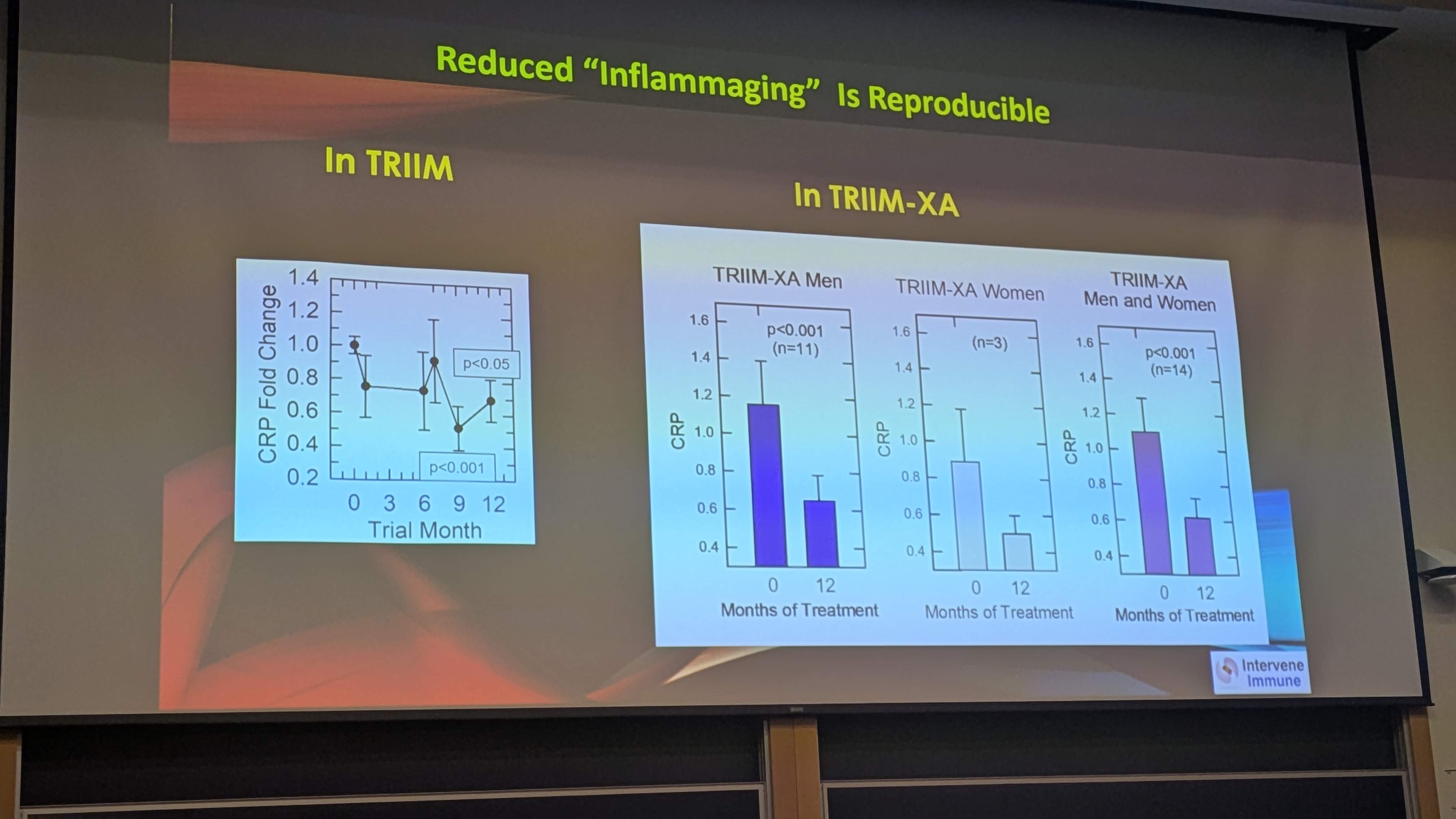
2. Accumulation of “Inflamm-aging”
When the bone marrow is overactive but the lymphoid pipeline (the thymus) is blocked, the body often defaults to producing more Myeloid cells (neutrophils and macrophages) instead.
