Circadian, homeostatic, architectural, autonomic, and breathing genetics of sleep
I’m continuing my deep dives into the genetic pathways to get actionable insights as the previous ones have been incredible precise and useful. This time I’m looking at the sleep related genetic pathways.
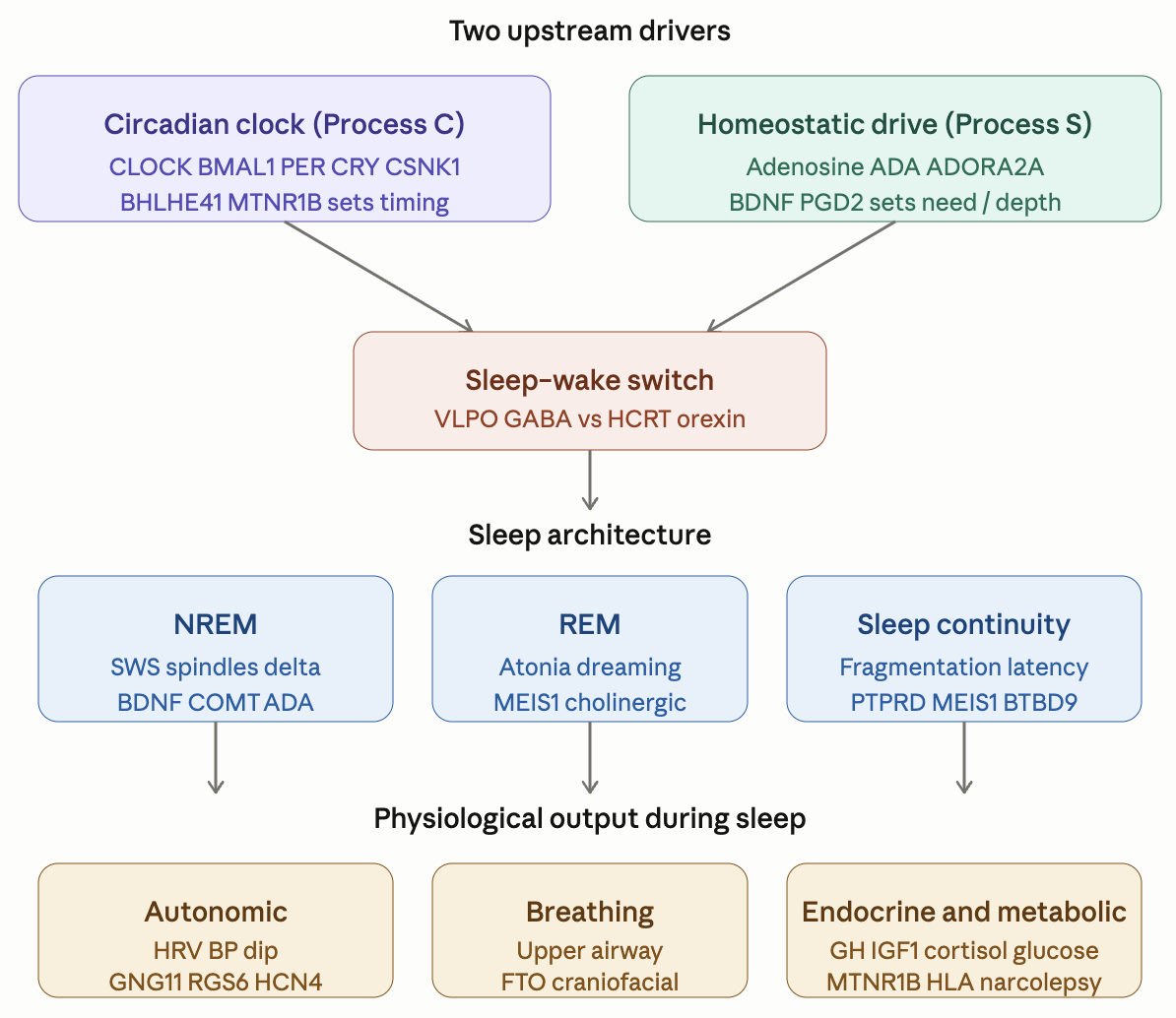
Here is the general description of the pathways and their variants. I will put the finding about my own genome below it as an example of what useful and actionable insights you can get.
Sleep_Genetic_Pathway_Reference.pdf (619.4 KB)
The pdf report above is valid for everybody but here is the summary of the findings I get when I apply it to my own genome.
