Rapa dosing.pdf (2.4 MB)
Lots to digest here. Enjoy.
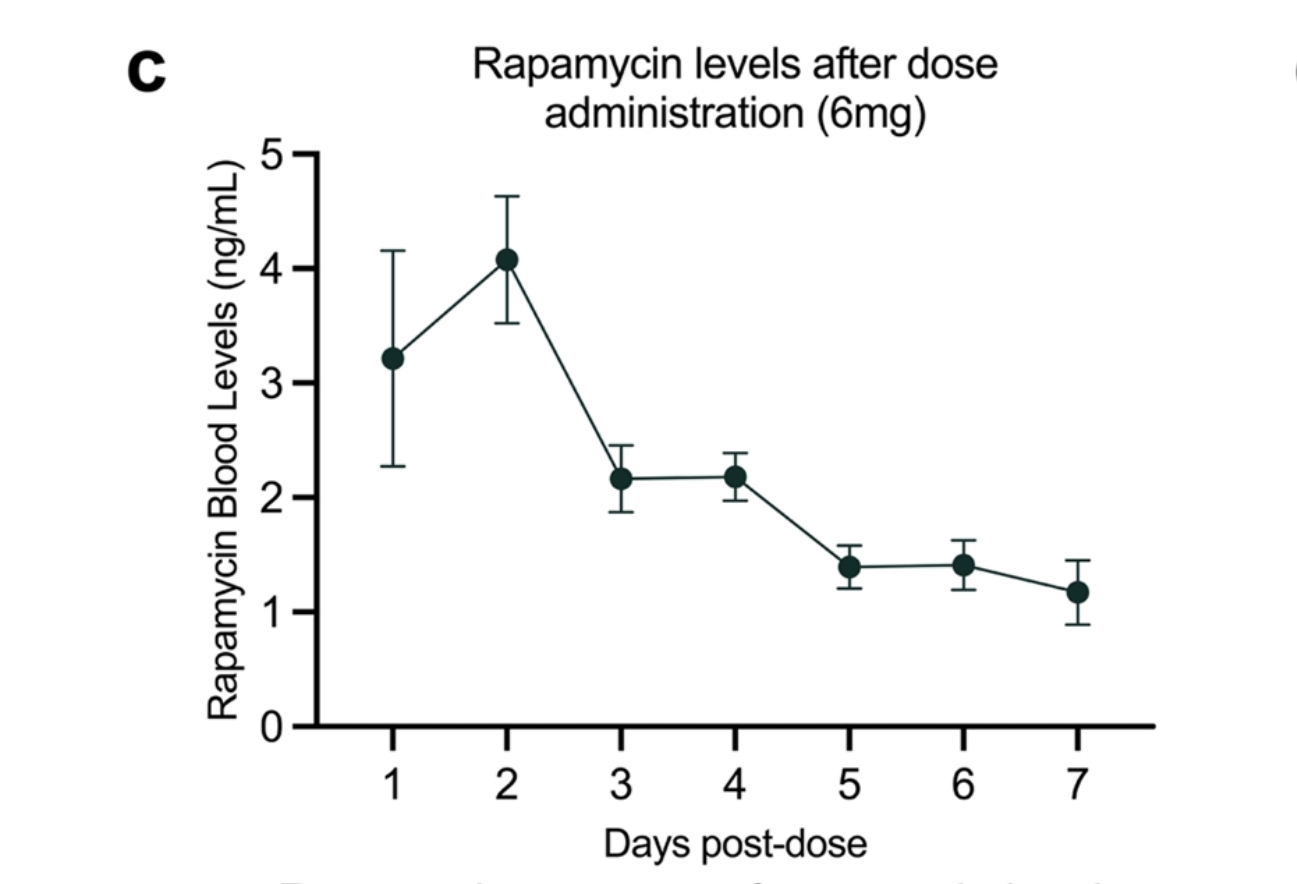
blood rapamycin levels peak after 2 days with gradual
decline thereafter
What?
That’s not what my labs showed.
Edit: I take it back. I didn’t get a 48 hour level. 23 hrs and 73 hrs. Guess I can’t say.
