We all know that CR is a lifespan extending intervention, but also that it’s difficult to maintain compliance all over life, living on a -20/-25% CR.
Does anyone already did drugs intervention focused on increasing the compliance of living on a permanent CR?
I’m starting experimenting taking naltrexone + bupropione drug, a neuro drugs working in hypothalamus to reduce the sense of appetite.
I’m already on Acarbose (100mg morning, 100mg evening) and will soon add GLP-1 agonist and SGLT-2 inhibitor, completing the T2D anti-aging portfolio (before lowing LDL with Ezetemibe+Statin, being then ready to starts Rapamycin).
I’ve read GLP-1 agonist should reduce appetite too, also slowing down digestion such as Acarbose is doing.
Does anyone can share their experiencing in living on permanent CR and usings drugs to support achieving compliance without too much mental effort?
Mounjaro (A glp-1 and GIP) is really a miracle when it comes to appetite suppression. Makes CR a dream. I am taking it for its anti-inflammatory effects, but losing weight and have to remind myself to eat - which I do to ensure health, not from hunger The good thing is, that although it reduces food craving it hasn’t reduced the ability or pleasure of eating (when I remember to do it).
Great finding @Walter_Brown, if that’s the case probably naltrexone + bupropione would not be needed (Tought i’m finding some results of using it together) .
Do you have any previous experience of GLP-1 agonist only (No GIP), if it excert the same appetite suppression?
I ask so, because i’m not a needle fan, and would be better willing to take pills of Rybelsus as daily Semaglutide, along with my pills stack.
Btw it’s super exciting to know that’s possible to lives in structural CR with such a pharmacological tools, definitively super part of longevity intervention program by achieving high compliance!
My understanding from many papers is that maintaining a structural CR all over life is doable and beneficial to lifespan across all animal models.
I maybe wrong, but do you have different technical research/experimental references identifying that CR over life does lead to die of malnutrition?
Fabio, if you take the starting energy input as a fixed reference, then it’s possible to live in permanent CR, although it may bring about some side effects, like immunitary problems, glucose intolerance, bone and muscles frailty. I would refer you to the CR forum, where there is an ample repository on related threads and you can always ask where to search. Some CR veterans switched to less severe CR, enough to maintain a BMI of 20-22.
In this Rapamycin forum there are quite a few very interesting threads on GLP1-R agonists, both injected and Rybelsus, I’m aware that they can have side effects as well. I personally tried berberine and at 1000 mg/d there was a significant appetite suppression, such that I had to decrease to 500 mg/d, since I do not pursue CR. Taking a supplement may be worth a try before taking more effective drugs which however may impingenegatively on other mechanisms (such as heart rate).
Would taking enough calcium through diet or supplements and maybe weightlifting prevent the reduction in BMD? I cannot personally see the benefit of CR if it makes your bones weaker or if it can’t be prevented. That’s a no go for me then. Falling, snap hip in half, 50% risk of death within 1 year.
My fears are not diminished when long term CR proponents say they have that side effect.
AnUser, as far as I’ve seen, CR-ON, that is with optimal nutrition, paired with resistance exercise, should avoid problems of excessive frailty. People track what they eat and make sure they have calcium, plus they add supplements and should measure regularly BMD. A single CR practitioner made it clear he had osteoporosis but he is over 80 and used appropriate pharmaceuticals.
Of course, the skeletal muscles will shrink in size, that’s inevitable.
Another issue is how you compute a restricted calorie input when exercising. One of the practitioners used to eat 3000 kcals a day since he was moving around a lot. That is more than I eat without CR.
At the end, the recent evolution in CR is a moderate restriction, such that you remain in the range of 20-22, maybe a little less for people who are naturally very thin. This to sit in the optimum region of the J curve which assigns, according to some articles, a higher mortality below BMI 20.
Some authors like Luigi Fontana rationalize and give some evidence that even significant CR is good. Personally, I wouldn’t follow his suggestions, since this field hasn’t been much studied.
KarlT, I understand what you mean; evidently the concept of ‘calorie restriction’ is relative to the starting stage, the ‘normal’ amount of calories you ate before starting Cr. After you lost weight, you enter a steady-state bodyweight where you can no more restrict, unless you create an infinite process which will take to an infinitesimal bodyweight, which is impossible because prior to that, you are dead.