Top 10 actionable findings
1. HLA-DQB1*06:02 NEGATIVE — narcolepsy NT1 risk at population baseline ✓
Both tag SNPs (rs9271117, rs2858890) absent in VCF and BAM pileup confirms reference at both positions (28 and 32 reads, all REF). Effectively excludes the haplotype that drives ~98% of NT1 cases. No action required.
2. BMI-INDEPENDENT OSA SUSCEPTIBILITY — recommend baseline sleep study 
NACA rs2958127 het + rs4759254 het + ABCC9 rs2074312 het + LPAR1 rs7030789 hom. FTO and MC4R both clean → BMI-mediated OSA pathway absent, but the residual signal is structural/neuromuscular. Recommendation: home sleep apnea test (HSAT) or in-lab PSG at age 62 even without classical risk factors. Highest-yield single investigation in this report.
3. RLS/PLMS susceptibility — check ferritin
BTBD9 rs9296249 het + rs9357271 het. MEIS1 and PTPRD both absent (major mitigators). Recommendation: ferritin, TSAT, sTfR — target ferritin >75 ng/mL (AASM 2025 threshold). Already recommended in Endurance/Strength reports for unrelated reasons; sleep panel reinforces. Not currently in recent labs.
4. Caffeine sleep-disruption convergence — strict noon cutoff
CYP1A2 rs762551 C/A (intermediate-slow metabolizer) + ADORA2A haplotype risk (rs2298383 het + rs4822492 het + rs2236624 hom + rs5751876 het) + NAT2 rs1799929 hom slow + ADA absent (no compensating clearance). Recommendation: all caffeine sources before noon. CacaoVia 750 mg AM is correctly timed — do NOT move later (theobromine half-life 7–12 h).
5. Melatonin dose — discuss step-down 5 mg → 1–3 mg
MTNR1B rs10830963 ABSENT (matches Glucose report) — no glucose-misalignment risk at any dose. CLOCK rs1801260 absent — no eveningness amplification. No specific genetic argument for high dose. Cross-report consensus (Strength, Glycation, sleep-genetic): supraphysiologic dose. Discuss step-down.
6. ADRB1 Gly389/Gly389 hom — β-blocker pharmacogenomics flag
rs1801253 G/C homozygous variant → blunted β1-AR signaling and blunted β-blocker response (Sofowora 2003; Liu 2003). No β-blocker currently in regimen. If antihypertensive intensification ever needed: prefer nebivolol or bisoprolol (β1-selective) over carvedilol or metoprolol; expect blunted response regardless. Telmisartan 80 mg evening is a well-aligned current choice.
7. Favorable autonomic profile — confirm with 24-h ABPM ✓
GNG11 rs10921075 hom + RGS6 rs4899412 hom — both higher-HRV alleles per Nolte 2017 Nat Commun. Predicts good vagal tone in NREM and deep nocturnal BP dipping. KIAA1755 hom partially offsets. Recommendation: 24-h ambulatory BP monitoring to verify dipping is preserved and confirm telmisartan 24-h coverage.
8. All rare Mendelian sleep variants ABSENT ✓
PER2 S662G (FASPS1), BHLHE41 P384R (FNSS1), CRY1 c.1657+3A>C (familial DSPD), CSNK1D T44A (FASPS2) — all clean. No FASPS, no familial natural short sleep, no familial DSPD. Strongly favorable.
9. Sleep supplement stack genetically well-aligned ✓
-
Mg L-threonate 2000 mg PM — BBB-penetrant (Slutsky 2010); supports COMT Val/Val EEG profile
-
Glycine 6 g PM — direct sleep-onset evidence (Yamadera 2007; Bannai 2012)
-
L-theanine 200 mg PM — aligns with FKBP5 het cortisol-axis finding
-
Phosphatidylserine 300 mg PM — cortisol-blunting, FKBP5-aligned
-
Lithium orotate 5 mg PM — modest circadian-stabilizing
No changes recommended. Continue.
10. Favorable duration/architecture predisposition ✓
PAX8 rs1191685 hom (sleep-extending allele, ~+5 min predicted) + KCNK9 rs2542425 het + rs888346 het (mildly NREM-extending, ~+2 min combined). FTO absent removes BMI-mediated short sleep risk. CRY2 hom protective. No FNSS/short-sleep signal.