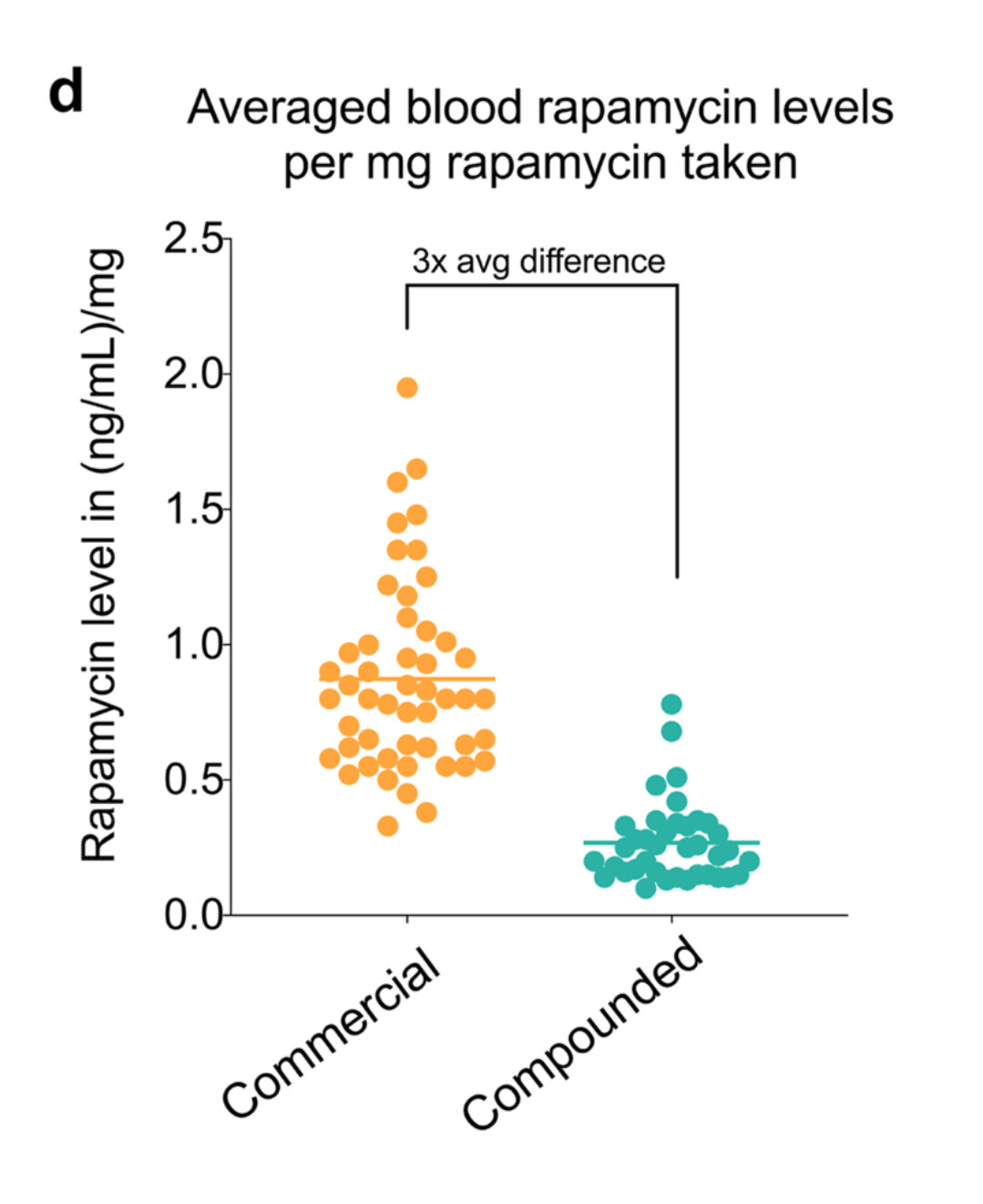
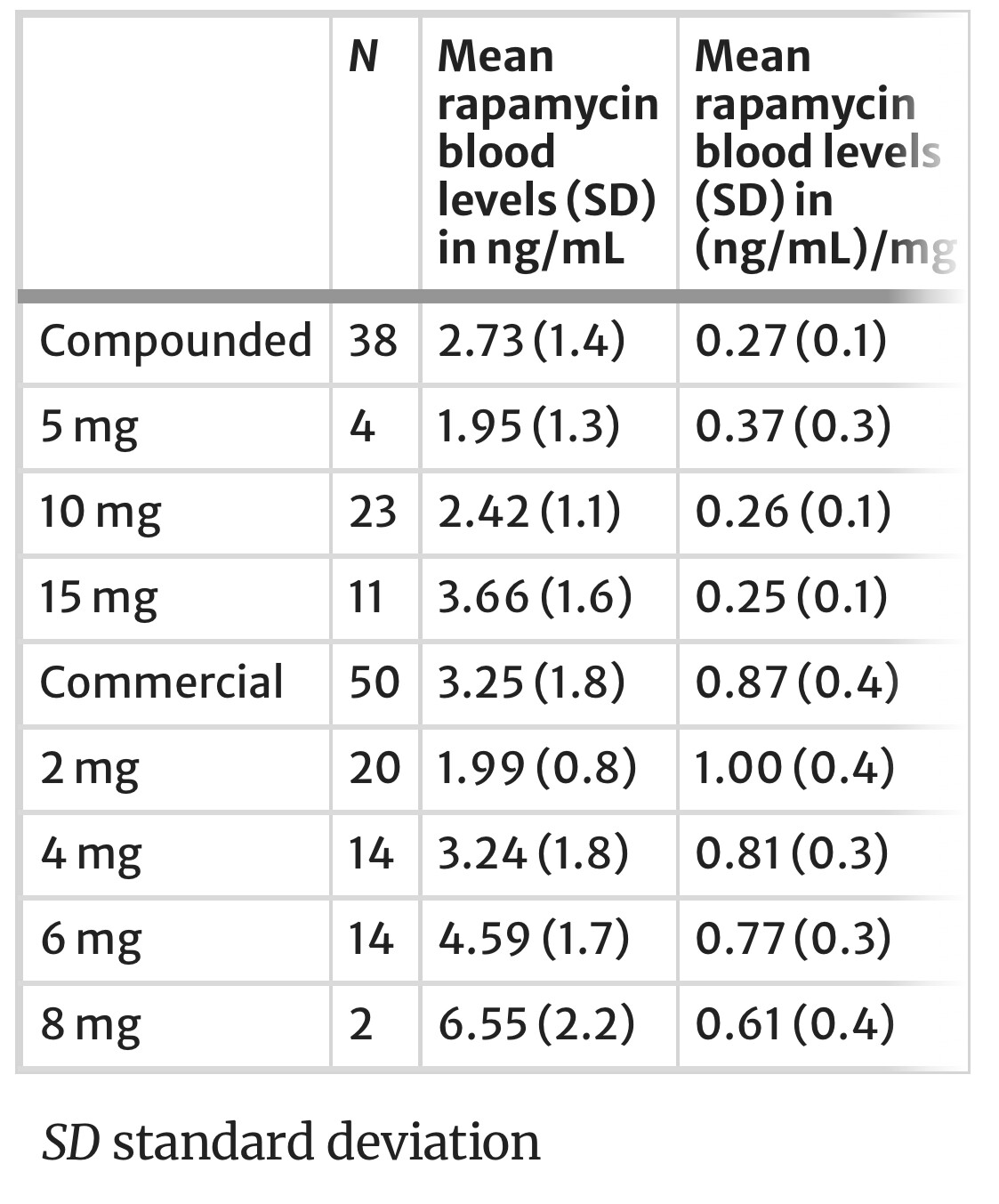
Well, at least they confirmed the 1:3 relationship between commercial pharma pill and compounded. Very nice find, Joe!
This chart says a lot. Measurements at 24 hours post dosing.
My conclusions for myself:
The question that hasn’t been answered is whether negative side effects (short term) are a sign of long term positive effects or whether negative side effects should be avoided
There’s a lot to ponder here. So much so, that it will take quite a while for me to digest this paper. One immediate reaction… test, test, and test again; if you’re not testing, you are flying blind.