The Result: An increase in systemic, low-grade inflammation.
This imbalance is a hallmark of aging. You end up with an immune system that is “loud” (highly inflammatory) but “clumsy” (unable to target specific new viruses).
3. The Rise of “Extrathymic” T Cells (The Low-Quality Backup)
In cases of severe thymic involution, the body sometimes attempts to mature T cells in alternative sites, like the gut lining (the intestines).
The Problem: These “extrathymic” T cells are like soldiers who skipped basic training.
They are often less efficient at killing pathogens and, more dangerously, less disciplined. They are far more likely to attack the body’s own tissues, leading to a higher risk of autoimmune disorders.
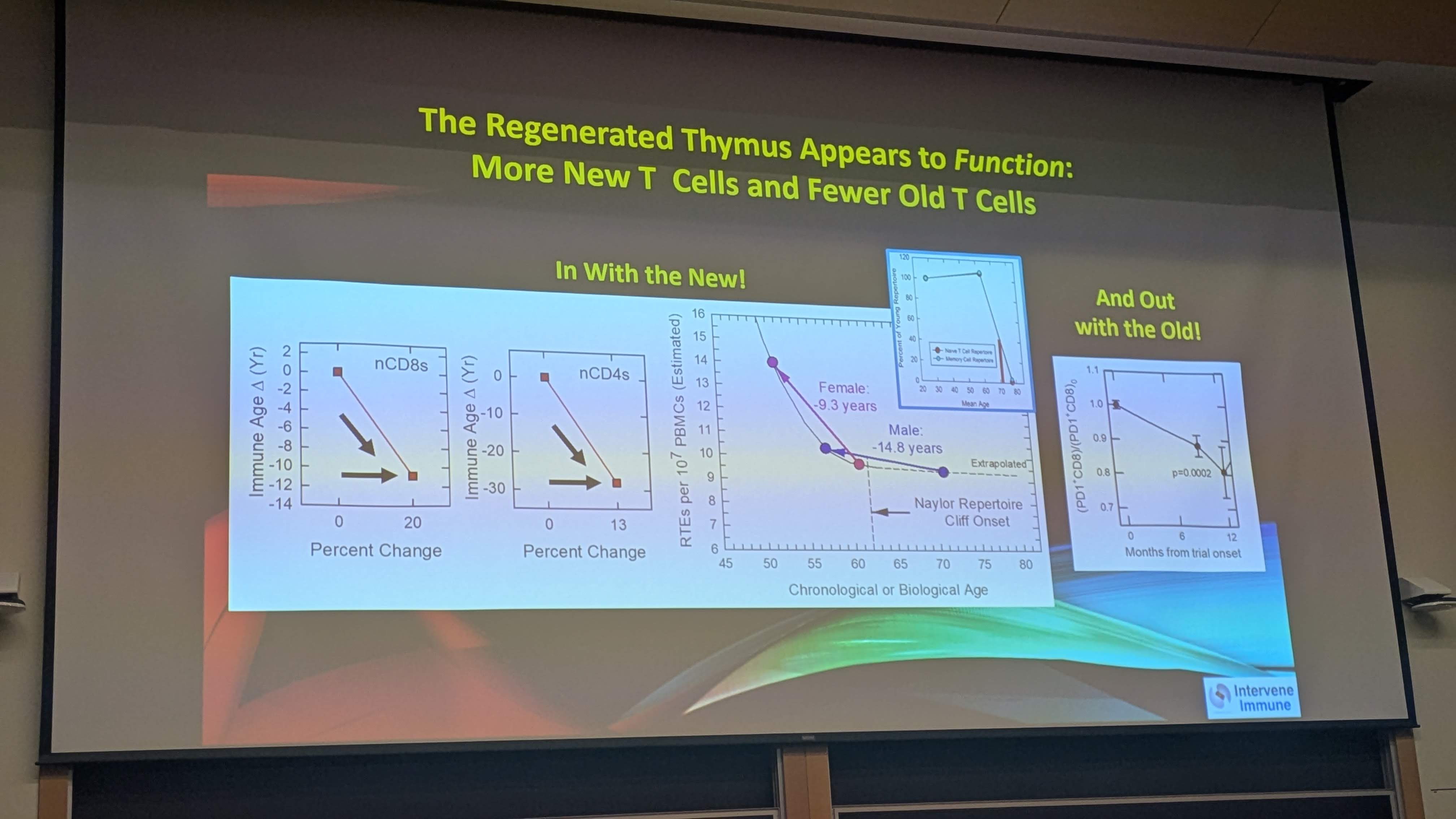
4. A Shrinking “T-Cell Repertoire”
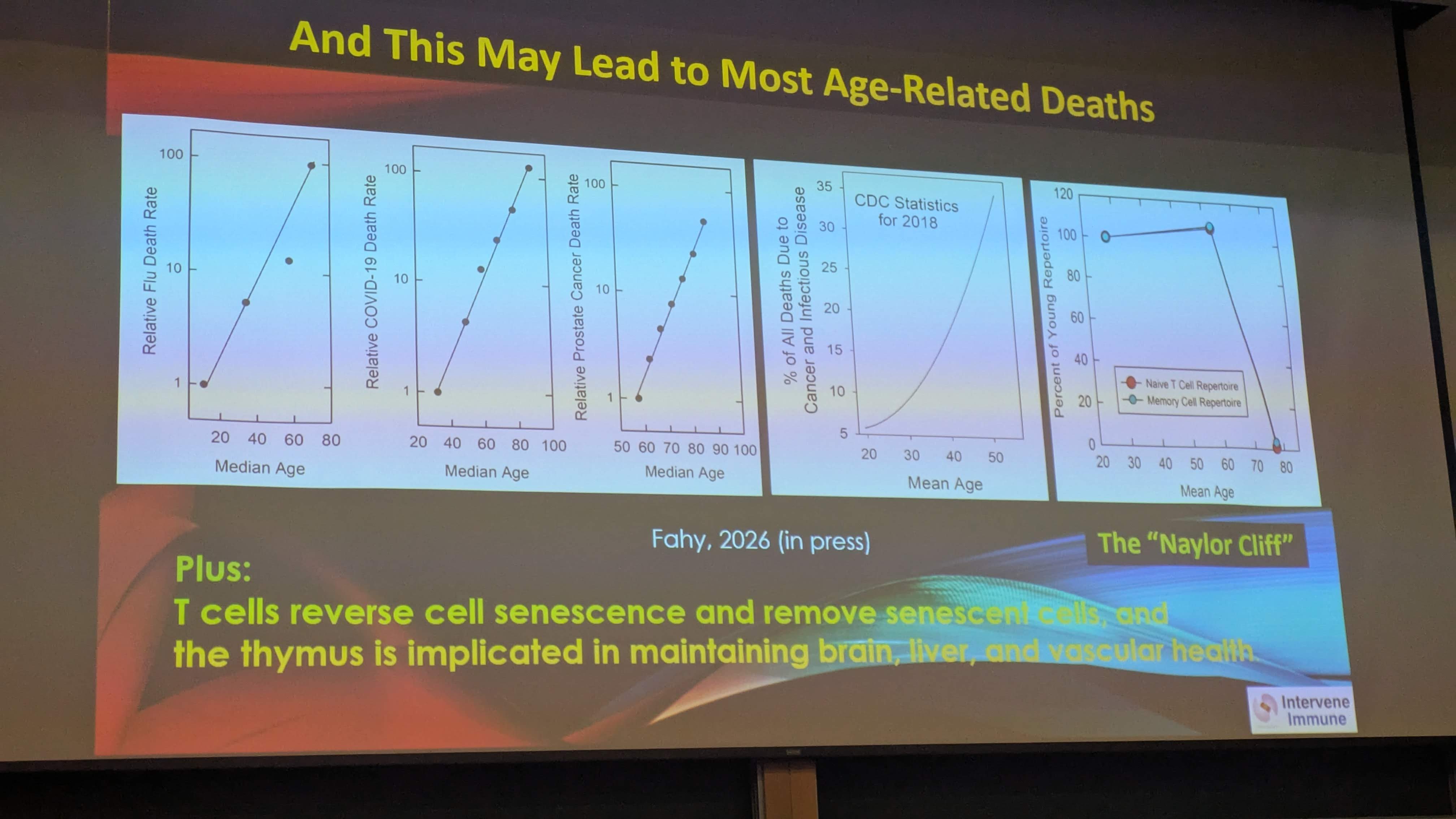
Because no new “Naive” T cells are being “printed” by the thymus, the body has to rely entirely on Memory T cells—cells that have already fought infections in the past.