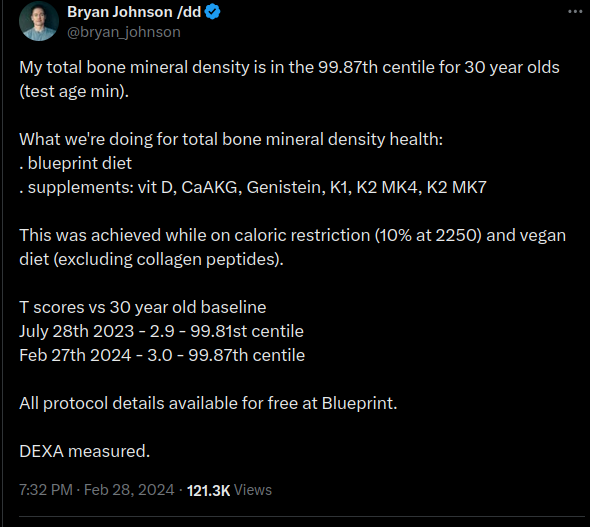
I take 1000 mg calcium supplement and 4000 iu Vitamin D at the moment.
I can replace a bit at least of the calcium with CaAKG, IIRC Brian Kennedy lab likes it. Genistein /K1/K2/MK4/K2 MK7 are interesting, anyone here knows something about those?
There’s a good part and a bad part to this. The good part is, that here’s an occasion to use Wolfgang Pauli’s excellent observation “this is not even wrong”. The bad part, is of course that the model used here is so catastrophically misaligned that it needs wholesale discarding.
You asked if someone here has been on CR - I’ve been interested in CR since the 80’s when Walford’s first diet book came out, and I went on CR for a number of years, successfully, before quitting for social and other reasons, which I’ve explained elsewhere on this site. I had no difficulty maintaining CR insofar as hunger.
More relevantly, there was a long time CR related list (even before the crsociety website existed), on which I was an active participant, where the participants shared a ton of research and which generated a lot of ideas and approaches. And what you are proposing fits right in with one of the biggest and long running discussions, the so called “Hunger Hypothesis”.
The Hunger Hypothesis, is the idea that the very thing that you are seeking to abolish, in order to make cutting calories, and thus practicing CR easier, is the thing that makes the benefits of CR possible.
Note that what you are doing is very risky from a scientific method point of view. You are ignoring the “black box” model and engaging in mechanistic speculation which almost always results in incorrect ideas of how things work, especially in biology. The black box approach is to look at inputs into the black box, and observe the outputs out of the black box and ignore (at least temporarily) what happens inside the black box. We can say this: based on animal studies cutting calories [input] results in longer life [output]. But you can’t now suddenly change the input and expect the same output, based on speculation of what happens inside the black box. Speculating on what happens inside the black box is the essence of mechanistic speculation.
What we observed: mice/rat/animal model given fewer calories resulted in - a longer life. Now you are changing the input, and you expect mice/rats/animal model given fewer calories, and with their appetite suppressed will result in - a longer life(??). Nope. This is not the same - the inputs have changed. Once you change the inputs, you must run the experiment again, to see if you get the same output. You speculated mechanistically that changing that aspect of the input (appetite suppression) is irrelevant to the inside of the black box, and you’ll get the same output. But you have no way of knowing if your speculation as to what the black box does (“it ignores appetite suppression”) is correct - that’s speculation. To know, you must observe - not assume - the outcome.
How CR works is part of what happens inside the black box. We have all sorts of ideas. And appetite - the sense of hunger with lower calories - is an integral part of the CR effect, because that is how the body operates signalling pathways. Part of the benefits of CR is hormetic, and a whole cascade of processes, the body senses there are not enough calories, so it uses them more efficiently, re-uses faulty cell components through autophagy, it rallies the body defence mechanisms to survive the caloric deficit, it sharpens the functionality of multiple systems - energy output, neurological efficiency, sense acuity - in order to allow the animal to find food. And how does all of it start? With the first step - signalling. The body must know that it is in a calorie deficit. One way it knows, is through sensing hunger - hunger is a signal in the body that there are not enough calories. This has consequences - there is a whole cascade of hormonal signals, gherlin and neuropeptide Y among them, that are feedback mechanisms with hunger.
To just look at neuropeptide Y - first, what it is, courtesy of our AI overlords - I’m using AI instead of chasing papers that I’ve explored decades ago, during the original discussion of the hunger hypothesis, as it’s faster:
"Neuropeptide Y (NPY) is a 36-amino-acid peptide that plays a role in many physiological and homeostatic processes in the nervous system:
Appetite regulation: NPY is a key regulator of appetite, stimulating food intake. NPY levels increase during fasting and exercise.
Stress and emotional behaviors: NPY is involved in regulating stress, anxiety, fear, and other emotional behaviors.
Energy metabolism: NPY regulates energy metabolism.
Immune system communication: NPY is a critical transmitter between the nervous system and immune system.
Blood pressure: NPY plays a role in controlling blood pressure.
Other physiological processes: NPY is involved in other physiological processes, such as learning and memory.