The dosing question is very important, obviously. However, the most important one is a fundamentally different one: what does rapamycin do? It’s all very nice to know how much is present in the blood at what dose when and for how long. But unless you know what it does, how do you decide on what dose you should be aiming for?
This is where you need to combine the dosing question with outcomes. And the most obvious entry here is the PEARL trial. Unfortunately, the dosing range in that trial was rather limited, especially for men. We’re talking just under 2mg/week at the high end. And… not much to see here (for men). My conclusion is that a higher dose is probably needed to noticeably move the needle (in men). Yet the paper also gives us an interesting hint in that drastically diminishing availability curve. Could that be some kind of guide? Frankly I don’t know, but while experimenting with dosages and timing protocols, I know I must test my levels.
![]() wow is this study full of unnecessary complexities and assumptions rationalizing massaging the data to get to any result at all, all in order to (re)discover nothing else but that the enteric coating of capsules sucks? Or am I missing something?
wow is this study full of unnecessary complexities and assumptions rationalizing massaging the data to get to any result at all, all in order to (re)discover nothing else but that the enteric coating of capsules sucks? Or am I missing something?
There’s more than that in the paper. A lot more
Yes, I read it, it is a most torturous paper, but they themselves say they did not find much more reliable than that one thing, and even with that one they give no certain believable reason for it; what is it with the compounding? See, that is why I take it rectally, because compounding sucks, and we knew that without this paper.
Really good summary, thank you. I read the paper, not expecting to learn anything new, but I was happily wrong.
For the case of increasing levels on concentration of over time in subjects,