The Result: You might be very well protected against a cold you had 10 years ago, but you are completely defenseless against a brand-new virus (like a new strain of flu or COVID-19).
The “library” of threats your body can recognize stops growing, even if the bone marrow is pumping out the “raw paper” (progenitors).
Summary Table: The Bottleneck Effect
Feature
Healthy Marrow + Functional Thymus
Healthy Marrow + Involuted Thymus
T-Cell Quality
Highly “educated,” precise
Uneducated or “rogue” (autoimmune)
New Virus Defense
Excellent (New Naive T cells)
Poor (No new recognition)
Inflammation
Balanced
High (Myeloid bias)
Analogy
Students graduating from a top university
Students standing outside a locked school
The Bottom Line: Increasing bone marrow output without fixing the thymus is like buying more wood for a furniture factory that has burned down. You end up with a pile of raw materials (progenitors) and a lot of smoke (inflammation), but no finished chairs (functional T cells). This is why researchers focusing on “immune rejuvenation” emphasize that the thymus must be restored for the bone marrow’s output to be useful.
That’s a thoughtful and fair perspective. I appreciate you sharing it.
Irina Conboy’s comments seem to get at the real issue: the findings may be interesting, but the conclusions may be stronger than the data currently support. A small n, indirect/imprecise measures, and reliance on biological clocks make it hard to be confident about claims like true thymus regrowth or meaningful age reversal.
I also think her point about bone marrow is important. If immune improvements occurred, they may not necessarily prove thymus regeneration. There could be multiple mechanisms involved.
The thymus absolutely seems relevant to immune aging and longevity, so I’m open to that line of research. I’m just cautious about jumping from preliminary signals to broad claims.
Same with GH safety discussions. Saying GH is “safe” based on tiny old animal studies (for example, a 1959 rat study done long before recombinant GH existed) seems like more confidence than the evidence warrants.
And it’s also reasonable to note that when someone is building a biotech company around a therapy, there is an incentive structure that can unintentionally bias interpretation or messaging. That doesn’t invalidate the work, but it’s another reason to keep standards of evidence high.
Interesting research area—just still a lot of unanswered questions, in my opinion.
May be a good example of:
Confirmation Bias: The tendency for researchers to selectively notice or interpret data in a way that confirms their preconceived beliefs.
Also, today I learned a new word: Apophany: Psychologists call the human tendency to see meaningful patterns in random data apophenia. The mind is a powerful pattern-matching machine, often finding correlations where none exist.
Exactly… only Dr. Fahy was fairly unfamiliar with off label dosing of rapamycin… he thought people were off-label dosing 6 mg daily. Matt corrected him.
Also, rapamycin clears the fat and compresses the thymus… so it is smaller when on rapamycin. Which is why Matt shared with me a 3 month washout would put my thymus at full size for a CT scan.
Fahy felt rapamycin might interfere with final T-cell review before being released… kind of its finishing step. So rapamycin might prevent the benefits of more T-cells.
Also, Fahy admitted rapamycin does something to improve nerve cells… but trying to keep his HGH protocols pure… stays clear of any rapamycin in his work.
Matt seemed very doubtful of rapamycin csusing issues and Fahy seemed to lack concrete evidence. That said, it would still make prudent sense if Fahy is right to do 2 -3 months on rapamycin… and 1 month break. So, T-cells are finished and released.
