I’m continuing my deep dives into the genetic pathways to get actionable insights as the previous ones have been incredible precise and useful. This time I’m looking at strength training genetic pathways.
Here is the general description of the pathways and their variants. I will put the finding about my own genome below it as an example of what useful and actionable insights you can get.
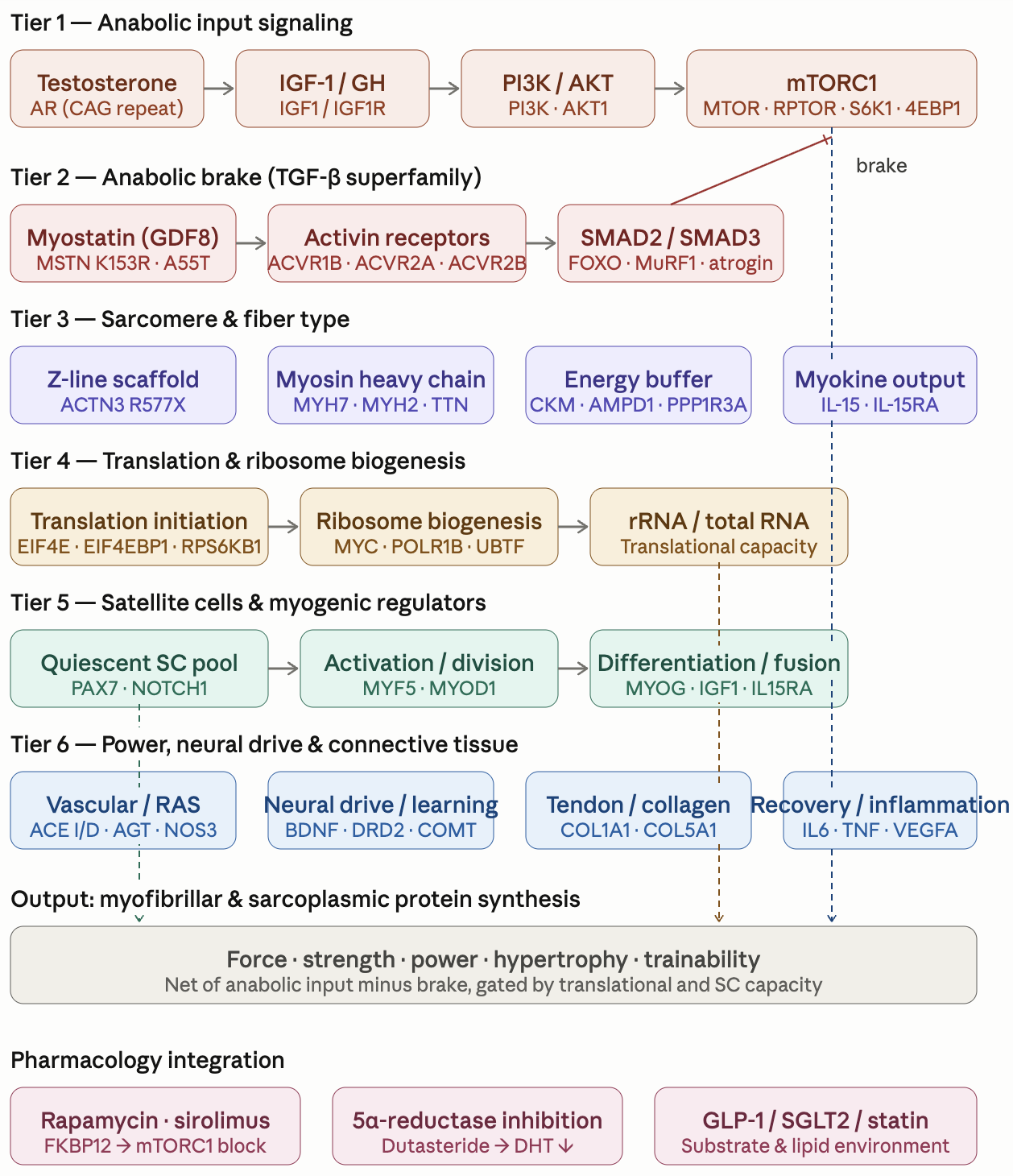
Strength_Hypertrophy_Power_Genetic_Pathway_Reference.pdf (467.6 KB)
The pdf report above is valid for everybody but here is the summary of the findings I get when I apply it to my own genome.