individuals
measured at two subsequent timepoints appear to
most commonly have the same or increasing blood
rapamycin levels, with higher magnitude increases
observed over 3 months than 2–4 weeks, and simi-
lar levels over periods longer than 6 months thereaf-
ter.
The graph for levels after 7 days seem to suggest that rapamycin levels never got to 0 for this population :
If that is the case, then this slow buildup of levels over long time periods would make sense.
Another fun part is the estimation of blood rapamycin levels based on dosage. It’s an approximation, but it’s better than nothing, and might save people from having to do blood tests in the exploration phase
Here is the formula they found :
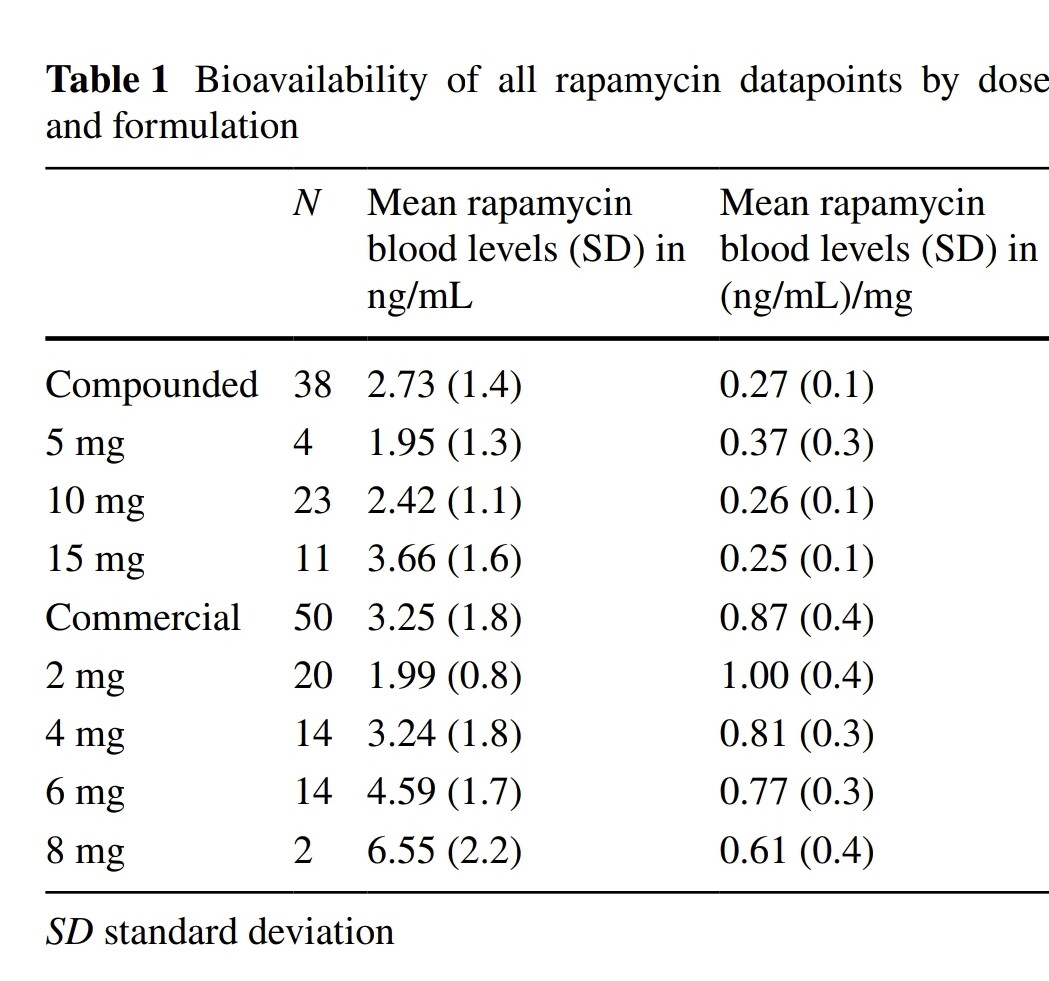
we estimated blood rapamycin levels of compounded to be 0.27 ng/mL per 1 mg dose, and commercial to be 0.87 ng/mL per 1 mg dose, resulting in a 31.03% bioavailability of compounded rapamycin relative to commercial rapamycin
It’s a really important study giving new data on levels, pharmacokinetics, product differences. Important also to consider CYP450 3A4 status of each individual since we all may be fast or slow metabolizers depending on this enzyme which would obviously affect the sirolimus levels and kinetics. They did a great job with this paper.
Was the compounded rapamycin in enteric capsules? If so, by decreasing gastric emptying time after taking the capsule it would be more bioavailable. Because it would be less time for stomach acid to break down the capsule.
Enteric delivery is not the issue here. Rapamune from Pfizer has no enteric coating.
The issue is the solubilization of the drug which requires advanced formulation.
So is the coating something that makes it more soluble? Could you expand a little more on that? Would it work to dissolve it in DMSO, then dilute and drink? Thanks,
I didn’t see this? Seemed rather linear to me that higher dose results in higher levels.