NPY is found in the central nervous system (CNS), sympathetic ganglia, and extra-neuronal tissues like the lung urinary tract, spleen, blood vessels, and reproductive organs"
Neuropeptide Y is elevated in hunger:
"Yes, neuropeptide Y (NPY) is considered elevated when someone is experiencing hunger, as it is a potent neurotransmitter in the brain that stimulates appetite and food intake, essentially signaling the body to eat when energy stores are low; its levels tend to rise during fasting or when experiencing calorie deficit.
Key points about NPY and hunger:
Function:
NPY primarily acts in the hypothalamus, a region of the brain that regulates appetite, and when activated, it triggers a strong urge to eat by increasing meal size and decreasing the feeling of satiety.
Regulation by energy status:
When energy levels are low (like during fasting), the production of NPY increases, leading to increased hunger signals.
Opposite effect of leptin:
Leptin, a hormone released by fat cells, acts as a satiety signal and can suppress the release of NPY."
_Neuropeptide Y is neuroprotective:
" Yes, neuropeptide Y (NPY) has neuroprotective properties:
Reduces neuroinflammation: NPY can reduce neuroinflammation.
Increases BDNF levels: NPY can increase the levels of BDNF and NGF.
Stimulates autophagy: NPY can stimulate autophagy.
Reduces oxidative stress: NPY can reduce oxidative stress and mitochondrial dysfunction.
Decreases glutamate-induced excitotoxicity: NPY can decrease glutamate-induced excitotoxicity.
Inhibits caspase-3 and caspase-4 activities: NPY can inhibit caspase-3 and caspase-4 activities.
NPY is a neurotransmitter or neuromodulator that plays a role in regulating physiological processes. NPY levels are altered in some neurodegenerative and neuroimmune disorders. NPY’s neuroprotective properties are mediated through the activation of Y1, Y2, and/or Y5 receptors."
And that’s just neuropeptide Y. There are so many others - all you have to do is look at the fasted state and the dramatically different signalling pathways activated as a result of this state.
Now you are proposing to not inform the body that it is in a state of caloric deficit. You are essentially, through chemical means, stopping the signalling pathway of hunger. Guess what. You are not going to experience the same results. It’s like not knowing how much you have in your bank account [how many calories]. If you do know, and are approaching zero funds, you are sent an alert [experience hunger], so you can now take actions [CR benefits] hoping to make more money, get a job [energy output], get an education, cut expenses [autophagy]. If someone stopped you getting the alert (hunger), you will lose your money (cut calories), but you will not know to get a job, an education or cut expenses, and you’ll just go bankrupt, no benefit of CR, instead harm. CR without hunger may be not only not beneficial, but harmful.
Here is an interesting fact - the signalling pathways are so powerful that they can abolish benefits of CR. How do we know that? Because we have hints of it in studies showing that in f.ex. fruit flies, merely sensing that food is around, abolishes most CR benefits. They don’t even need to eat more to abolish CR benefits - all they have to do is sense that food is around:
When you make a massive intervention like GLP-1RA agonists or some agents that suppress appetite, you are really messing around with the physiology of the body. There are consequences to that. You cannot get away with changing the inputs and expect the same output.
I therefore have to say, you must completely re-think your approach to science to account for the black box model in situations where we don’t fully know how a drug or intervention (like CR) work. Any - any - change in the intial conditions must be tested for outcomes. You cannot assume anything.
Interesting observations and conceptually right. Does CR without Ghrelin and Neuropeptide Y has the same effects as CR with these hormones? It may be so, it may be not. We really don’t know.
However, it may be that we accept a state of ignorance and adopt a strategy that assigns by hypothesis a greater sensitivity to the intra-cellular decrease of nutrients rather than to the presence of ghrelin and NPYs.
In a few words, we may hypothesize that ingested nutrients rule over the ghrelin-NPYs signal.
My concern is rather that we don’t really know the chronic effects of GLP1-RA in an individual on CR.
Besides, we don’t know the poster’s age and the other boundary conditions, like overall health, biomarkers, exercise and so on. It may even be that CR is not advised at all.
Perhaps GLP-1 analogs don’t necessarily reduce grehlin levels, but may just counteract (some of) grehlin’s effects, such as its appetite-stimulating effects. It appears we don’t know yet.
But this study CT posted (‘Researchers Find Link Between Food Odors And Lifespan In Fruit Flies’) I’ve also seen years ago, and it’s one of many studies that should make anyone interested in the potential benefits CR(ON) and the use of GLP-1 analogs pause.
Natural Supplements such as Bitter gourd extract in Coconut Nut cold pressed oil has significant reduction of Apetite for many. I dont have any data one can study further.