Strength, Hypertrophy & Power — Top 10 Findings & Action Items
The headline
The strength/hypertrophy/power profile is strongly favorable on the canonical power axis (likely ACTN3 R/R, likely MSTN K/K, likely AMPD1 C/C, AR ≥21 CAG repeat inferred, balanced ACE I/D) and on the neural-drive layer (likely BDNF Val/Val, likely DRD2 Glu/Glu, likely COMT Val/Val), but carries two consequential homozygous-variant convergences — a connective-tissue / tendon-injury haplotype (COL5A1 T/T at both queried SNPs + COL1A1 GT high-risk genotype + COL3A1 A/A + MMP3 K/K) and a complete VDR signaling-block (FokI G/G + BsmI/ApaI/TaqI homozygous haplotype) — plus the cross-report rapamycin × resistance-training timing question that this profile makes more consequential than population baseline.
1. Time the existing 15 g collagen + 500 mg vitamin C to 30–60 minutes pre-training
The COL5A1 T/T at both rs12722 and rs13946, COL1A1 GT heterozygous (highest-injury-risk dose-response genotype per Lulińska-Kuklik 2018), COL3A1 A/A homozygous, and MMP3 K/K homozygous convergence puts the connective-tissue / tendon-injury risk meaningfully elevated. Per Shaw 2017 (Am J Clin Nutr), 15 g hydrolyzed collagen + 50 mg vitamin C taken 30–60 minutes pre-tendon-loading exercise produced a 2× increase in collagen synthesis biomarker (PINP) vs random timing. The 15 g collagen is already in your AM stack — confirming and adjusting the timing to be ~45 minutes pre-training (rather than just any time of day) is the lowest-cost, highest-leverage intervention in this report. If multiple training sessions per day, re-dose pre-each-session.
2. Increase Avmacol Extra Strength to 2 caps/day (or add a stabilized sulforaphane source)
Already flagged HIGH in the Endurance report for the NFE2L2 −617 homozygous promoter variant (verified). The strength context reinforces: high-volume resistance training generates more training-induced ROS than the moderate-aerobic baseline assumed there, and the constrained NRF2 inducible response limits adaptive antioxidant upregulation. Doubling Avmacol or adding a stabilized sulforaphane preparation (target 30–60 mg sulforaphane equivalents/day, well within Ahn 2022 / Sedlak 2018 ranges) is the highest-priority supplement increase across the integrated profile.
3. Rapamycin-aligned resistance training schedule: protect days 0–2 post-dose; concentrate hypertrophy work on days 7–14
Drummond 2009 (J Physiol, n=14) showed acute rapamycin completely blocks the contraction-induced ~40% rise in muscle protein synthesis. Your profile amplifies the impact: homozygous AKT1, homozygous MTOR (Rapamycin report), heterozygous FOXO3 longevity haplotype (IGF-1 report) all unmask the catabolic/autophagic program more strongly than population baseline during rapamycin peak-to-mid-trough. Concrete schedule: avoid heavy resistance training within ±4 hours of dose; light-to-moderate work days 1–2; main hypertrophy window days 7–10; main strength window days 11–14. Track lean-mass trajectory via DEXA every 6 months; adjust if unfavorable.