Certainly doesn’t follow simple 1/2 life pharmacokinetics.
And certainly doesn’t clear by 1 week post dose.
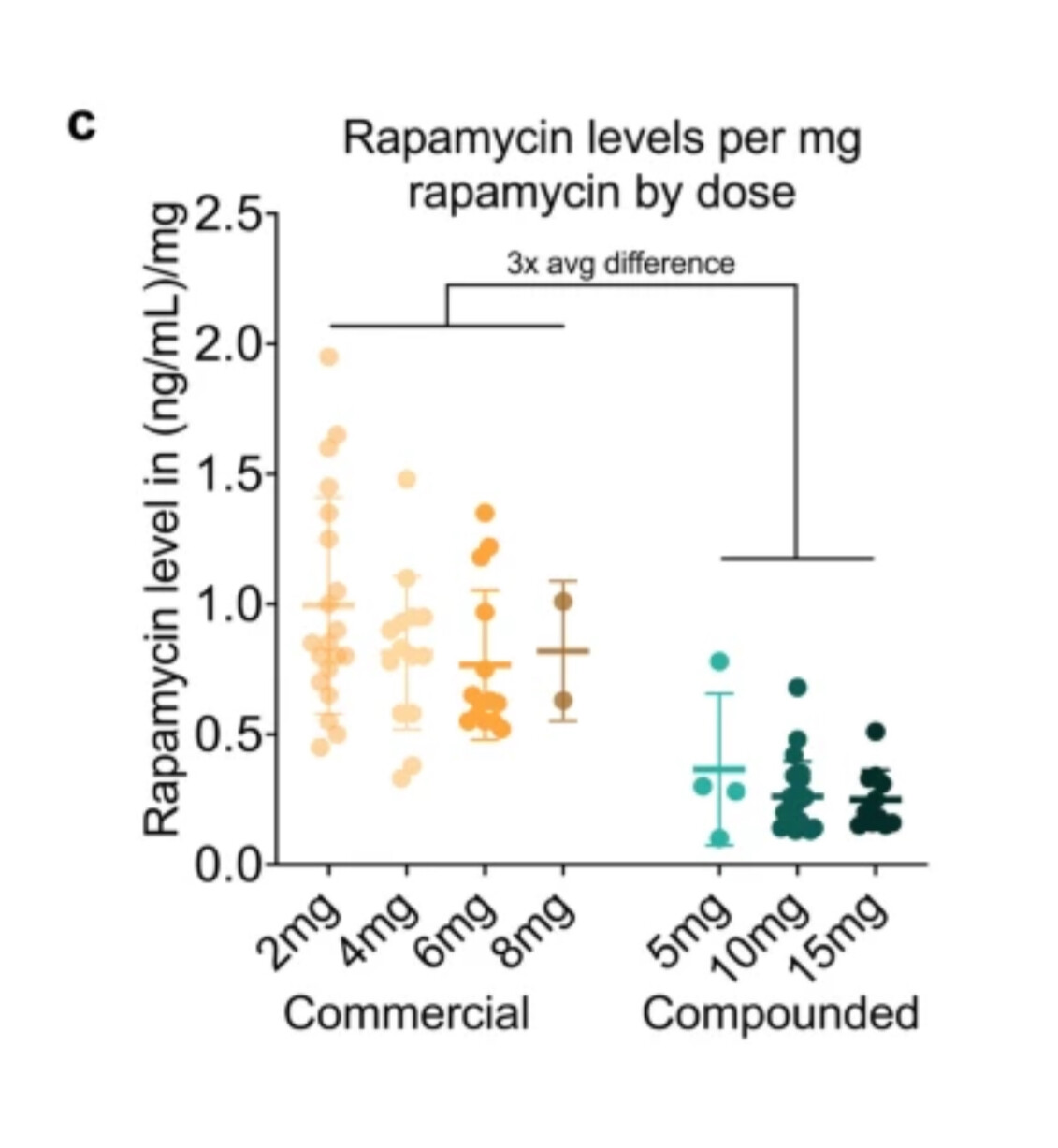
@KarlT This chart and table show diminishing increases in blood level per incremental mg dose of rapa. I’m only looking at the commercial data; I’m ignoring compounded.
Funny it goes down and bottoms out at 6 commercial and probably bottoms out at 18 compounded (3X). Then it goes back up. Maybe for low rates it goes into an organ or something, that gets full then it starts raising the blood levels again.
Thank you, okay so the issue is not stomach acid breaking down the rapamycin, this is quite some news. Not sure why I (and others) have been so mistaken about this.
I guess back to square one. If enteric coating is not any different than “film” coating in the Indian sirolimus generics as far as bioavailability goes, then where does that leave us insofar as dosing is concerned? Are these generics, the Biocon and Zydus ones from India equivalent to the compounded ones wrt. bioavailability? That would mean considerable dosage adjustments!
Ultimately, I think this must come down to measuring serum levels of sirolimus, regardless, and adjusting the Indian generics dose so that the serum levels hit Pfizer formulation levels whatever they may be, 3mg equivalent, 6mg equivalent and so on. Plus that would also adjust to the individual - Bob may need to take 6mg to hit the same serum level that Jim gets from 4mg, etc. at, say, 50 hours. Now, if only we were clear on what the effects of various levels were…
In turn, even the serum levels are not dispositive. We need “effects” or at least biomarker signifiers for beneficial effects, which may require different serum levels depending on the individual. But what are these signifiers? This is where we enter the realm of the anectdotal - “6mg/1-week resolved my frozen shoulder” etc.
Btw. I wonder if this is what the “e” rapa formulation for the mice in the ITP was developed for, and nothing to do with enteric coating🤷.