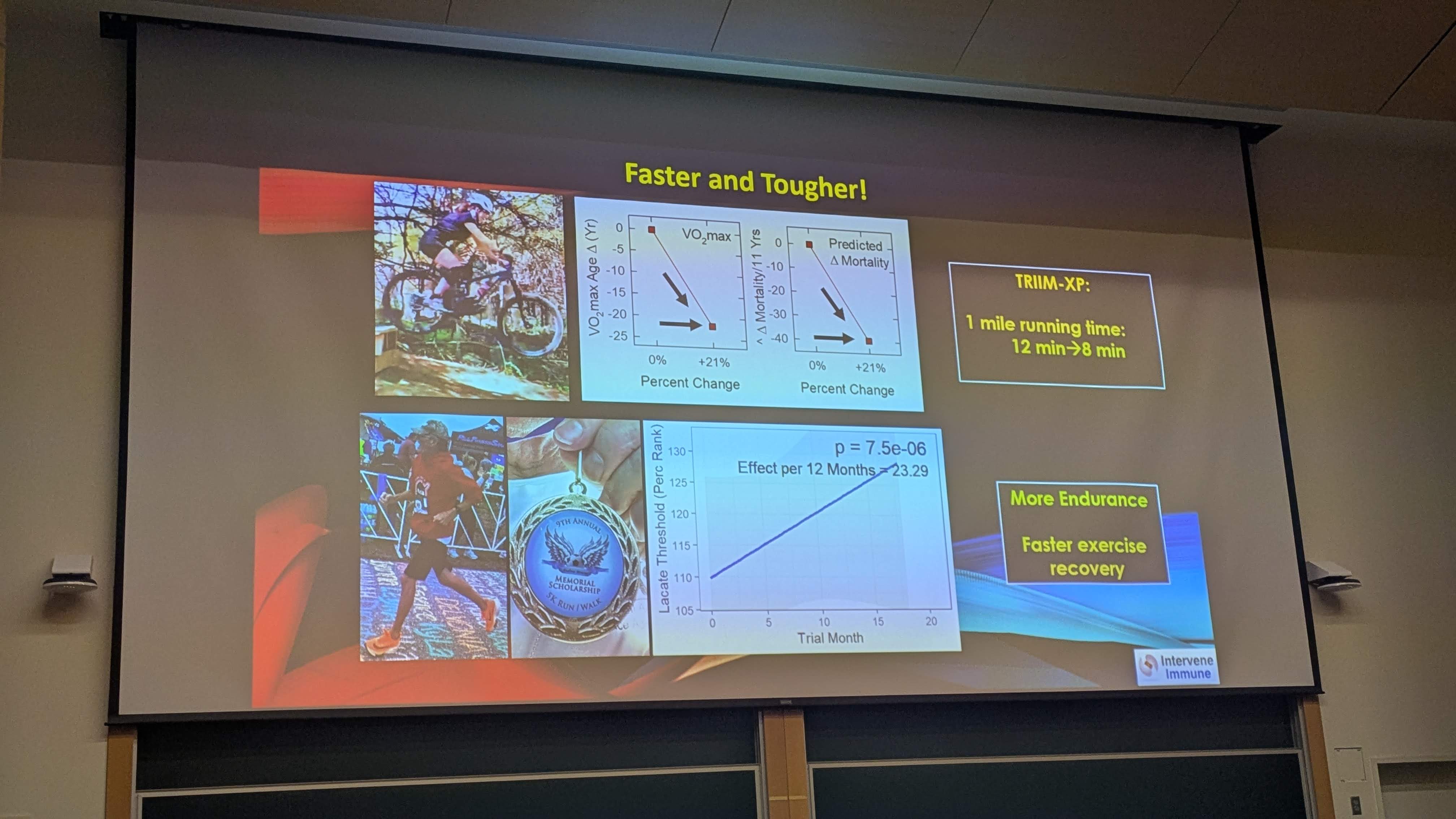
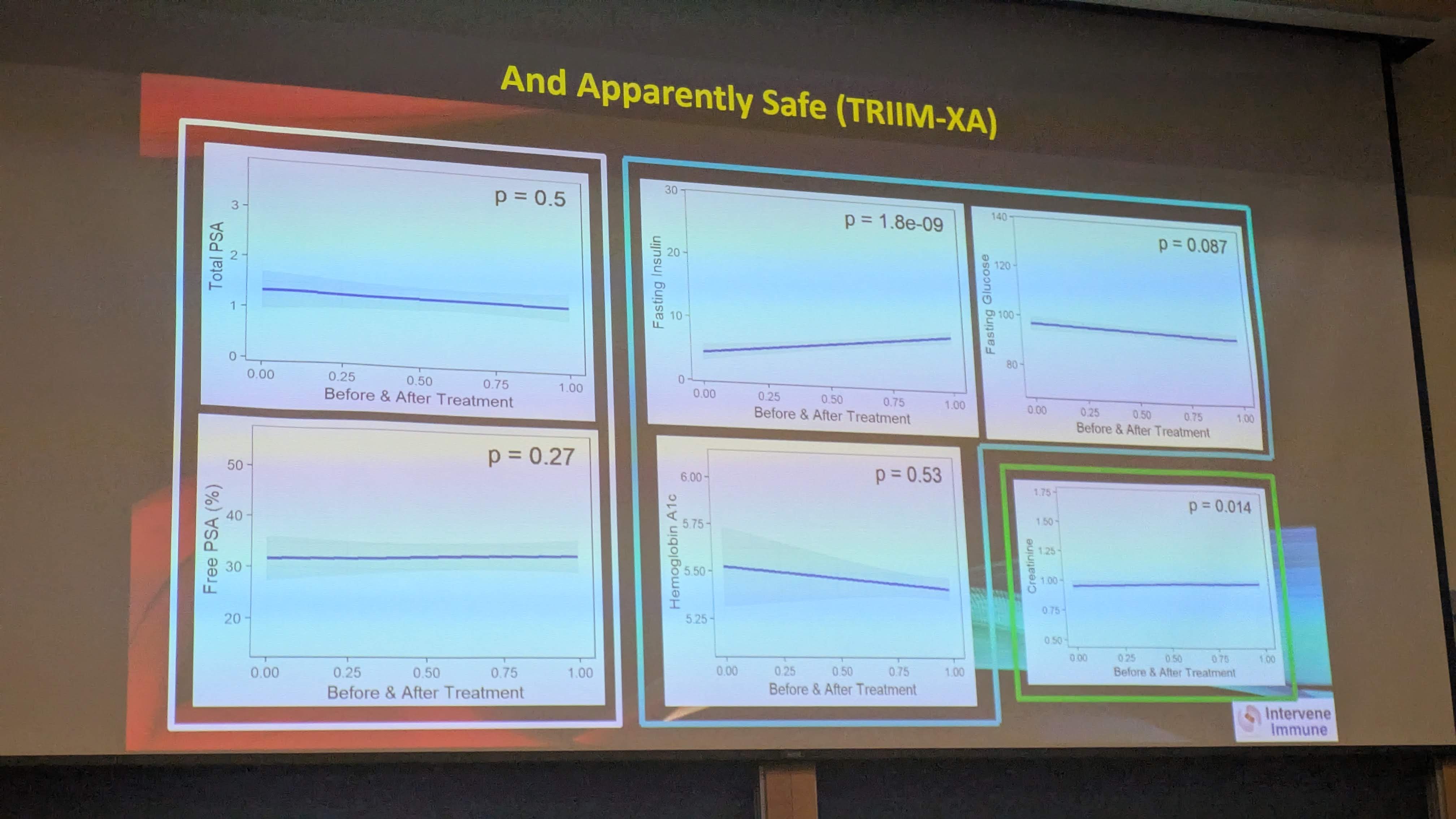
All this graphs with 4 data points, N=11, N=3 sample sizes, unreliable aging clocks correlations, rodent safety data. Missing information to be able to review the data and conclusions.
I’m fairly optimistic/hopeful for this area of research - whilst appreciating it has a long way to go.
The XPrize would be interesting - if they get to the finals then we’re looking at n>100 and some blinding (single or double both possible) with decently broad outcome metrics. But that’s at least a year away.
Did he give any hints as to his new protocol? He suggested that the new formula produces results in 90 days rather than a year