4. Add β-alanine 4–6 g/day (divided 1.6 g × 3–4)
Already flagged HIGH in the Endurance report for the SLC16A1 T/T MCT1 lactate-shuttle limit. The strength context reinforces: hypertrophy-rep-range training (8–12 reps with short rest) accumulates intramuscular H+ that limits repeat-set output. β-alanine drives muscle carnosine accumulation for intramuscular H+ buffering. Loading: 4–6 g/day for 4–10 weeks; tingling (paresthesia) is harmless and disappears with smaller divided doses.
5. Discuss vitamin D3 titration to maintain 25(OH)D in the 50–60 ng/mL band
Current 25(OH)D 84.6 ng/mL on Labcorp 01/07/2026 is HIGH (typical target 40–60; 80+ approaches concerns about hypercalcemia and possible adverse cardiovascular signals — Durup 2015 J Clin Endocrinol Metab; Dror 2013 PLoS One). With homozygous VDR signaling-block at all four queried sites (FokI G/G + BsmI T/T + ApaI A/A + TaqI G/G), the receptor is rate-limiting, not the substrate. Titrating D3 to 2000 IU q.o.d. or 5000 IU twice weekly preserves saturated VDR signaling without high-end risk. Discussion point with treating physician.
6. Eccentric loading included routinely — but with 60–70% the rate-of-progression of population guidance
Heavy slow eccentrics for the Achilles, patellar, and supraspinatus tendons are gold-standard tendinopathy prophylaxis and rehabilitation (Alfredson protocols, Heavy Slow Resistance training). The COL5A1 T/T + COL1A1 GT + COL3A1 A/A + MMP3 K/K convergence argues for routinely including eccentrics but progressing volume and intensity more conservatively than for an average genotype. Specific tendon warm-up (10–15 min zone-1 aerobic + 2–3 ramp-up sets at 50–60% 1RM) before working sets becomes more important than for population baseline.
7. DEXA scan baseline + every 6 months
Phenotypic readout for the rapamycin × training timing hypothesis (item 3) and the anabolic-vs-catabolic tension (homozygous AKT1/MTOR anabolic vs heterozygous FOXO3 longevity haplotype). Lean-mass trajectory across 6-month windows is the meaningful confirmation of whether the rapamycin-aligned training schedule is preserving / building lean mass. If lean-mass loss is detected, the dose-day-relative training timing can be adjusted (most likely: shifting heavy work further into days 10–14).
8. Discuss melatonin reduction from 5 mg to 1–3 mg evening
Already flagged across Glucose and Rapamycin reports. The strength context adds urgency: high-dose evening melatonin can mildly disrupt deep sleep architecture, and sleep is the single most powerful single recovery intervention for the bottleneck-4 recovery convergence (IL6 G/G high-producer + NFE2L2 hom + VEGFA hom + connective-tissue convergence). The genetic recovery limits make sleep-quality protection particularly important. 1–3 mg is the longevity-protocol standard.
9. Increase NACET to 300–500 mg total daily (currently 200 mg)
Per Endurance report, current NACET 200 mg total is on the low end for the NFE2L2 hom + multi-point GSH-pool pressure profile (cross-ref Glycation report’s CTH hom + AKR1B1 hom + GLO1 hom). The strength context adds the high-volume-training oxidative load. Bringing NACET to 300–500 mg total is well within standard supplementation ranges (clinical NAC trials use 600–1800 mg/day).
10. Routine ferritin, TSAT, sTfR, reticulocyte hemoglobin at next draw
Already flagged HIGH in the Endurance report. The strength context reinforces: TMPRSS6 V/V hom (Endurance report) raises hepcidin set-point and lowers iron absorption; IL6 −174 G/G high-producer (this report + Endurance + Inflammation) acutely shuts down iron absorption for 6–12 hours post-exercise. Reticulocyte 1.4% on Labcorp 01/21/2026 is at the low end for an active person. Ferritin baseline before any training-volume escalation; if oral iron is added, AM only, on empty stomach, with vitamin C, AT LEAST 60 minutes before any training.